Hi, and welcome to the site. Good questions…
I personally think its a really good idea to at least do fasting blood tests before you start rapamycin so that you have a baseline to look at later and compare your results over time.
The Complete blood chemistry panel from LEF is a good one - and one I’ve used a number of times. At $35 its a great value. I also do the CRP test - so I can do the Levine phenotypic calculations for biological age - and its been going well so far - with a 15 year lower biological age compared to chronological age. Sadly I didn’t test before I started rapamycin, so I have no idea if rapamycin has helped in that calculation.
By the way - for peoples benefit - here is the free spreadsheet (towards the bottom of this page at the following link) that I think Mike Lustgargeten pulled together so we don’t have to log onto special websites to calculate our Levine Phenotypic age.
Please - post your results here over time.
I try to get my basic CBC and CRP blood tests done every few months so I can track my progress.
The issue of the value of the sirolimus blood level test is a harder question. Its a blood test that is used commonly for serious disease patients using rapamycin (e.g. organ transplant, cancer, etc.) because they want to make sure that the level of the drug is high enough to be providing value. In our case we sort of want the opposite - we want to know that the trough level is low enough so that we aren’t inhibiting the mTORC2 complex, and therefore at risk of suffering from the negative side effects like immune system lowering.
In theory this blood test would help us, when done right at the end of the week (or two, if you’re on the two-week dosing schedule) just before you we take the next weekly dose of rapamycin, we can see if our blood sirolimus levels are low enough that we can be confident that we aren’t blocking mTORC2.
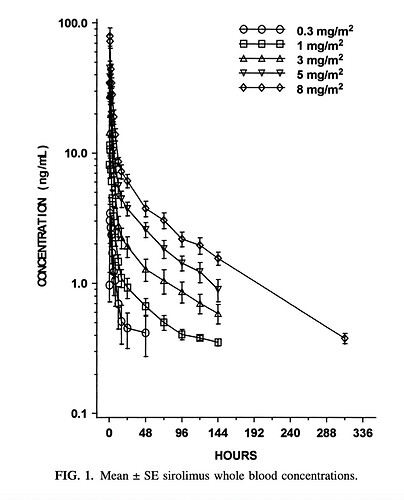
Dr. Green has suggested that we want to get our sirolimus blood levels down to 5 half-lives from when we took the last dose… which is a rather rough number. The half life for sirolimus in transplant patients is around 62 hours (+/- 16 hours or so) but I’ve seen a paper that suggests the blood sirolimus levels in healthy, younger, ethnically diverse patient groups is more like 80 hours (+/- 12 hours). So there is a wide variety we may have in the people here who are using rapamycin for anti-aging.
But, I’m not sure we (and I mean the medical community “we”) even know what a good lower target blood sirolimus level should be for healthy humans in an rapamycin anti-aging application.
Does anyone else have an idea or thoughts on this?
