I’ve been doing a little research on the whole issue of formulations of sirolimus / rapamycin using Elan pharmaceutical’s nanocrystal technology.
Here is what I’ve found:
NanoCrystals particles consist entirely of drug, thinly coated with a surface modifier to impart physical stability. NanoCrystals provide manufacturing and clinical performance advantages by eliminating the formulation problems usually associated with physical changes in drugs during micronization and formulation, thereby eliminating problems associated with loading and releasing drugs from delivery devices.
According to Elan, NanoCrystals benefit any drug formulation. Advantages include quicker onset of action, increased dose uniformity, fewer side effects, enhanced bioavailability, improved dose proportionality, elimination of food effects, more predictable therapeutic response, targeted delivery, improved safety, and greater efficacy.
So - what does the science say?
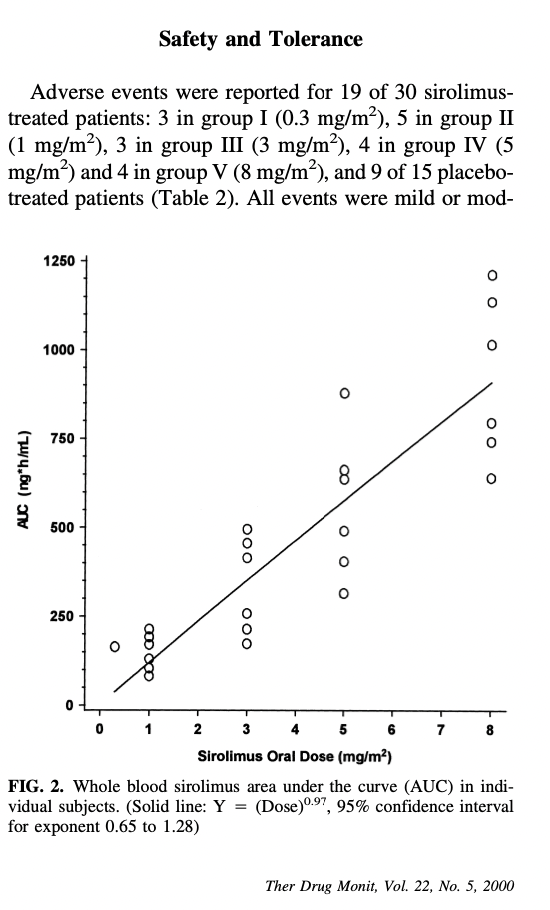
This study suggests:
Rapamune® (Wyeth) is a nanocrystalline-based formulation of the macrocyclic immunosuppressive drug sirolimus (rapamycin). It was the first nanocrystalline product to reach the market and is available in two formulations: oral suspension and tablets [10]. The product was developed using Elan’s NanoCrystal® technology in order to eliminate limitations related to the first commercially available formulation of sirolimus, which is a viscous oral solution of the drug in Phosal 50 PG and polysorbate 80. The lipid-based liquid solution needs to be refrigerated and protected from light upon storage, it is unpalatable and its dispensing protocol is complicated [66]. Rapamune® tablets, on the other hand, exhibited a 27% increase in the bioavailability of the drug compared to the lipid-based solution and their ease of administration contributes to enhanced patient adherence to medication [67].
[Note - this says above that they see a 27% increase in bioavailability compared to the liquid-based solution. No comment comparing it to other tablet based products like the generics from Zydus, Biocon, Dr. Reddy’s etc.]
They reference (for this above quote) this paper:
Merisko-Liversidge E. Nanosizing: ``End-to-End’’ Formulation Strategy for Poorly Water-Soluble Molecules. In: Templeton AC, Byrn SR, Haskell RJ, Prisinzano TE, editors. Discovery and Developing Molecules with Optimal Drug-Like Properties, New York, NY: Springer New York; 2015, p. 437–67. doi:10.1007/978-1-4939-1399-2_13.
where they state:
The biopharmaceutical performance value that particle size reduction can impart on a product is best illustrated by reference to the NanoCrystal products in the marketplace. The first NanoCrystal product that was launched was Rapamune, an immunosuppressive medication in tablet form, indicated for renal transplant patients (Shen and Wu 2007). The active ingredient, rapamycin (sirolimus), is a poorly watersoluble fermentation product (MW.914.17 g/mol). In accordance with the Biopharmaceutical Classification System (BCS) (Benet 2013), Rapamycin is a Class IV molecule, i.e., poorly soluble and poorly permeable. The product was initially launched as a liquid-lipid solution containing phosphatidylcholine, propylene glycol, monoglycerides, ethanol, soy fatty acids, ascorbyl palmitate and polysorbate 80, i.e., Phosal ®50® PS. This solution is stored refrigerated and has a rather elaborate procedure for dispensing and dosing. Conventional tableting approaches proved to be problematic and incompatible with the chemical stability of the molecule. However, with wet-media milling, rapamycin is fractured as a crystalline solid. Maintaining the molecule in a crystalline solid state during processing, improved chemical stability (Liversidge and Wei 2007) and provided opportunity for the product, by launching a tablet after liquid solution. In addition, the nanocrystalline tablet formulation prepared from a nanosuspension of rapamycin exhibited a 27 % improvement in bioavailability (Shen and Wu 2007). Although improved bioavailability was not a goal for the project, it was interesting to observe that when formulated using NanoCrystal technology, the nanosized formulation out-performed the liquid-lipid solution in terms of bioavailability, stability, and ease of administration.
I have yet to study all the papers - but it looks like a moderate improvement in bioavailability - but about the same level of improvement as taking rapamycin with a fatty meal, 20% to 30%. So - not a deal breaker, but interesting.
Given this statement above:
Conventional tableting approaches proved to be problematic and incompatible with the chemical stability of the molecule.
It would seem interesting to know the variations in bioavailability and performance (in terms of raising your blood/sirolimus levels, half life, etc.) of the different generic versions of rapamycin that are available - I wonder if any groups have ever done a head to head comparison.
Given the licensing costs of something like the Elan pharma nanocrystal technology - I’d actually be surprised if any of the generics have anything like it, as the focus in generic medications is always “cost”.
Related Reading:
Progress in the study of drug nanocrystals
Currently marketed pharmaceutical nanosuspension products
From: Emerging role of nanosuspensions in drug delivery systems
| Trade name/Company | Drug | Dosage form/Route of administration | Nanosuspension method | Indication |
|---|---|---|---|---|
| Abraxane®/Abraxia Biosciences | Paclitaxel | Freeze-dried powder for injection/ Parenteral | nab™ | Metastatic breast cancer |
| Cesamet®/Lilly | Nabilone | Capsule/Oral | Coprecipitation | Antiemetic |
| Emend®/Merck | Aprepiant | Capsule/Oral | Nanocrystal®Elan | |
| Nanosystems | Antiemetic | |||
| Giris-PEG®/Novartis | Griseofulvin | Tablet/Oral | Coprecipittation | Antifungal |
| Invega Sustenna®/ Johnson & Johnson | Palperidone palmitate | Liquid nanosuspension/ Parenteral | High pressure homogenization | Schizophrenia |
| Megace ES®/Par Pharmaceutical Companies | Megestrol-acetate | Liquid nanosuspension/Oral | Nanocrystal®Elan Nanosystems Media milling | Anti-anorexic |
| Rapammune®/Wyeth | Sirolimus | Tablet/Oral | Nanocrystal®Elan Nanosystems | Immunosuppressant |
| Tricor®/Abbott | Fenofibrate | Tablet/Oral | Nanocrystal®Elan Nanosystems | Hypercholesterolemia |
| Triglide®/First Horizon Pharma | Fenofibrate | Tablet/Oral | IDD-P® Skyepharma | Hypercholesterolemia |
| Avinza®/King Pharmaceuticals | Morphine sulphate | Tablet/Oral | Nanocrystal®ElanNanosystems | Psychostimulant |
| Ritalin®/Novartis | Methyl Phenidate HCl | Tablet/Oral | Nanocrystal®ElanNanosystems | Muscle Relaxant |
| Zanaflex™/Acorda | Tizanidine HCl | Capsules/Oral | Nanocrystal®Elan Nanosystems | Muscle Relaxant |
| Focalin®XR/Novartis | Dexmethylphenidate hydrochloride | Tablet/Oral | Nanocrystal®ElanNanosystems | CNS Stimulant |
| Ostim®/Heraseus Kulzer EquivaBone®/Zimmer BiometOsSatura®/IsoTis Orthobiologics NanOss®/Rti Surgical | Hydroxyapatite | Paste/Injection | a | Bone substitute |
| Vitoss®/Stryker | Calcium phosphate | Foam packs, Foam strips/Injection | a | Bone substitute |
| Ryanodex®/Eagle Pharmaceuticals | Dantrolene sodium | Freeze-dried powder for injection/intravenous | a | Malignant hypothermia |
The first five examples were manufactured using wet bead milling (Elan’s NanoCrystal® technology, now owned by Alkermes), while the last one uses high pressure homogenization (Skye Pharma’s IDD-P technology).