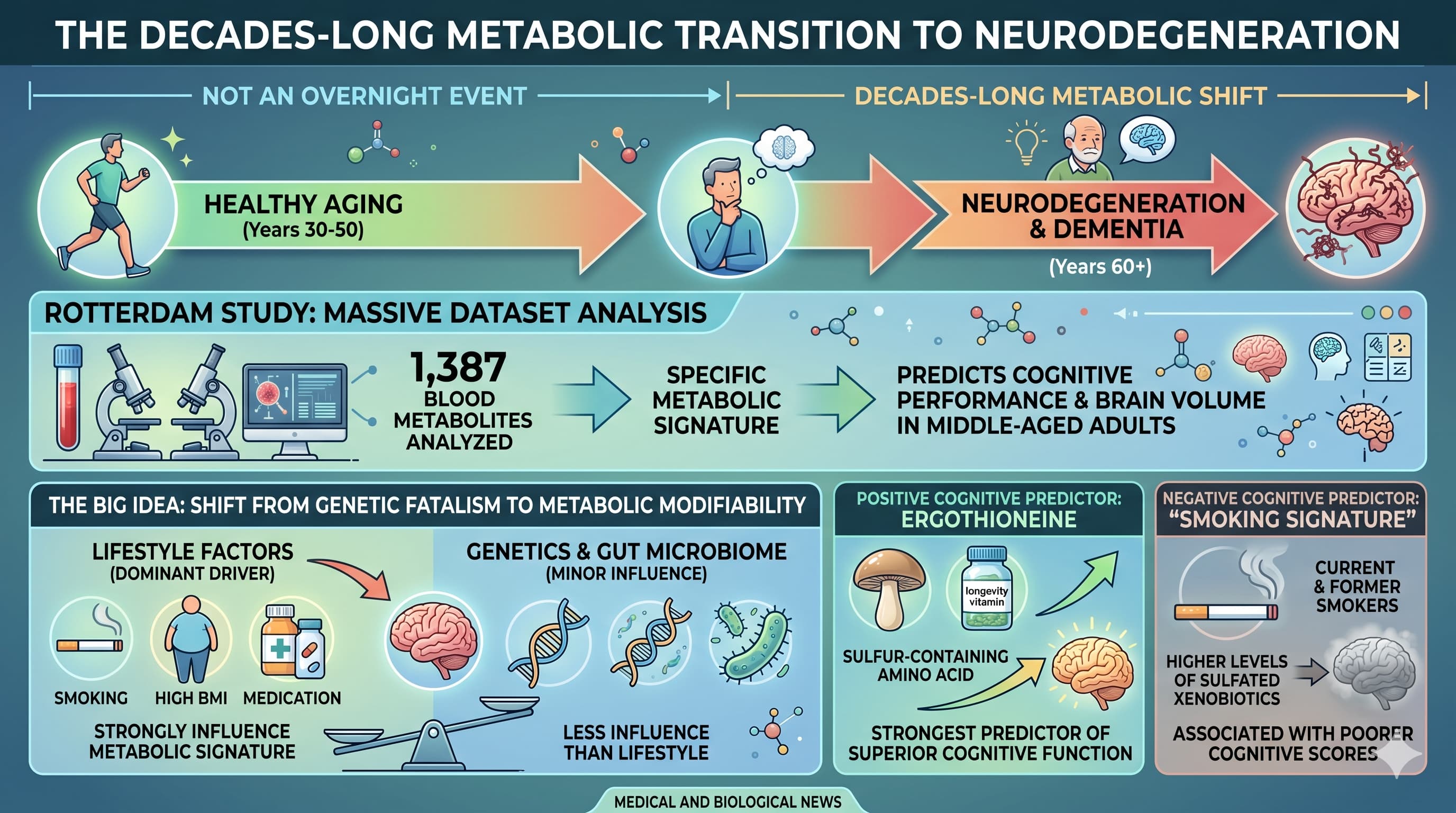
The transition from healthy aging to neurodegeneration is not an overnight event but a decades-long metabolic shift. New research from the Rotterdam Study , utilizing a massive dataset of 1,387 blood metabolites, has identified a specific “metabolic signature” that predicts cognitive performance and brain volume in middle-aged adults long before clinical symptoms of dementia appear.
The “Big Idea” here is the shift from genetic fatalism to metabolic modifiability. While we often view Alzheimer’s risk through the lens of unchangeable genes, this study found that lifestyle factors —including smoking, BMI, and medication use—drive the variance of these brain-health metabolites far more than genetics or even the gut microbiome.
The most significant finding centers on ergothioneine , a sulfur-containing amino acid often dubbed a “longevity vitamin”. Higher levels of ergothioneine were the strongest predictor of superior cognitive function. Conversely, the study identified a “smoking signature” in the blood: current and former smokers carry higher levels of sulfated xenobiotics, which are directly associated with poorer cognitive scores.
Perhaps most alarming for the modern consumer is the discovery regarding antacids (proton pump inhibitors). The research provides a mechanistic “smoking gun” for why chronic antacid use is linked to dementia: these drugs significantly lower blood levels of the neuroprotective ergothioneine. In fact, the loss of ergothioneine explains nearly 31.5% of the negative impact antacids have on cognition.
By mapping how modifiable behaviors like alcohol intake, weight management, and medication choices influence the peripheral metabolome, researchers are moving closer to personalized prevention strategies that could “stabilize” the brain’s environment decades before the onset of Alzheimer’s disease.
Actionable Insights
Prioritize Ergothioneine Intake: Given its robust association with better cognition and neuroprotection, increasing ergothioneine through diet (primarily mushrooms) is a logical longevity intervention.
Audit Antacid Use: Chronic use of proton pump inhibitors (PPIs) is linked to lower ergothioneine levels and cognitive decline. Users should consult clinicians to see if these can be tapered or replaced, especially if cognitive health is a priority.
Smoking Cessation is Non-Negotiable: Smoking leaves a metabolic “residue” of sulfated xenobiotics that correlates with brain aging; these effects persist in former smokers, emphasizing the need for early cessation.
Metabolic Health Drives Brain Volume: MRI markers for brain volume were strongly influenced by BMI and diabetes. Maintaining glycemic control is essential to preserve structural brain integrity.
Monitor Alcohol Intake: Alcohol consumption was significantly linked to alterations in 20 out of 22 metabolites associated with MRI markers of brain health.
Institutions: Erasmus MC (Netherlands), Duke University (USA), Helmholtz Zentrum München (Germany), and Oxford University (UK) .
Country: Netherlands, USA, Germany, UK .
Journal:medRxiv (Note: This is a preprint and has not yet undergone formal peer review), Posted December 16, 2024.
Impact Evaluation: The impact score of this journal is N/A (Preprint server), However, the study is part of the high-prestige Alzheimer’s Disease Metabolomics Consortium.
The following claims were extracted from the research paper and evaluated based on the hierarchy of evidence, ranging from Level A (Meta-analysis) to Level E (Expert Opinion).
1. Ergothioneine & Neuroprotection
Claim: Higher blood levels of ergothioneine are associated with better general cognition and a lower risk of incident Alzheimer’s Disease (AD).
Verification:
External Support: Numerous observational studies confirm that plasma ergothioneine levels are significantly lower in individuals with mild cognitive impairment (MCI) and dementia compared to healthy controls Ergothioneine - ADDF (2022).
RCT Progress: A double-blind, placebo-controlled trial is currently evaluating the efficacy of ergothioneine to delay cognitive decline in elderly subjects NCT03641404 (2024).
Evidence Level:Level C (Human Observational) for the association; Level B (Human RCT) is currently in progress.
2. Antacid (PPI) Use & Ergothioneine Depletion
Claim: Antacid medication significantly lowers ergothioneine blood levels, explaining approximately 31.5% of the negative association between antacids and cognition.
Verification:
External Support: While the broader link between PPIs and increased dementia risk is well-documented in observational data Pourhadi et al. (2024), the specific mediation through ergothioneine is a novel finding from the Rotterdam Study Ahmad et al. (2024).
Evidence Level:Level C (Human Observational). Note: This mediation percentage is specific to this cohort and requires external replication.
3. N-Lactoyl Amino Acids & Metabolic Health
Claim: N-lactoyltyrosine is associated with diabetes and BMI; higher levels are linked to lower brain volume.
Verification:
External Support: There is high-level evidence that N-lactoyl amino acids (specifically Lac-Phe) are “anorexigenic” metabolites that increase significantly with metformin use and exercise to regulate body weight Xiao et al. (2024).
Association with Brain: The link between type 2 diabetes and cortical brain atrophy is established through systematic reviews Frontiers in Dementia (2024).
Evidence Level:Level B (Human RCT/Cohorts) for metabolic signaling; Level C (Human Observational) for the association with brain volume.
4. Sulfated Xenobiotics & Smoking-Related Decline
Claim: Smoking is associated with higher levels of seven sulfated xenobiotics (e.g., o-cresol sulfate) which correlate with worse cognitive performance.
Verification:
External Support: Recent research (2026) has identified a “lung-brain axis” where smoking triggers chemical signals (exosomes) that disrupt neuronal iron balance and increase neurodegeneration markers University of Chicago News (2026).
Evidence Level:Level C (Human Observational).
5. Gut Microbiota & Imidazole Propionate (ImP)
Claim: Imidazole propionate, a gut-derived metabolite, is associated with lower cognitive scores and incident AD.
Verification:
External Support: Longitudinal data in over 1,100 adults link higher plasma ImP levels to lower preclinical cognitive scores and biomarkers of neurodegeneration Kuehn et al. (2026).
Evidence Level:Level C (Human Observational) with supporting Level D (Mouse Mechanistic) data showing ImP exacerbates AD-like pathology.
Actionable Intelligence
The Translational Protocol (Ergothioneine)
Human Equivalent Dose (HED): * NOAEL-based Calculation: Based on subchronic toxicity studies in rats providing a No Observed Adverse Effect Level (NOAEL) of 800 mg/kg/day.
Math: 800 mg/kg (Rat)×(6/37)=129.7 mg/kg (Human).
Theoretical Safe Limit: For a 70kg adult, the safety limit is ~9.08 grams/day.
Therapeutic Target: Clinical research suggests a daily supplemental dose of 5–30 mg to achieve concentrations associated with the top cognitive quartiles in the Rotterdam study.
Pharmacokinetics (PK/PD): * Bioavailability: Highly bioavailable; oral ET is rapidly absorbed and detectable in red blood cells (RBCs) within 1 hour.
Half-Life: Exceptional retention; estimated whole-body half-life is approximately 1 month due to sequestration in tissues expressing the OCTN1 (SLC22A4) transporter.
Brain Entry: Enters the brain via the OCTN1 transporter; the study indicates that central levels correlate with peripheral blood levels.
Safety & Toxicity: * NOAEL: 800 mg/kg/day (Rat).
LD50: Safety Data Absent (but identified as GRAS - Generally Recognized As Safe by FDA/EFSA).
Drug Interactions: Possible competition for the OCTN1 transporter with medications like metformin, gabapentin, and verapamil (which can abrogate ET’s neuroprotective effects).
Biomarker Verification
To verify target engagement and biological response, monitor the following:
Plasma/RBC Ergothioneine: Direct measurement of circulating and sequestered levels.
Oxidative Damage Markers: Reduction in 8-OHdG (DNA damage) and 8-iso-PGF2a (lipid peroxidation) suggests effective antioxidant signaling.
Neuro-Metabolic Surveillance: Rising N-lactoyltyrosine levels may serve as an early warning of glycemic-driven brain volume loss.
Feasibility & ROI
Sourcing: Available as a dietary supplement (L-Ergothioneine) and highly concentrated in mushrooms (Porcini, Oyster).
Cost vs. Effect: * Cost: ~$30–$50/month for a 10–30 mg daily protocol.
ROI: High. Given the 31.5% mediation of cognitive decline in antacid users, the “cost per cognitive unit saved” is minimal compared to the long-term burden of neurodegeneration.
Part 5: The Strategic FAQ
Is the ET-antacid connection causal? * The study used mediation analysis to show ET accounts for 31.5% of the cognitive deficit associated with antacids, but a formal RCT is required to prove causality.
Why does smoking affect ET if smoking is not its primary source? * Smoking induces a “xenobiotic load” that increases oxidative stress, potentially depleting sequestered ET faster than diet can replenish it.
Does education confound the ET-cognition link? * Associations remained significant after adjusting for education, suggesting a biological effect independent of socioeconomic status.
Can we just eat more mushrooms? * Yes; diet accounts for ~14% of ET variance, and high-ET mushrooms like Porcini can provide therapeutic doses (~528 mg/kg).
Is the gut microbiome the primary driver of these metabolites? * No; lifestyle (smoking/BMI) and medication (antacids) explained significantly more variance than the microbiome in middle-aged adults.
Why was hippocampal volume not significantly associated? * Hippocampal changes may occur later in the disease process, or the cross-sectional power was insufficient for this specific region.
What is the significance of the “smoking residue”? * Sulfated xenobiotics persisted in former smokers, suggesting long-term metabolic signatures of previous environmental exposure.
Is N-lactoyltyrosine a byproduct or a driver of brain atrophy? * It likely reflects systemic glycemic stress and metabolic dysfunction that eventually leads to brain volume loss.
Should all PPI users supplement ET? * The data “strongly suggests” this as a protective strategy, especially given the established safety profile of ET.
Does the OCTN1 transporter efficiency vary genetically? * Yes, the SLC22A4 gene governs ET uptake, meaning some individuals may require higher doses for the same tissue saturation.
Interaction Check: Longevity Stack
Metformin: Potential Competition. Metformin uses OCTN1 and OCT1; co-administration may reduce ET uptake. Monitor plasma ET.
Rapamycin:Compatible/Synergistic. No known interference; ET may buffer oxidative stress while Rapamycin modulates autophagy.
SGLT2i / Acarbose:Compatible. These target glucose pathways; ET protects against the resulting oxidative byproducts.
PDE5 Inhibitors / 17-Alpha Estradiol:No Known Interaction. Current metabolic mapping does not suggest interference.
I still harvest the golden oyster several times a year and dry/grind it for my morning smoothie. I take 7 grams of the powder, so very safe. I forget what percent is actually ergo. Since I sun dry I am getting a bunch of vitamin D too and my level is now 91. Holy crap I was aiming for 55. Could have been my lights too.
I was talking to my AI and found out blasting the pinned fungus for just a couple days as they develop with 450nm light will double the ergo content. Apparently this frequency puts it under so much stress and it makes the ergo to be able to resist. Makes me want to avoid 450 nm light.