We see an increasing number of people in their 20s in our forums who have started using rapamycin, including this 24 year old PHD student who is posting on his personal rapamycin trial. And a 30 year old MD who describes his rapamycin regimen and his rationale behind it. Additionally, women in their early 30s and early 40s are increasingly turning to rapamycin to maintain their health and fertility.
And we see even younger people. Below we see that 21 year old Thiel Fellow Ben Nashman has started rapamycin. Read on to see some of the research that is driving these types of decisions.
One of the leading researchers in the rapamycin area, Dr. Blagosklonny, suggests people should start rapamycin at 25:
Lifespan Benefits of Starting Rapamycin Younger
The scientific evidence suggests that total healthspan and lifespan may be optimized when a person starts rapamycin in their late 20s or early 30s, rather than in their 40s, 50s or 60s; the more common age range among rapamycin users.
In animal studies, rapamycin has been shown to be effective at increasing healthy lifespan when usage is started either in early adulthood (e.g. equivalent to about 30 years in human terms) or middle age (equivalent to about 60 in human terms), but the longest lifespans achieved in studies so far are when rapamycin is started in earlier adulthood.
In the National Institute on Aging’s ITP studies, the longest lifespan improvements have been in young adult mice (who started taking rapamycin at age 9 months, equivalent to about age 30 in people) where they saw a 23% (male) and 26% (female) median lifespan improvement. This compares the study where they did not start giving rapamycin to the mice until middle-age (20 month old, equivalent to about 60 in human terms) and the study saw a median lifespan improvement of only 11% (m) and 15% (f) using the same dose (source). As they state in the research paper “it may be that this Rapamycin dose is more effective when given starting earlier in adult life”. To the best of my knowledge, the 26% median lifespan improvement in female mice are the best results seen to date for a single longevity drug (rapamycin) study by the National Institutes on Aging.
Some researchers are suggesting with optimized dosing schedules determined through rigorous rapamycin clinical studies may be able to increase human lifespan by 30 years. In fact, new 2022 results recently announced in an interview with Richard Miller of the National Institutes on Aging, Interventions Testing Program showed the longest lifespan extension ever achieved in their tests; a 29% lifespan increase for male mice that are fed rapamycin and Acarbose starting in early adulthood.
Changes in many measures of aging start getting worse (ramping up) as young as age 26, as this graph below demonstrates:
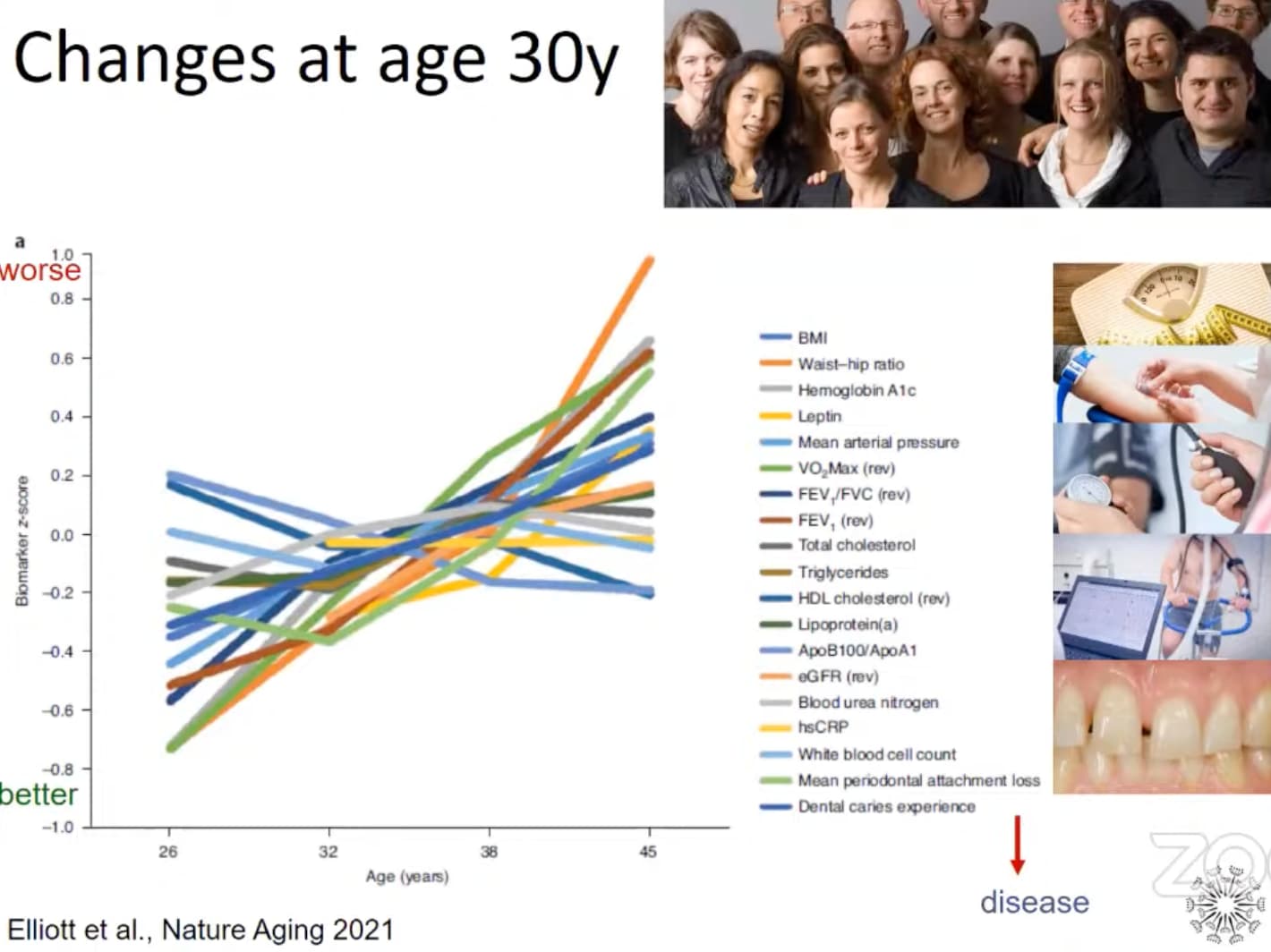
Source: Disparities in the pace of biological aging among midlife adults of the same chronological age (Nature Aging, 2021), Full Paper PDF, Video Discussion
There are many cases where rapamycin does a better job at protecting functionality from aging if you start it earlier rather than later. It is true that in many research studies we see a reversal of function back to a younger functional state (e.g. ejection fraction in the heart studies - returning to a more youthful profile), but I suspect that if we look more closely and at more functional outcomes we would see rapamycin is better, in general, at “preserving” functionality during aging (and therefore increasing healthspan) compared to the reversal of aging, and improvement of function that has been lost.
If this is the case perhaps the best strategy may be to start a low dose (e.g. 3mg / week) earlier in life - say when people are at their peak physical condition (say 27 years old, for example). And perhaps the argument for earlier young adult use of rapamycin is stronger for females than males because female fertility decreases much faster than male fertility.
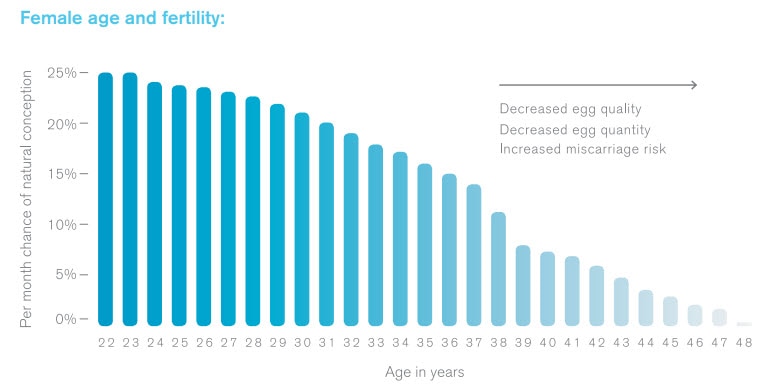
Fertility
In terms of female fertility, there is already strong evidence in mice and rats that rapamycin delays (reverses?) reproductive aging in females.
Geroscience researcher Matt Kaeberlein said recently that he was at a June 2022 conference on reproductive aging and there were 3 or 4 presentations related to rapamycin and/or mTOR studies on ovarian aging. He notes that he saw a rapamycin/mtor presentation where:
“they had remarkable pictures with old mice with atrophied ovaries, and then you look at an old mouse that had been treated with rapamycin and the ovaries look like young ovaries from a young mouse.”
You can listen to his comments yourself; I’ve positioned the video in this link to the exact spot where reversing ovarian aging / function is discussed, here: Targeting aging with rapamycin: On the path toward 21st Century Medicine - YouTube
Here are some of the academic research studies that report this benefit:
- Short‐term rapamycin treatment increases ovarian lifespan in young and middle‐aged.
- Rapamycin can preserve the developmental potential of eggs.
- Rapamycin can maintain the developmental potential of eggs (full paper, PDF)
- Rapamycin keeps the reproductive clock ticking.
- Rapamycin prolongs female reproductive lifespan.
- Effect of caloric restriction and rapamycin on ovarian aging in mice
The inhibition of mTOR signaling can also prolong ovarian lifespan. Compared to that in control rats, rapamycin-treated rats have a 2-fold increase in the number of primordial follicles after 10 weeks of treatment with rapamycin (5 mg/kg every other day, i.p.) (17, 111). These results indicate that rapamycin can protect the ovarian reserve and extend ovarian lifespan. An interesting experiment also showed that a transient 2-weeks regimen of rapamycin facilitates the sufficient extension of ovarian lifespan in mice regardless of the age at treatment initiation. Source: Frontiers | Role of mTOR Signaling in Female Reproduction
[Note: other compounds like Ca-AKG, NMN and Resveratrol seem to also help with preservation of fertility (sources: 1, and 2 and 3 (resveratrol)). Here, a couple of anti-fibrotic drugs (pirfenidone and BGP-15) restored ovulation in reproductively old mice. So perhaps an ideal approach would be to combine these supplementation approaches.]
There are researchers who argue that rapamycin effectively “slows down time” from a biological growth and development perspective - while maintaining that potential for growth in the future. I’ve spoken to some academics at major US universities that are planning more studies focused on rapamycin and human fertility so its an area ripe for more research, but the preliminary evidence is very encouraging. It was announced in mid-2022 that researchers at Columbia University in New York have initiated a human clinical trial to duplicate the rapamycin fertility trials done in mice and rats, but now in women. It seems to me that preservation of fertility is easier and more likely than reversal of fertility loss, but of course, I could be wrong.
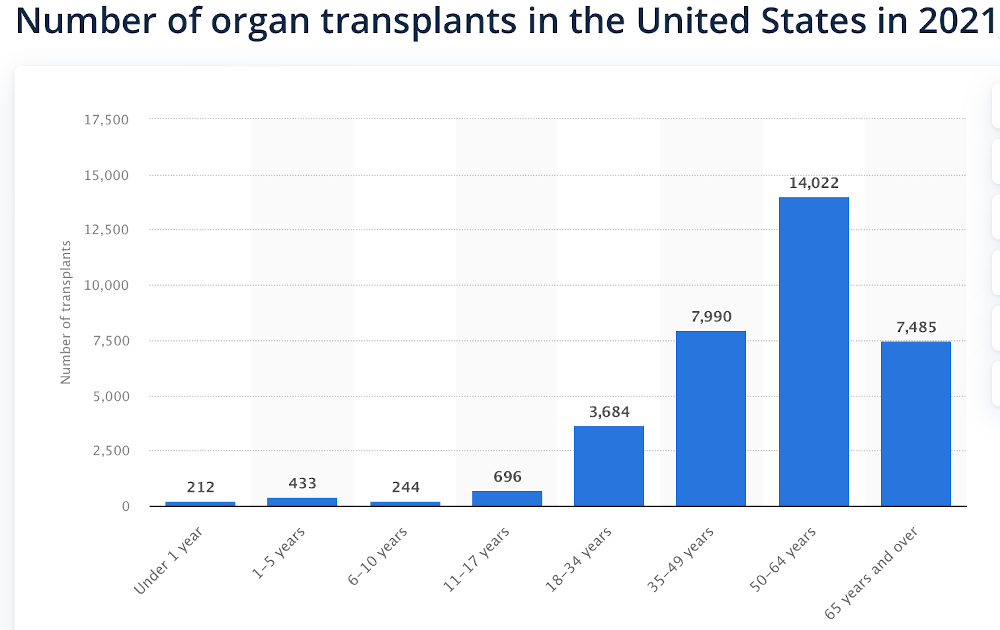
There would, however, be some unique risks I think, associated with being a younger female using rapamycin. Probably the biggest concern would be if a woman were to get pregnant when they are on rapamycin. There is not much research on this - but since rapamycin shuts down mTOR, which is a key growth signal in the body, there could be serious and very negative impacts on any developing fetus (see this study for example) - so a woman would want to work closely with her doctor on this, and really want to be careful about being sure they are off rapamycin for a few months (or more) before thinking about having babies.
I would also argue that the medical profession has been dealing with the risk of rapamycin use / mTOR inhibition and potential pregnancy for the past 20+ years with rapamycin in transplant patients (as long as rapamycin has been used in this application) and there is not that much difference with it going forward in an anti-aging application with people of this age group. Something like 20% of organ transplant patients are under the age of 40 and a significant number (I believe) have had children, so this is a challenge that the medical profession seems to have managed for the past 20+ years already.
If the results in humans are as good as the studies in animals, the cost/benefit for rapamycin is very compelling. The typical cost of rapamycin for anti-aging doses is approximately $40 to $120 per month (for the years of use) vs. the cost for a woman to freeze her eggs (in addition to the hassle and pain of doing so) is approximately $7,000 plus ongoing long-term storage costs.
Menopause
If rapamycin is slowing fertility declines, then it suggests that it might also delay or prevent menopause. And while there is no research on this published that I can find, there are annecdotal reports that people are seeing this:
One Report:
I have been taking rapamycin for 6 months on and off. It has improved my hdl and ldl ratio to the point where my hdl is now higher than my ldl. I have also been giving it to my mother who is 63 years of age. She rather unwillingly told me that she has been having her period again for the first time in 14 years.
Another report:
Age-related Erectile Dysfunction
Rapamycin has been shown in several studies (mice and humans) to delay, and reverse erectile dysfunction. A study has even been done that identifies the mechanism of action (see: Rapamycin Improves Erections).
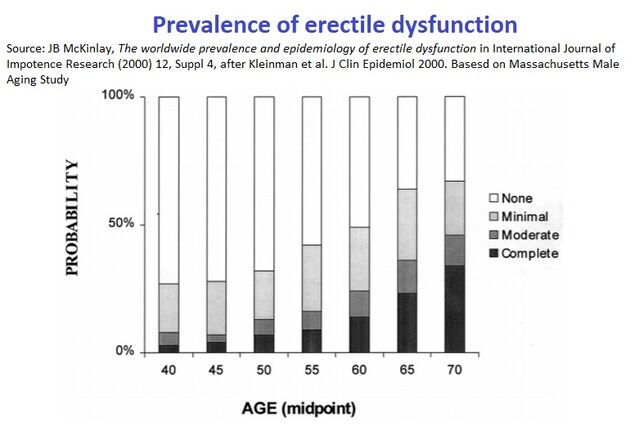
In the ResTORbio clinical studies of their mTOR inhibitor in healthy older humans, it has been reported that “one of the strongest reported “side effects” of the mTOR inhibitors from the resTORbio RCTs was an increase in morning erections”.
Several studies accessed the prevalence of erectile dysfunction (ED). The Massachusetts Male Aging Study reported a prevalence of 52%.2 The study demonstrated that erectile dysfunction is increasingly prevalent with age: approximately 40% of men are affected at age 40 and nearly 70% of men are affected at age 70. The prevalence of complete erectile dysfunction increased from 5% at age 40 to 15% at age 70.2 Age was the variable most strongly associated with ED.
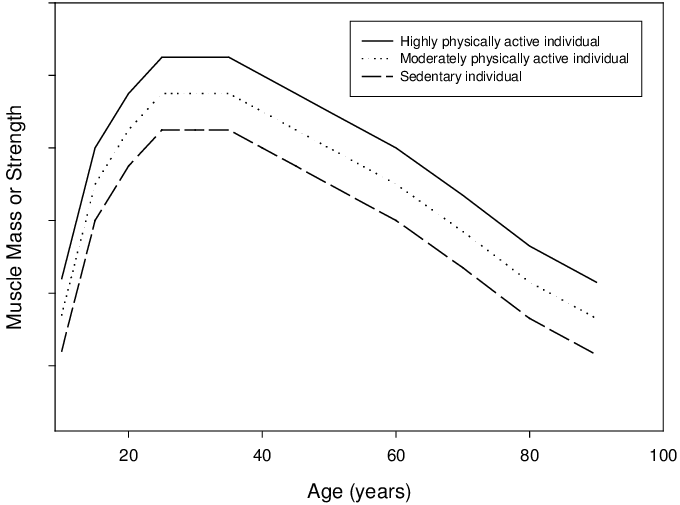
Muscle Function
Additionally, studies indicate that rapamycin can preserve muscle function (important for men and women) much longer if you start earlier rather than later.
Here are some such studies that report this benefit:
- Rapamycin protects aging muscle (2019 Research Paper)
- Rapamycin Rescues Age-Related Changes in Muscle-Derived Stem/Progenitor Cells from Progeroid Mice
- Rapamycin rescues mitochondrial myopathy via coordinated activation of autophagy and lysosomal biogenesis
- Age-related muscle loss: Study finds rapamycin may delay sarcopenia; diet, exercise key to minimise decay
I’ve seen some estimates that muscle function starts to decline in sedentary people in their late 20s.
Obesity Prevention
Another argument for rapamycin earlier in life is the trend for people (especially in the USA, but increasingly all around the world) to gain excessive weight as they get older, and it really starts ramping up after age 25, as this graph below shows (this graph is for only one state, but it seems likely to be representative for most states in the USA).
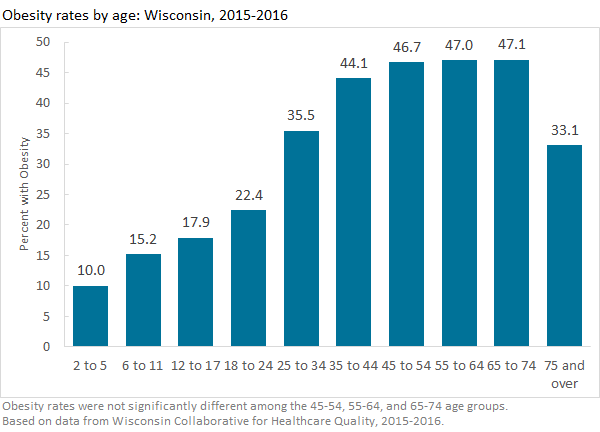
Two studies have shown that rapamycin can prevent obesity in mice fed high fat diets. Matt Kaeberlein stated in a recent twitter post: “we show in this paper that rapamycin prevents diet induced obesity in mice and activates CEBP/b target genes”.
Even in people that are not gaining a lot of weight, rapamycin may be of significant value. After age 25 people also start to gain visceral fat, the fat that wraps around your abdominal organs deep inside your body. You can’t always feel it or see it, but it contributes significantly to many health problems. Visceral fat is more likely to raise your risk for serious medical issues. Heart disease, Alzheimer’s, type 2 diabetes, stroke, and high cholesterol
In unpublished data, it has been stated that the reason the PEARL trial for rapamycin in humans chose visceral fat loss as the primary endpoint is because one of its collaborators, Dr Watson, had previously done a very small Rapamycin trial and the biggest effect he saw was a reduction of visceral fat on DEXA scan.
Stem Cell Aging
In this MIT Blood Stem cell study the rapamycin prevented the blood stem cells from aging if they started treatment early in life but it did not rescue them if started later.
When the researchers treated mice with rapamycin, beginning at a young age, they were able to prevent blood stem cells from enlarging as the mice got older. Blood stem cells from those mice remained small and were able to build blood cells like young stem cells even in mice 3 years of age — an old age for a mouse.
Our data indicate that rapamycin prevents the enlargement of HSCs and thereby protects them and potentially other stem cells from aging. However, rapamycin does not restore HSC function once they are large.
Hearing
Similarly - there is research suggesting that rapamycin can stop hearing loss almost completely if you start it early, but it can only slow down hearing loss if started later in life. Here is that study on rapamycin and hearing loss.
Here is some information on how people’s hearing declines with age:

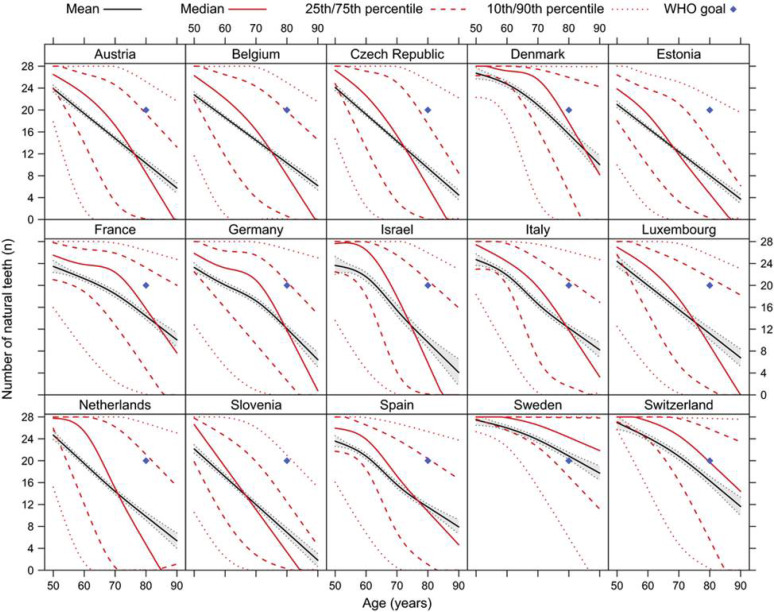
Oral Health
There is also the issue of dental and oral health. Having your teeth is really important - and rapamycin can do a lot to improve oral health and even bone growth, but there is no research suggesting it will grow your teeth back. However, it seems potentially realistic that rapamycin may help people keep their teeth and maintain their oral health much longer if they start rapamycin before they develop any teeth / oral health issues. A good article related to rapamycin and oral health is here: Longevity probably starts with a nice smile. A story about rapamycin and gum disease, an age-associated disorder
A new study has been funded with approximately $300,000, and initiated at the University of Washington, to see if direct application of rapamycin on teeth and gums can prevent periodontal disease, see: New Study Funded: Towards reversing periodontal disease using Rapamycin
Here is a graph showing how oral health (tooth loss, specifically) is seen around the world (I’d like to know what Sweden is doing with their teeth - impressive!):
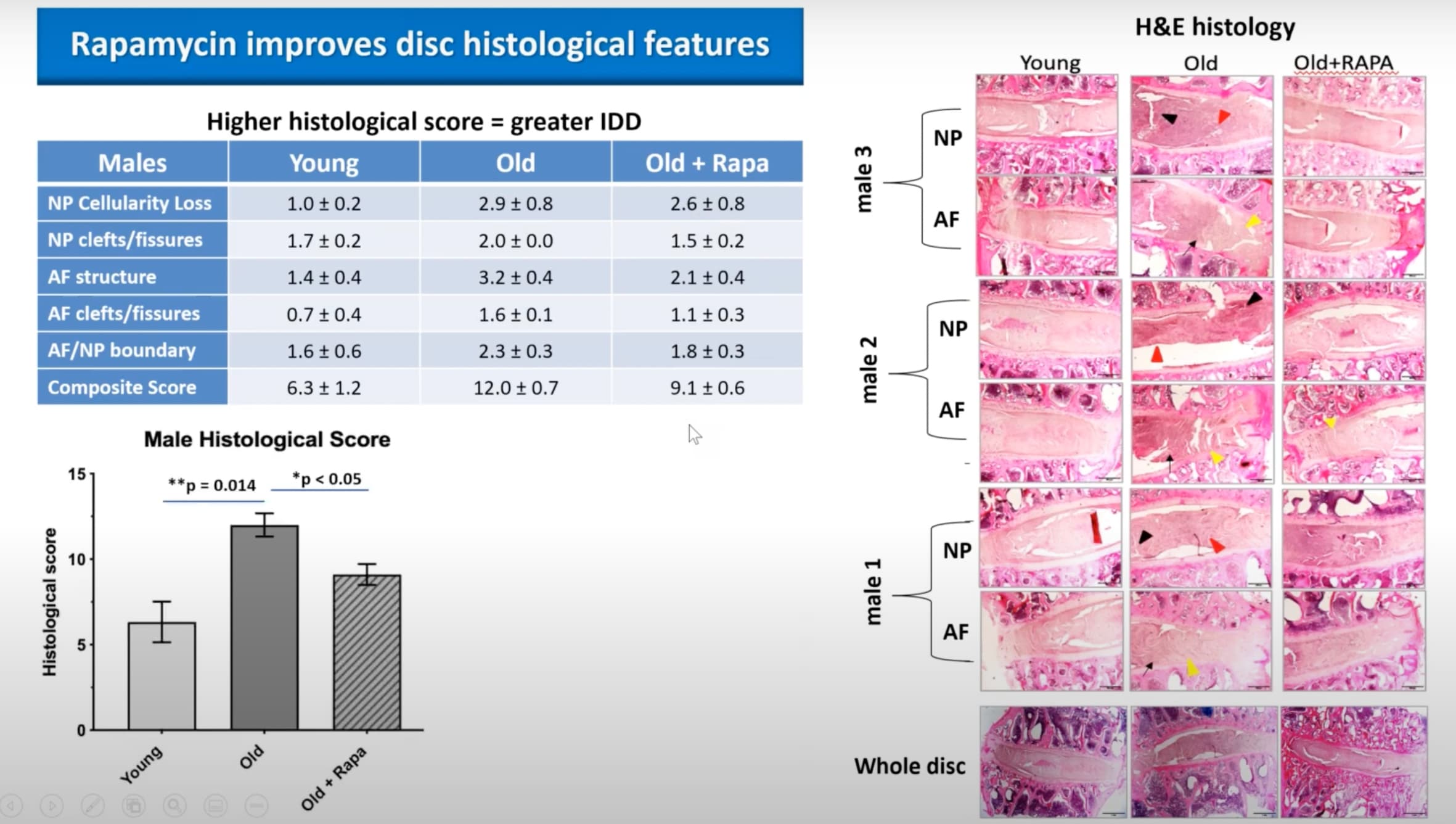
Spinal Health
Also - when you look at spinal disc degeneration that comes with age you see that rapamycin reverses some of the effects of age on the spinal disc, but only about 50% (very roughly). While this study was done in older monkeys and looked at spinal disc regeneration, I suspect that the results for preservation of the discs would be much better if rapamycin was started earlier. As with all these areas, more research needs to be done.
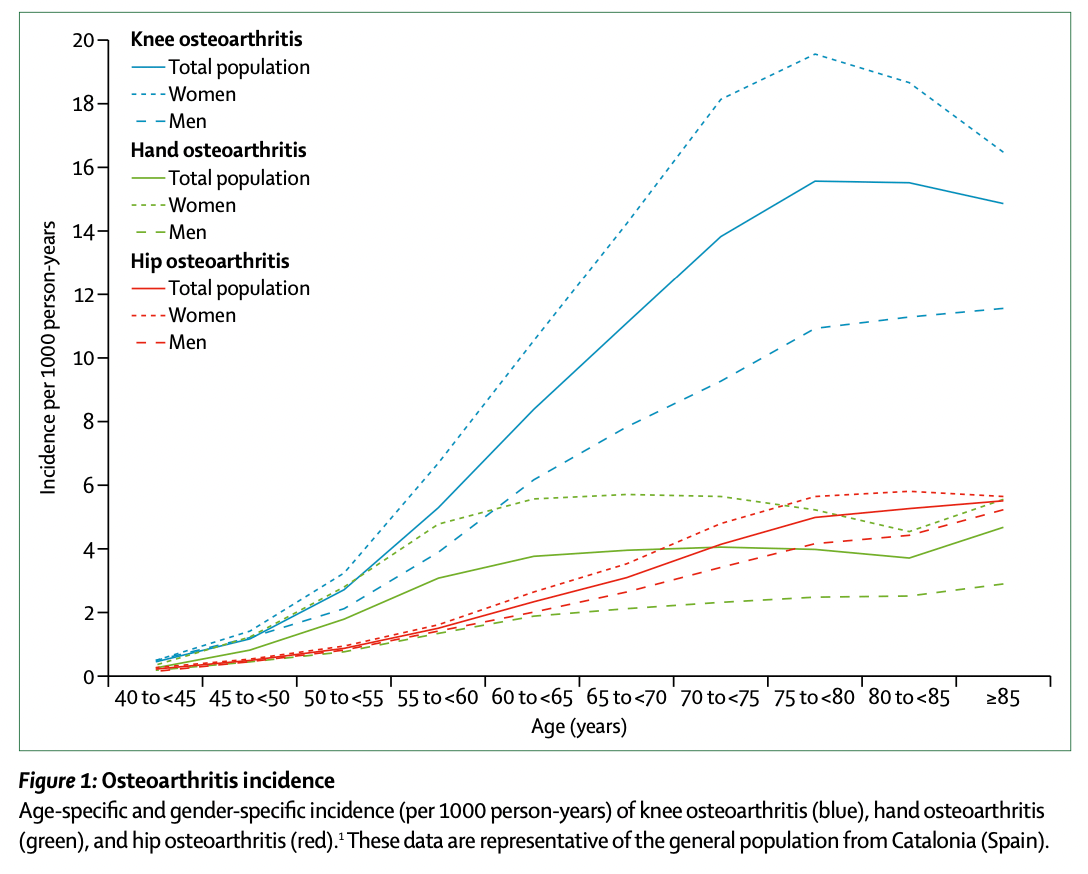
Osteoarthritis
Osteoarthritis is a leading cause of disability and source of societal cost in older adults. With an ageing and increasingly obese population, this syndrome is becoming even more prevalent than in previous decades (see this review paper on osteoarthritis).
New research on rapamycin suggests that treatment with Rapamycin may compress severe osteoarthritis pathology to late life. See this: “rapamycin delays osteoarthritis” research report and news story.
Problems taking Rapamycin When Older
Other issues arguing for younger rather than older for initiation of rapamycin might be:
-
The older you are, the more sensitive you are likely to be to any side effects. Generally people are stronger, more fit, healthier and more resilient when they are younger - so they are more able to handle any medication side effects or any illnesses, etc. Therefore rapamycin may be less risky for younger rather than older people. I haven’t looked closely, but I suspect older people have to go off medications more frequently due to bothersome side effects than people in their 30s and 40s, just because they have a healthier body.
-
The issue of “Polypharmacy”. I look at my parents and their friends and I see people who take a lot of different medications for a lot of different conditions… and adding rapamycin into the mix makes things even more complex and difficult to manage for the medical professionals, and more likely to be problematic. When people are young, they typically aren’t taking any medications - or a minimal amount, and mostly periodically - when they are sick - so it would be much easier to manage integrating rapamycin into their lives and any of the medication the person may be using if they are young. (A group in the UK are struggling with this issue: Video: Safe set of drug candidates for aging - John Overington)
Risks
And, of course - all this has to be weighed against the risks of taking rapamycin at whatever age the person is at. Those risks are still being determined, and will likely be dose dependent.
At high, continuous doses there is evidence that rapamycin can negatively impact the male gonads/ spermatogenesis - and ability to have children. This problem is generally believed to go away after a male stops taking rapamycin, (similar to the case in caloric restriction) - and that has been documented in younger male transplant patients who go on to have children after initially being unable to while on high doses of rapamycin) - but there is some lower level risk there that has to be considered.
There is also risk of cataracts (seen in mice at high doses, not in people), and also possible immune system reduction - which can result in serious problems. So these would also need to be factored in, though again, the risk is likely much lower for younger people, especially at lower doses of Rapamycin dosed periodically.
What are your thoughts? What research have you seen and what do you think might be the best age to start rapamycin?