In the distant past the concept of “young blood” as a fountain of youth was the stuff of fringe science. However, the discovery of heterochronic parabiosis—physically stitching the blood circulatory systems of young and old mice together—transformed this myth into a rigorous biological inquiry, with significant health and longevity benefits demonstrated in research studies done over the past two decades.
The most striking benefits of this young blood exposure are localized in the brain, where the introduction of young blood components, coupled with the dilution of pro-aging factors like β2-microglobulin, reverses established impairments in synaptic plasticity and hippocampal function, driving a reversal of age-related cognitive decline. Mechanistically, these experiments show that young plasma revitalizes the aging brain by stimulating neurogenesis and decelerating epigenetic aging processes.
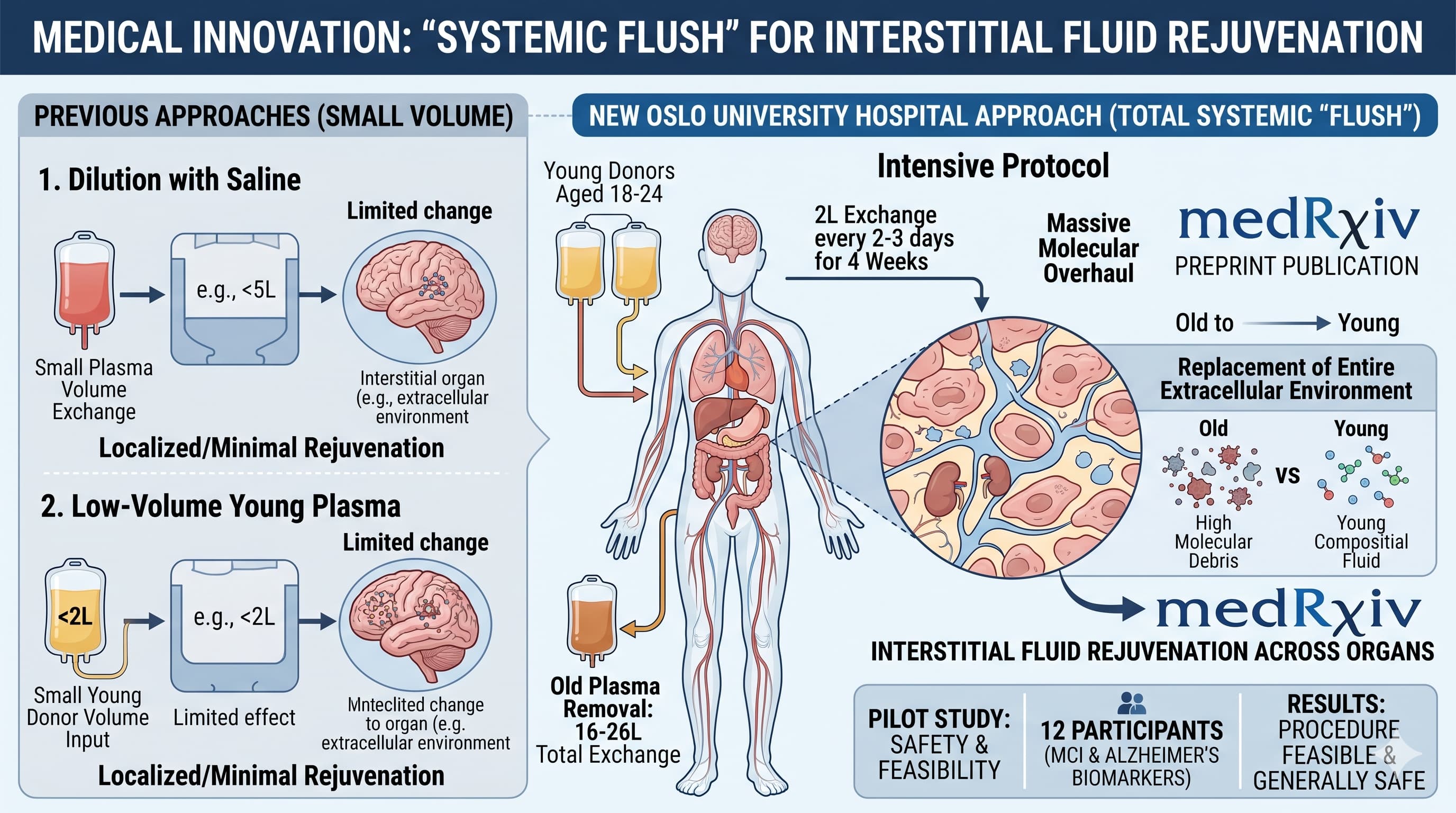
While previous human trials focused on either diluting old plasma with saline or albumin, or infusing small amounts of young blood plasma, researchers at Oslo University Hospital have now taken the logical, if aggressive, next step: a total systemic “flush”.
The pilot study, published as a preprint on medRxiv , investigated the safety and feasibility of “interstitial fluid rejuvenation”. Unlike simple blood transfusions, this protocol aimed to replace the entire extracellular environment within organs—a staggering 16 to 26 liters of plasma per patient—using donors aged 18 to 24. The 12 participants, all diagnosed with mild cognitive impairment (MCI) and biomarker evidence of Alzheimer’s disease, underwent various treatment intensities to determine if a human body could handle such a massive molecular overhaul.
The researchers hypothesized that by exchanging large volumes of plasma and allowing for a 48-hour equilibration period, they could shift the molecular composition of the interstitial fluid to resemble that of a young adult. Their “intensive” protocol involved exchanging approximately 2 liters of plasma every 2 to 3 days over a four-week period.
The results indicate that the procedure is feasible and generally safe within a controlled clinical environment. While two life-threatening adverse events occurred—a severe infection and a rare connective tissue tumor—independent reviews judged them unlikely to be caused by the treatment. Common side effects were limited to known risks of plasma exchange, such as mild allergic reactions. While the sample size was too small to claim clinical efficacy, the study provides a blueprint for a new modality of anti-aging therapy: the systemic removal of the “aged milieu” paired with the introduction of youthful signaling factors.
Actionable Insights
The “Whole-Body Flush” Threshold: For biohackers and clinicians looking at therapeutic plasma exchange (TPE), this paper identifies a volume of 3 liters (blood plasma) plus 12 liters (interstitial fluid) as the theoretical target for complete systemic rejuvenation.
Equilibration Timing: The study suggests that most proteins equilibrate between the blood and organs within 48 hours. Any protocol intended to “rejuvenate” organ tissue must account for this transcapillary exchange rate (5.2%/h for albumin) rather than assuming a single transfusion is sufficient.
Donor Selection Rigidity: The use of donors aged 18–24 is critical. The study notes that youthful signaling environments are highly sensitive to donor lifestyle factors and age-related molecular shifts.
Biomarkers for Monitoring: Practitioners should track grip strength and FEV1 (lung function) alongside cognitive tests (MoCA), as these physical metrics improved in rodent parabiosis studies and are reliable markers of biological aging pace.
This is the first published human protocol to combine large-volume plasma removal with young-donor replacement (18–24 years) at a scale (16–26 L) intended to rejuvenate the interstitial fluid. It bridges the gap between rodent parabiosis and human clinical practice by treating the blood as a communication medium for systemic aging rather than just a fluid.
Study Design Specifications
Type: Clinical Trial (Pilot safety and feasibility study; Open-label, unblinded).
Subjects: 12 humans (8 males, 4 females).
Condition: Mild Cognitive Impairment (MCI) with positive beta-amyloid PET-CT or CSF biomarkers.
Control Group: None (Patients received standard treatment as usual).
Potential Commercial Cost in the USA
Based on the volumetric data provided in the pilot study, the total plasma exchanged per patient ranged from 16 to 26 liters. To calculate the total cost based on your hypothetical pricing of $5,000 to $8,000 per liter (prices for young blood, per liter, that have been quoted by USA commercial providers) , the following table extrapolates the total expenditure per patient group using the mean volumes reported in the study:
Per-Session Costs : In the intensive protocol, patients received approximately 1.83 liters of plasma (three 610 ml bags) per session. At the hypothetical $5,000–$8,000/L rate, a single treatment session would cost between $9,150 and $14,640 for the plasma alone.
Study Cost Baseline : The researchers’ own internal cost estimates were significantly lower, ranging from a mean of EUR 4,541 to EUR 6,650 per patient for the entire treatment course. These figures included donor plasma, consumables, and personnel, reflecting the use of a non-profit, hospital-integrated blood center rather than premium commercial “young plasma” sources.
Equilibration Requirements : The study emphasizes that “interstitial fluid rejuvenation” requires large-volume exchange (theoretically 15 liters to cover both blood plasma and interstitial fluid) to shift the signaling environment within organs. At your provided price points, achieving this threshold would represent a high-cost intervention compared to traditional therapeutic plasma exchange (TPE).
Knowledge Gaps and Scholarly Debate
A primary knowledge gap exists regarding the dose-response relationship for young plasma in humans; it is currently unknown if lower volumes could achieve similar cognitive results if specific pro-youthful factors were concentrated. Nor do we know how long the benefits of this young plasma (blood) treatment would last, or how frequently it would need to be done to maintain the benefits. Furthermore, scholarly debate continues regarding the ethical implications and scalability of sourcing such massive volumes from young donors (ages 18–24), who have high attrition rates due to lifestyle factors. Additional data from randomized controlled trials would be required to determine if the high costs associated with your hypothetical pricing could be justified by clinically significant slowing of Alzheimer’s disease progression.
an email from one of the paper authors (on the GRG mailing list):
Thank you all for your nice comments on our manuscript on yFFP! We are so happy that it is finally available!
It is an ambitious project with many collaborators contributing time and effort, and it was made possible by an Impetus Grant and more than 50 young blood donors. We aim to continue the project later this year.
Regarding Tom’s comments on TRALI: our specialists in transfusion medicine, who were intimately involved in project planning, advised that sex-matching does not completely eliminate TRALI risk. We mitigated risk through several measures: we excluded ever-pregnant women from our donor pool, performed routine anti-HLA screening on all donors (with additional anti-HNA 3a screening for female donors), and excluded plasma from donors found positive for these antibodies. We also excluded participants with any new signs of inflammation, as inflammation is believed by some to increase TRALI risk.
On the question raised about mitochondria and repeated transfusions: There is extensive clinical experience with repeated large-volume FFP transfusion, which is reassuring. TTP patients, for instance, routinely undergo daily plasma exchange for weeks during acute episodes and long-term maintenance over years.
On the choice of exchange over infusion: our design goal is interstitial fluid rejuvenation. This was partially based on parabiosis experiments and on our own results from blood epigenetic age after heterochronic hematopoietic stem cell transplantation (https://onlinelibrary.wiley.com/doi/10.1111/acel.14112).
Interstitial fluid rejuvenation requires exchange of large plasma volumes to meaningfully shift the molecular environment within organs. Small-volume infusions, however well-tolerated, cannot achieve this. The Spectra Optia simultaneously removes and replaces plasma at zero fluid balance, which means TACO is not a concern in our protocol. The trade-off, as Tom rightly notes, is reduced efficiency — plasma given early in the procedure circulates and is partly removed later. In most of our procedures, the machine calculated 60–70% plasma exchange at completion.
Efficiency could probably have been improved by accepting some blood-volume change, but this introduces additional risk for limited gain. In our setting, the cost savings would also be modest: our close collaboration with the Blood Bank — and their enthusiastic staff motivating young donors to participate — gave us sufficient and (by US standards) inexpensive supply of yFFP.
To be honest, the safety profile is questionable. Aside from two life-threatening adverse events, six Grade 3 severe adverse events occurred across the six patients, which directly forced the interruption of the current treatment and required rescue medication with oral corticosteroids and antihistamines. Furthermore, there were 17 Grade 2 events and 34 Grade 1 events, covering symptoms such as localized urticaria, dry cough, and hypocalcemia. As for efficacy, no cognitive improvement was observed; the disease simply continued to progress as expected.
Reasonable people will disagree on what are acceptable side effects, but to me this doesn’t seem very bad (but obviously we need a real study to identify the positives before making any conclusions on the risk/reward tradeoff).
Safety Profile
The safety profile of large-volume young-donor therapeutic plasma exchange (TPE) in this pilot study revealed a total of 60 adverse events (AEs) across the 12 participants. The events were classified using standard clinical grading from Grade 1 (mild) to Grade 4 (life-threatening).
Grade 4 Adverse Events (Life-Threatening or Severe Morbidity)
The study recorded two Grade 4 adverse events. Both were critically evaluated by an independent Safety Committee and determined to have a low probability of causal relation to the plasma exchange protocol itself.
Severe Infection, Probable Liver Abscess, and Supraventricular Tachycardia (SVT): One patient was hospitalized seven days after completing nine intensive treatments.
Clinical Commentary: The patient had a documented history of SVT prior to enrollment. The investigators judged the event as having a low probability of being caused by the plasma exchange. The presentation of a localized liver abscess points toward an opportunistic or pre-existing infectious focus independent of the sterile apheresis process.
Undifferentiated Pleomorphic Sarcoma: One patient noticed a tumor in their arm during the treatment cycle, which was confirmed weeks later as a rare malignant connective tissue tumor.
Clinical Commentary: The treating oncologist concluded that the tumor was not caused by the intervention. Connective tissue sarcomas require significant timelines to develop oncologically; the physical manipulation of the arm during dual-vein cannulation or the intensive clinical surveillance simply accelerated the detection of a pre-existing, asymptomatic malignancy.
Grade 3 Adverse Events (Severe)
Six Grade 3 adverse events were documented among six separate patients. These represent the most significant directly actionable risks discovered during the trial.
Generalized Urticaria (3 cases): Severe hives occurred during the procedure, forcing the clinical team to abort the ongoing session.
Clinical Commentary: This is a classic hypersensitivity reaction to foreign plasma proteins, well-recognized in standard transfusion medicine. The events were managed successfully with a single tablet of antihistamine and short-term oral corticosteroids (prednisolone), with all patients fully recovering by the next day. This is an inherent risk of blood product transfusion rather than a specific toxicity of “young” plasma.
Cough without Dyspnea (1 case): This respiratory reaction led to the temporary discontinuation of the active plasma bag.
Clinical Commentary: The session was successfully completed the same day following the administration of an antihistamine and oral prednisolone. Like urticaria, this represents a mild, transient anaphylactoid response to donor plasma components.
Paroxysmal Atrial Flutter (1 case): Detected during a scheduled break in the procedure after the fifth treatment session.
Clinical Commentary: The patient was stabilized with anticoagulant therapy, and the event was deemed unlikely to be associated with the protocol. Older populations with early-stage neurodegenerative disease carry baseline cardiovascular vulnerabilities; large fluid shifts inherent to shifting 2 liters of plasma could theoretically act as a transient hemodynamic trigger, though it does not reflect direct chemical toxicity from the young blood.
Physical Testing Injury (1 case): A Grade 3 adverse event was triggered directly by one of the physical performance tests.
Clinical Commentary: This event was entirely independent of the apheresis or plasma transfusion mechanisms. It represents an operational hazard of the baseline frailty testing protocol rather than the biological intervention.
Grade 2 Adverse Events (Moderate)
Seventeen Grade 2 events were registered across eight patients, with six showing a probable or likely association with the TPE process.
Vivid Dreams and Mild/Localized Urticaria: Transient neurological and localized dermatological responses.
Clinical Commentary: Localized itching or hives represent minor immune reactivities to donor proteins that did not require terminating therapy. Vivid dreams suggest potential systemic signaling changes in the central nervous system, though placebo or psychological components cannot be ruled out in an open-label design.
Mild Symptomatic Hypocalcemia (2 cases): Muscle twitching or tingling sensations during apheresis.
Clinical Commentary: This is a direct, predictable side effect of the anticoagulant used (sodium citrate or anticoagulant citrate dextrose solution A). Citrate chelates ionized calcium in the patient’s blood. The protocol managed this effectively by pre-medicating with 500 mg calcium chewing tablets and administering additional doses during the procedure.
Elevated Cardiac Markers: Mildly elevated Troponin T and creatine kinase.
Clinical Commentary: This occurred exclusively after a maximum-exertion cardiopulmonary exercise testing (VO2max) protocol. It is a known physiological artifact of strenuous physical testing in older adults, not an adverse effect of plasma rejuvenation.
Pre-existing Baseline Conditions (Anemia and Supraventricular Arrhythmia): Discovered or tracked during the trial.
Clinical Commentary: One patient’s mild anemia was documented as having lasted for several months before entering the study. The arrhythmias were likewise present pre-trial. They are clinically unimportant regarding the safety of TPE, as they reflect baseline sample characteristics of an aging cohort rather than treatment-induced pathology.
Grade 1 Adverse Events (Mild)
Thirty-four Grade 1 events occurred, meaning every participant experienced at least one mild reaction. Sixteen were directly linked to the intervention.
Mechanical and Infusion Artifacts: Significant hematoma at the needle site (1 case), dizziness after the procedure, dry throat, and feeling cold followed by a mild (0.6 degrees) temperature increase during treatment.
Clinical Commentary: Large-bore intravenous access needles (typical 18G to 16G cannulas) frequently cause local bruising or minor hematomas. Temperature drops are standard when infusing room-temperature or recently thawed fresh frozen plasma, followed by minor rebound thermal corrections. Dizziness is a typical orthostatic response following hours spent immobile in a treatment chair.
Minor Systemic/Dermatological Reactivity: Evening sleepiness, feeling warm before bedtime, itchy eyes, itchy face, and an increased number of skin spots.
Clinical Commentary: These represent low-grade, transient physiological accommodations to massive protein shifts. They do not pose clinical risks and typically resolve without medical intervention.
Summary Assessment of Safety
From a biohacker or clinical specialist perspective, the safety data indicates that the protocol does not introduce novel toxicities. The documented actionable adverse events—specifically generalized urticaria and citrate-induced hypocalcemia—are classic, predictable, and fully manageable complications of standard therapeutic plasma exchange. The treatment appears clinically acceptable for wider testing, provided stringent screening for pre-existing cardiovascular vulnerabilities and strict adherence to calcium replacement protocols are maintained.