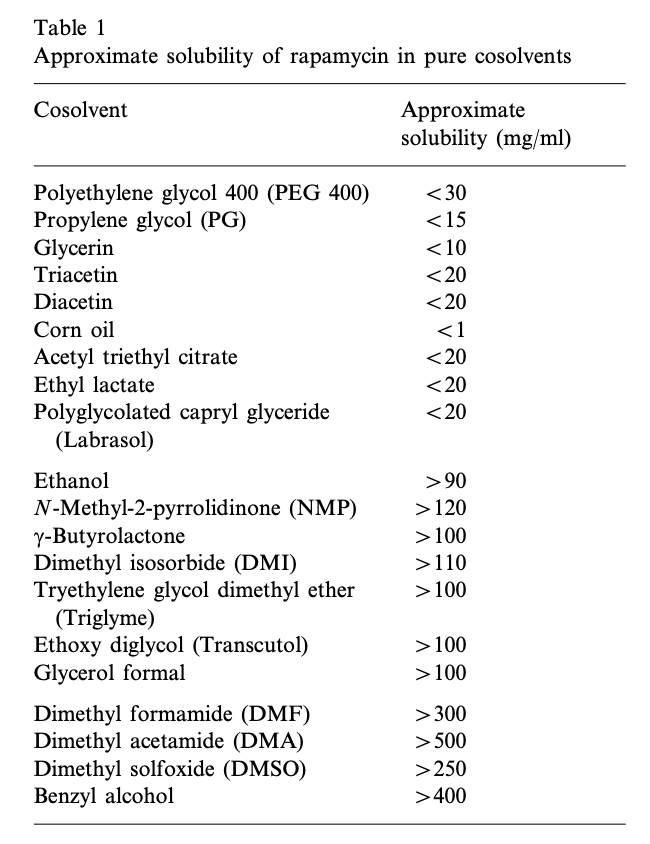
So, to address your first response regarding benzyl alcohol - yes, it has slower release time. This is because “like dissolves like” applies here.
The more similar a compound’s kinetics and properties are to its solvent (i.e. lipophilicity, surface charge/area, viscosity), the more readily it will dissolve in said solvent and reject others. This is the basis for most long-acting injections like testosterone, which is usually esterified into compounds like testosterone cypionate, which is many times more lipophilic than plain testosterone and thus will separate more slowly from its preferred solvent, oil.
Now, whether or not you want sustained, gradual release of rapamycin like this is debatable. I have no idea about the pharmacokinetics of such an injectable preparation of rapamycin, but if it ends up being similar to a long-acting injectable, you’d essentially be replicating a daily dosing regimen that cancer/transplant patients use, which has its own issues.
To address your second reply regarding nanoemulsions, I think you may be misunderstanding the purpose of such preparations. They are not typically intended for injection.
Injectable preparations are considered 100% bioavailable. This is because you use a parenteral route, bypassing saliva, bile acids, and liver metabolism. In other words, you avoid anything that could potentially degrade or inactivate your active drug.
Nanoemulsions are intended to make up for the limited bioavailability of oral preparations. Most drugs have poor solubility in aqueous solvents, especially so for rapamycin, so the idea is to encapsulate them in a carrier lipid which is also miscible with water; this allows the drug to be more readily absorbed by the intestines.
Creating nanoemulsions, or even micellar ones, requires very precise and controlled laboratory conditions. It isn’t something that can be achieved at home, unless you bootleg some specialized lab equiment (which you usually need a license for, even secondhand).
So, for IM and SC, nanoemulsions wouldn’t make much sense since you’re not injecting into aqueous environments. For IV, it would matter since blood is aqueous, so you may see nanoemulsions used here in order to bridge the aqueous solubility issue. Most people here seem to be aiming for IM or SC, which is far easier to prepare and use than IV. Furthermore, IV preparations need to be used fresh every time since aqueous solvents have very short shelf lives, so it would be extremely difficult to do at home.
And yes, taking the raw powder orally, even when packed into a capsule, is basically like ingesting nothing. Most of it will be destroyed in bile acids, and most capsules marketed as “enteric-coated” are actually fake, since you’d need a pharmaceutical license to make enteric capsules due to regulations in the US. However, I do have methods for preparing enteric-coated tablets at home which can bypass the stomach acids, so let me know if you’d like a how-to for that. I can’t guarantee that it’d have the same performance as the factory-prepared ones, but you can get pretty damn close.
Just keep in mind… making your own medicine is illegal. So, if you purchase any medicine-making equipment, it will put you on a list. The FDA and DEA do not fuck around with homemade drugs. If they suspect you are making drugs of any kind, be wary of getting raided. Usually most people will fly under their radar, but if you have an online record of buying pharmaceutical equipment (ESPECIALLY tablet/pill presses) without a license… yeah… they might start monitoring you. Buying the ingredients is fine, but buying equipment implicates you as a manufacturer and/or distributor.
When your tissues start to necrose, deteriorate, or other similar effect. Cytotoxic just means that cells begin to malfunction and die. I’m assuming you’re talking with regard to DMSO, which is generally safe when kept to a concentration of 10% or lower. However, even at 100%, you should be fine as long as you rotate sites and keep injection volume low. It just tends to sting like a bitch, but tolerance can vary between individuals such as with MAC, who has no reaction to it. Cytotoxicity really only appears if the same site is exposed repeatedly over a long period of time. To date, only a few cases of this have been reported from people drinking bottles of the stuff for some reason.
This is just a disclaimer that I usually have to put because of my background. The pharmacokinetics of injectable rapamycin in humans, aside from a few IV trials, has not been well-investigated. We have no idea how IM or SC administration would perform. Therefore, I cannot recommend it.
The reason I still give advice is because of harm-reduction. That is, if people are going to self-experiment anyways, they should at least know how to do it properly in order to reduce the overall risk.
I suppose the economics of it would be better, but keep in mind what I mentioned earlier regarding pharmacokinetics. Saving money per dose is a rather tiny detail compared to the overall unknown of such a radical treatment. I’d be more concerned about the impact on your overall health rather than price per bioavailable dose, since the former can end up costing you far more than you’d save on a kilo of powder.