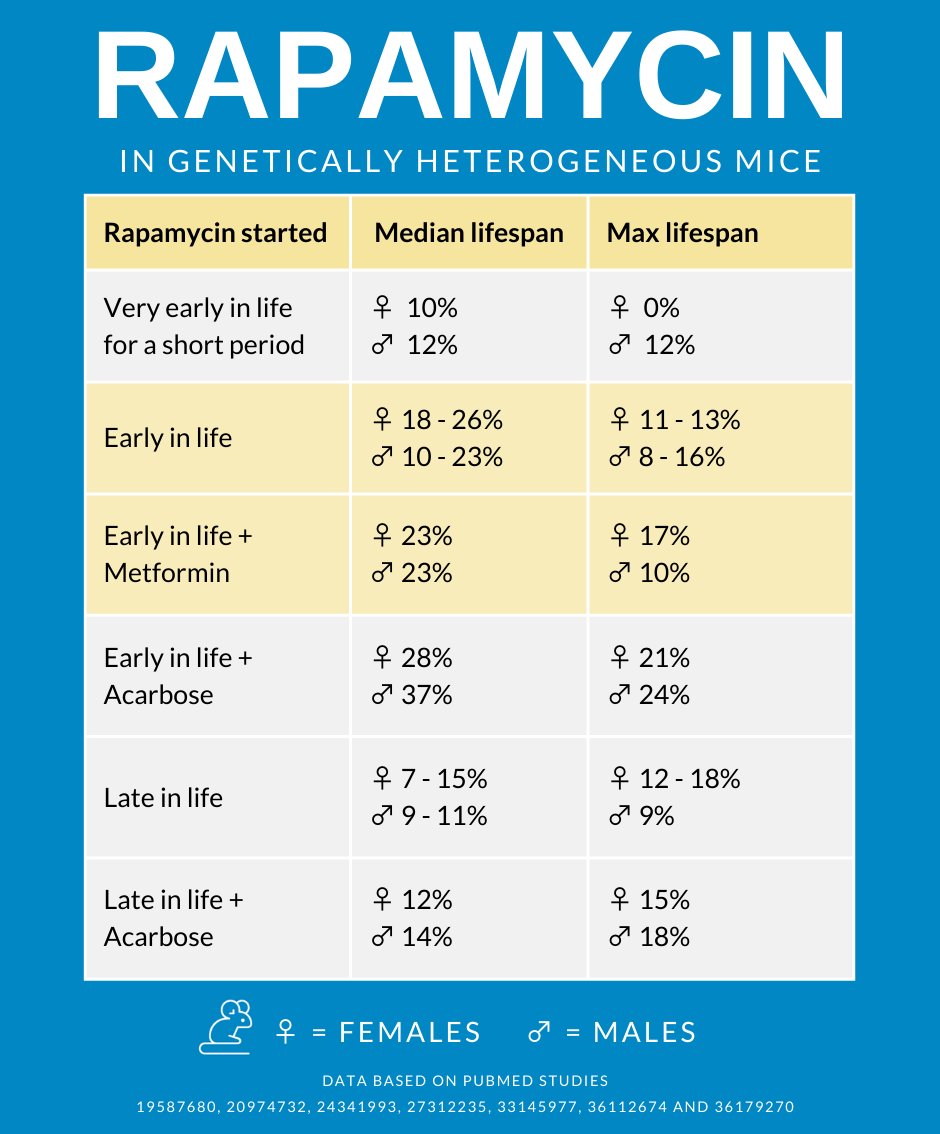
Another example where starting longevity drugs earlier in life result in better outcomes over starting later in life. In this study, the mice that started at age 9 months (equivalent to approx. 30 years old in human terms), lived 28% to 34% longer, whereas mice that started at age 16 months (equivalent to approx. 50 to 60 years in human terms) only lived 13% longer:
Mice bred in 2017 and entered into the C2017 cohort were tested for possible lifespan benefits of (R/S)-1,3-butanediol (BD), captopril (Capt), leucine (Leu), the Nrf2-activating botanical mixture PB125, sulindac, syringaresinol, or the combination of rapamycin and acarbose started at 9 or 16 months of age (RaAc9, RaAc16). In male mice, the combination of Rapa and Aca started at 9 months and led to a longer lifespan than in either of the two prior cohorts of mice treated with Rapa only, suggesting that this drug combination was more potent than either of its components used alone. In females, lifespan in mice receiving both drugs was neither higher nor lower than that seen previously in Rapa only, perhaps reflecting the limited survival benefits seen in prior cohorts of females receiving Aca alone. Capt led to a significant, though small (4% or 5%), increase in female lifespan. Capt also showed some possible benefits in male mice, but the interpretation was complicated by the unusually low survival of controls at one of the three test sites. BD seemed to produce a small (2%) increase in females, but only if the analysis included data from the site with unusually short-lived controls. None of the other 4 tested agents led to any lifespan benefit. The C2017 ITP dataset shows that combinations of anti-aging drugs may have effects that surpass the benefits produced by either drug used alone, and that additional studies of captopril, over a wider range of doses, are likely to be rewarding.
Here, we extend this strategy, testing rapamycin and acarbose in combination, starting at 9 or 16 months of age, based on a similar rationale to that used for the metformin/rapamycin trial.
Rapamycin plus acarbose, starting at 9 months of age (RaAc9) . This combination of agents produced a 28% increase in median lifespan in females (p < 0.0001) and a 34% increase in males (p < 0.0001) for data pooled across sites (Figure 1). This was the only treatment that significantly increased survival in both sexes at all three sites tested separately.
Rapamycin plus acarbose, starting at 16 months of age (RaAc16) , increased median lifespan by 13% both in females (p < 0.0001) and in males (p < 0.0001), using data pooled across sites (Figure 1). Site-specific analyses, shown in Tables 2 and 3, revealed a significant extension of lifespan at all sites for females, but only at UT for males. In females, RaAc16 extended median lifespan by 21% at TJL (p < 0.0001), 5% at UM (p = 0.01) and 18% at UT (p < 0.0001). RaAc16 increased 90th percentile survival for pooled data in both sexes (p < 0.001; Table 1) and at each site individually for females. In males, RaAc16 extended median lifespan of UT males by 32% (p < 0.0001). The RaAc16 effect on male survival was significant only at UT.
Captopril, started at 5 months , increased the median lifespan in females by 6% (p = 0.002) and in males by 13%
More reading:
Acarbose: Acarbose - Details On Another Top Anti-Aging Drug