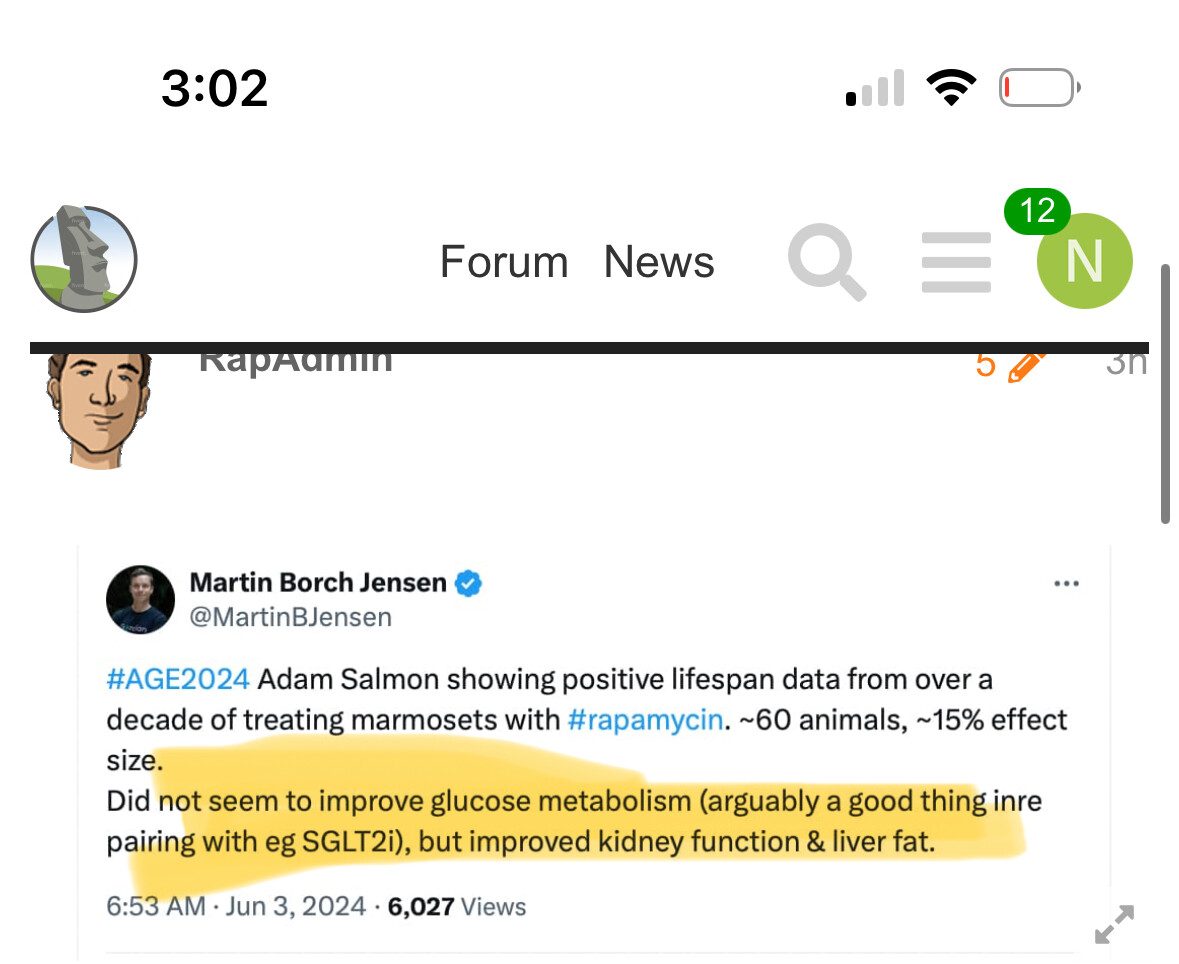
Some very good preliminary news on rapamycin was presented today at the American Aging Association Conference in Wisconsin. This is a groundbreaking development as its the first time we’ve seen primate lifespan improvement with rapamycin (or any other compound TTBOMK) in a well-designed study. It is based on the long-term study of rapamycin-dosed marmosets at UT Southwestern being done in the lab run by Adam Salmon.
This new announcement is important because while rapamycin has been proven effective in lengthening healthy lifespan in every organism its been tested in (including yeast, flies, worms and mice… by dozens of different labs around the world) it has never been tested in primates before for lifespan extension. Some people have questioned whether rapamycin, which has performed so well at lifespan extension in shorter-lived species, would do as well in longer-lived species. This study seems to resolve this question.
The newly announced results (an increase in the median lifespan by approx. 15% for the Rapamycin-dosed marmosets) would seem to be strong evidence that rapamycin works well in primates, and thus there is a very high probability it works similarly well in humans. I’ve contacted Adam Salmon for more information but he says the information presented at this conference is still preliminary so he wasn’t about to give me any survival curve data or other information yet. The research paper covering these results is in process, so we should see more details on the study soon.
The challenge that this news presents to us is that the dosing level and frequency for the marmosets was quite high compared to what we usually dose rapamycin in longevity applications as people are practicing it today. The marmosets received 1mg/kg dosing in their food daily, which given the typical animal to human dosing translations, seems to equate to around 10mg/day for a a 60kg person [Updated; perhaps closer to 30mg every day or two equivalent in humans, per Adam Salmon interview]. Most people in longevity applications right now are dosing around 6mg to 8mg once per week. This new marmoset study suggests that a higher dose may be required for humans to get the same level of benefit, but with higher doses of rapamycin we tend to see higher rates of side effects (diarrhea, gastro-issues, etc.) and if higher doses are taking on a regular basis you typically get some level of immune suppression, and potentially some lipid and blood sugar disregulation; all of which tend to increase health risks in humans. So this may be the key challenge for human translation of this research, how to get higher levels of rapamycin into the blood system, while minimizing the undesirable side effects and risks.
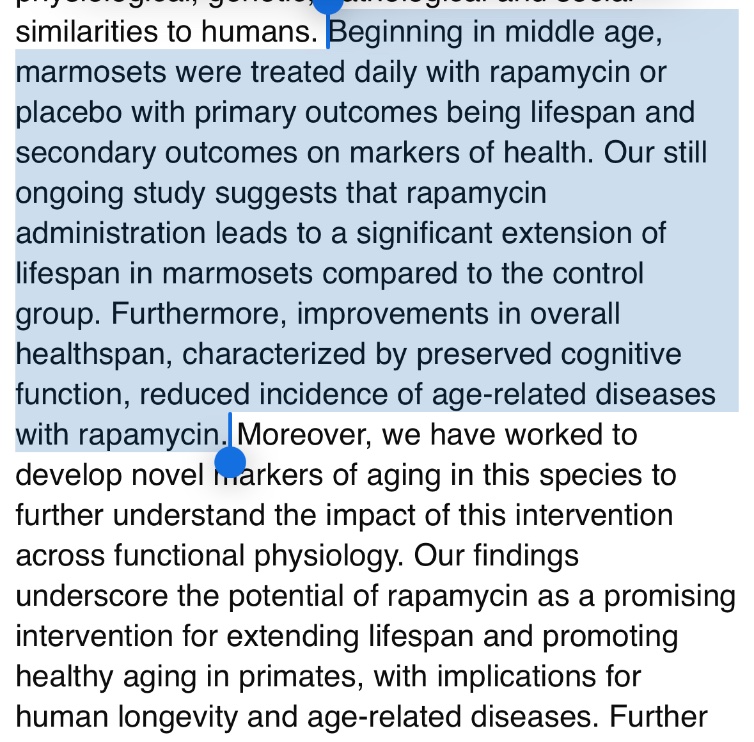
The AmericanAging conference abstract for this talk (Posted on X by David Barzilai):
1mg/kg per day, in-food dosing. This is a high dose, and only used in lab animals because they live in pathogen-free environments. I interviewed Adam last year - this will motivate me to post the audio this week.
Hmmm… that seems about right … I wonder how the researchers factor in metabolization time (i.e. do marmosets have the same half-life for rapamycin as we humans do?).
In other words, the fact that marmosets don’t typically die from cancer, and in this study they are living longer, suggests that the fact that their lifespan is increasing by 15% is actually due to slowing aging (not simply preventing cancer, as some suggested is the Method of Action (MOA) for rapamycin and life extension.
In this study, we found that long-term treatment of marmoset monkeys with orally-administered encapsulated rapamycin resulted in no overall effects on body weight and only a small decrease in fat mass over the first few months of treatment. Rapamycin treated subjects showed no overall changes in daily activity counts, blood lipids, or significant changes in glucose metabolism including oral glucose tolerance.
The paper on osteoarthritis did some stuff on the tissues:
Results Rapamycin decreased P-RPS6Ser235/36 and increased P-Akt2Ser473 in cartilage, meniscus, and infrapatellar fat pad, suggesting inhibition of mTORC1 but not mTORC2 signaling.
Do we know that 15% effect size is =
15% lifespan?
If the marmosets are the same ones as in the osteoarthritis paper they seemed to have started rapa when they were 9ish years old and only lived about 2 more years…?
After reviewing the marmoset (humanish) trial information. I am so glad to be an early adopter at 62.5 years old - now 66 years. I will take 15 more years of life and health span.
Let me be your lighthouse customer for rapamycin! And of course the rest of us on this site!
Origin of the early adopter idea
E.M. Rogers in 1962 first proposed the term early adopter in the diffusion of innovations (DOI) theory. It explains how a new idea, behavior or product gains momentum over time and spreads, or diffuses, through a population or social system. Through this diffusion, the people who are part of the social system adopt that new idea, behavior or product.
Per the DOI theory, adoption of the innovation does not happen in a social system all at once. Rather, some people will adopt the innovation before others. These are the early adopters – a small minority of people in the social system.
Rogers discussed five types of adopter stages. Besides early adopters, the other four adopter categories are as follows:
Innovators. They are the most daring people in a population and most willing to take risks. That’s why they’re the first to develop a new idea.
Early majority. This group includes people who typically adopt new ideas before most of the population, but they do so only after examining evidence that the innovation works.
Late majority. While resistant to change, they’re willing to adopt a new innovation after it’s been tried by the majority.
Laggards. These people are conservative and tradition-bound. They’re extremely resistant to change, making them the opposite of early adopters.
Really do hope that yours is the correct interpretation, but not sure.
The marmoset data from other paper is as below - that seems to match ~60 animals from the study with positive lifespan data
common marmosets treated with oral rapamycin (n=24; 1mg/kg/day) or parallel control group (n=41). Rapamycin started at 9.2±3.0 years old and lasted until death (2.1±1.5 years).
So the controls would have had to live very, very short for it to be 15% of total normal control age that was extended.
Perhaps there was something with the top 10% living much longer or something, for max life span increase of 15% even if the median was not as high.
This is amazing news! Rapamycin works for (almost) every living thing tested (sorry diabetic mice!). If it works for yeast, fruit flies, C. Elegans, mice, rats, and marmosets with an average increase in lifespan of 15%, you’d be a fool not to try it. It’s 100% repeatable over 70-80 studies. That’s unheard of in the scientific world, and a testament to Rapamycin’s capabilities.
I’ll take an extra 10-15 healthy years!
Where else can you buy 10-15 years of healthy lifespan for $3 USD a week?
But now the challenge will be to figure out how we can safely increase our dosing closer towards the 1mg/kg dosing that the marmosets were at without our benefiting from the “pathogen free” environment that these lab animals enjoy.
The lab marmoset environment is nothing like our own… so we still have our work cut out for us, if we want to get that 15% + healthy lifespan improvement. We are not likely getting it at the current 6mg/week level.
I’m currently at the 12-14 mg/week level. (4 mg + GFJ). Yes, I have been sick lately, but not as sick as compared to the past.
What I mean by this is as follows. In the past, I’d get a URTI and it would take 5 months to clear up (chronic dry cough). Now it only takes about a month. I still get sick once a year with the flu/COVID. I just recover quicker.
By effect size, I assume they just mean the statistical term. So for example, if the stdev of lifespan was 2 years, a 15% effect size would be 0.3 years or a ~2.5% increase.
That said, seems like it was started pretty late in life.