I’m pulling this news post out by itself so its easier for people to find:
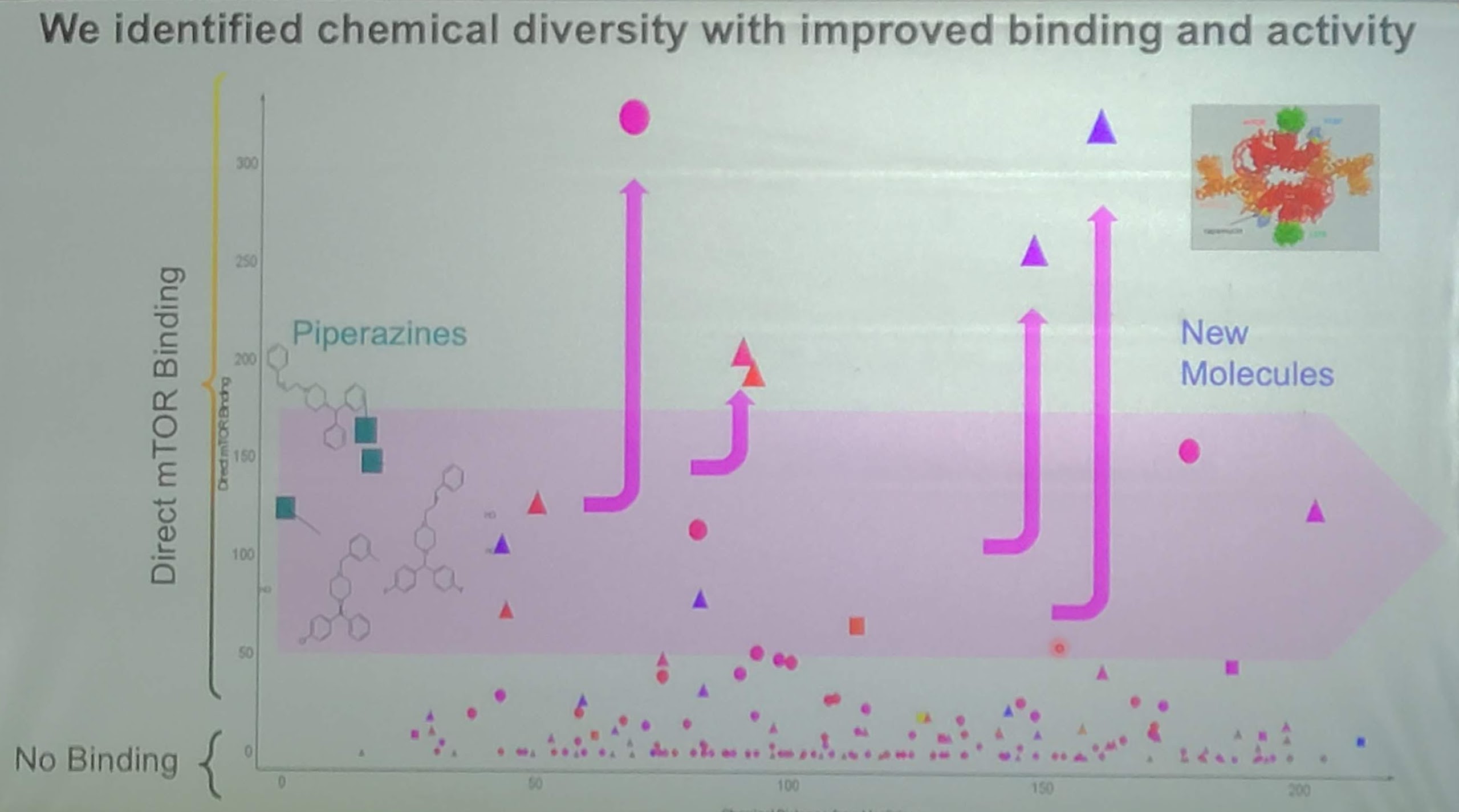
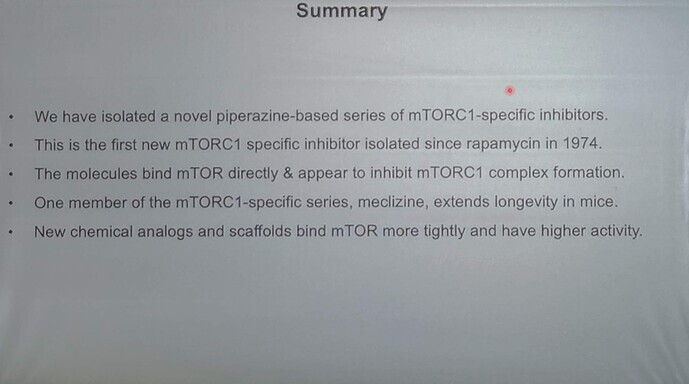
The second BAAM presentation of interest was on focused on a novel mTORC1 inhibitor which in the class of drugs called Piperazines. The drug, called Meclizine, (e.g. brand name Dramamine II) is a common over the counter (available for purchase without prescription) drug for motion sickness.
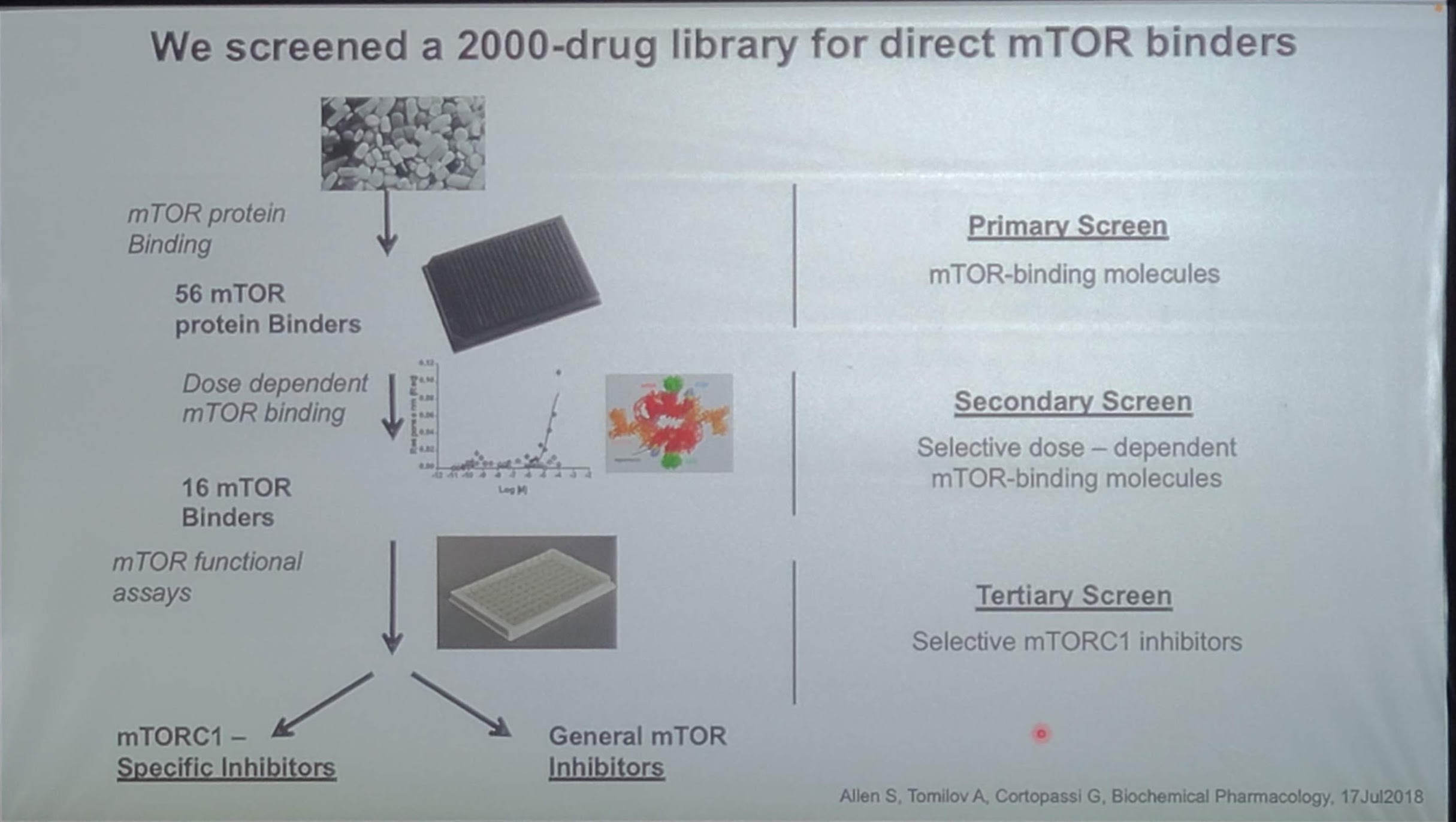
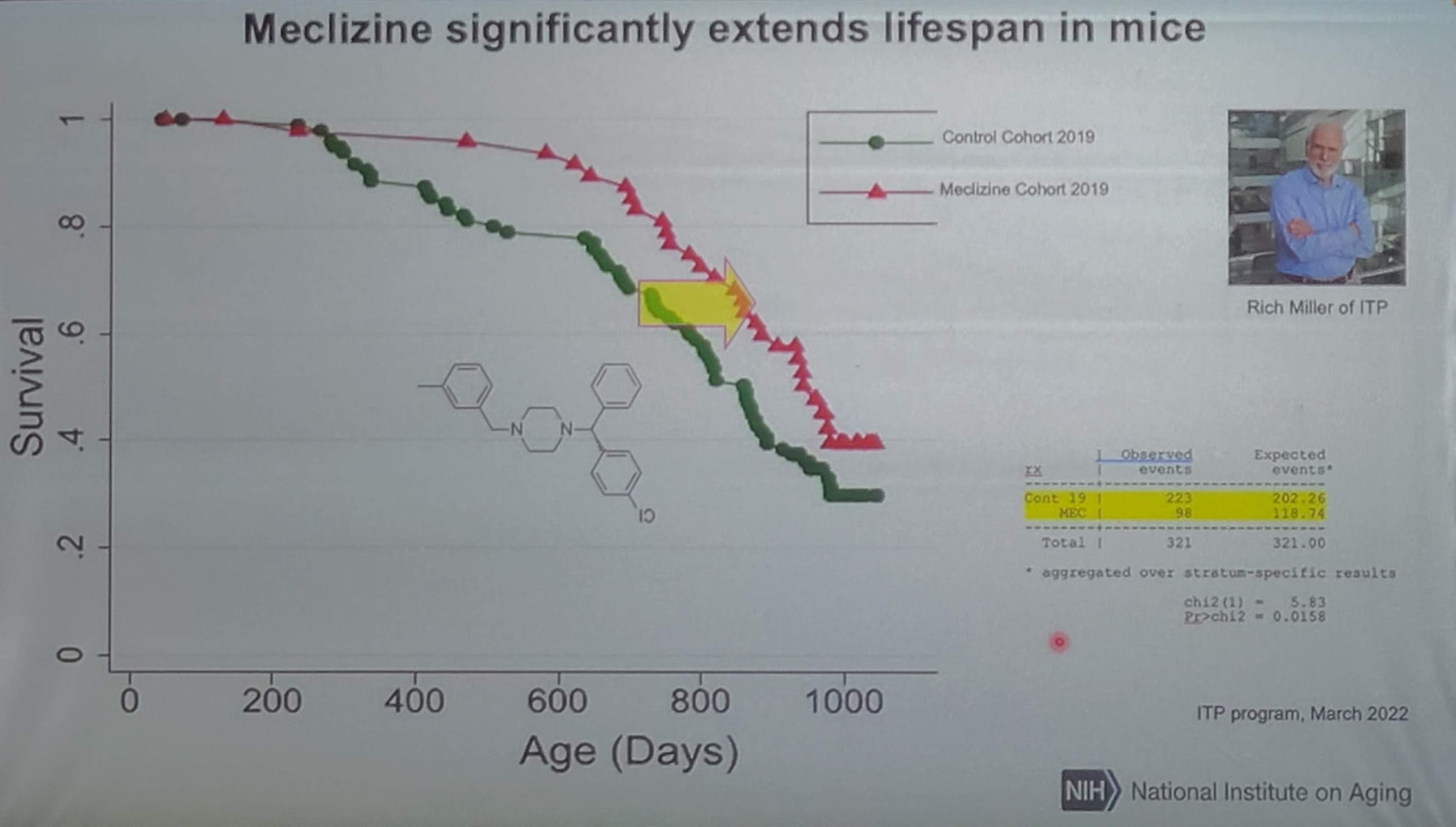
This research reports that Meclizine is an mTORC1 inhibitor that they identified and tested, and which in the NIA ITP program has been revealed to increased mice lifespans by approximately 15% (median lifespan) based on the preliminary data shown with about 75% of the mice deceased (note, this data may be from just one of the 3 ITP sites). The lifespan study is/was being done by Richard Miller and his groups in the ITP program, and the full results have not yet been published or announced. This news from the UC Davis research group is the first I’ve seen that has reported on the Meclizine impact on life extension increase.
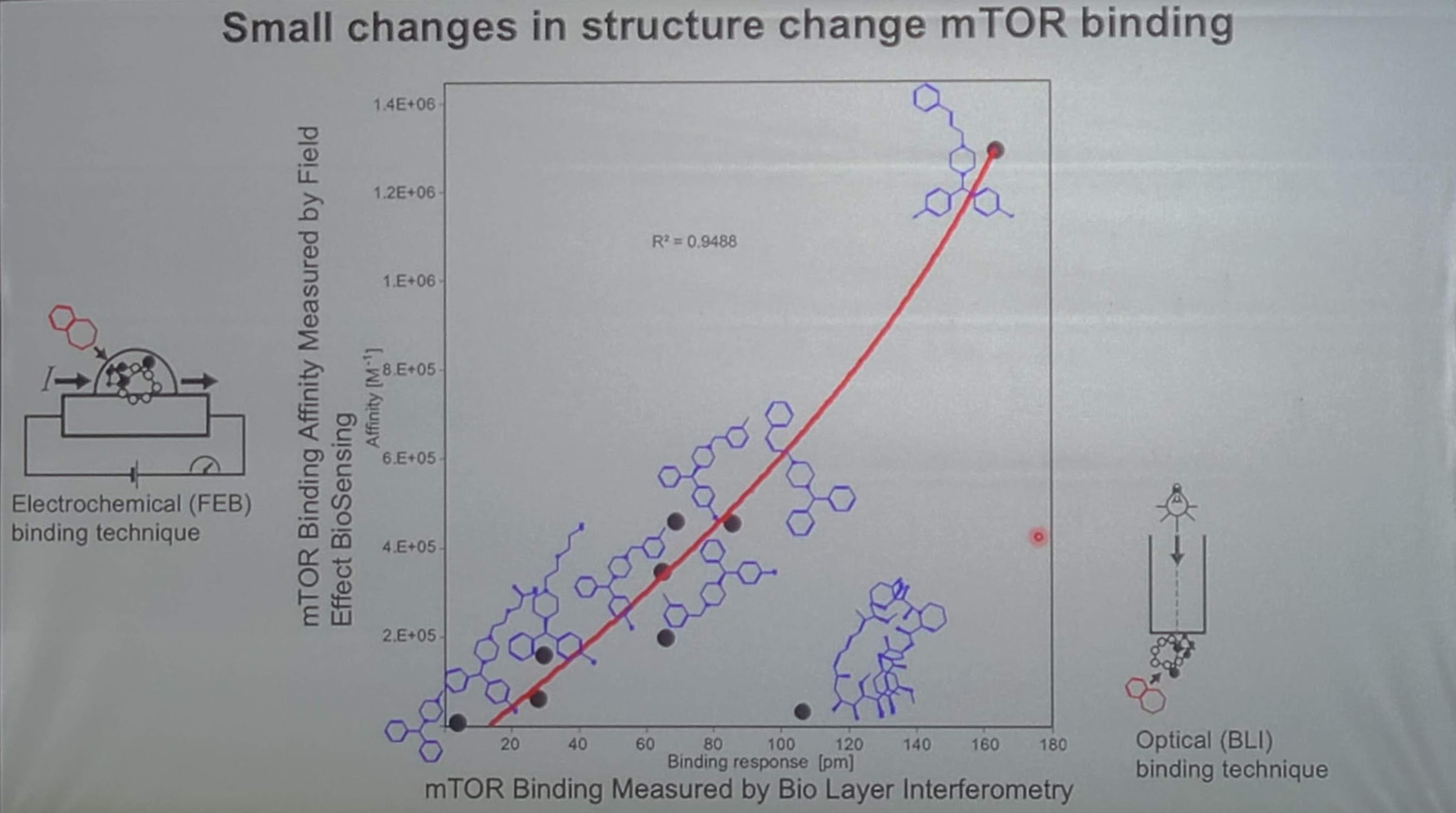
The results with Meclizine have been good, but they are also looking for other drug targets within that general class of mTORC1 inhibitors for something that has a better binding affinity than Meclizine (binding affinity is a key measure of a drug’s ability to target a specific area, the tighter the binding, the fewer “off-target” effects).
Note: In the ITP 2019 study they have been testing 800 ppm in mice). My quick and dirty calculations suggest that 800ppm in mice equates to something like a dose of 300mg/day for a 72kg/160lb human. The key side effect of dramamine is “drowsiness”, so its generally considered a much more benign drug than rapamycin (which can have many negative side effects at high daily doses used in organ transplant and cancer patients).
Another person gave me this dosing calculation (from Louis:
My calculation shows that the ITP fed the mice a human equivalent dose of about 730mg of Dramamine per day for a 70kg person.
Here is the math: The ITP used 800ppm in food (see attached photo). And 800ppm is 0.08%. A typical mouse weighs about 0.025kg and eats about 4g of food per day, so 0.08% is 3.2mg of Dramamine for the mouse per day. That is a dose of 3.2mg/0.025kg=128mg/kg. Divide by 12.3 to allometrically scale to humans, to get a human equivalent dose of (128mg/kg)/12.3=10.4mg/kg. So for a 70kg human, that would be 728mg of Dramamine per day.
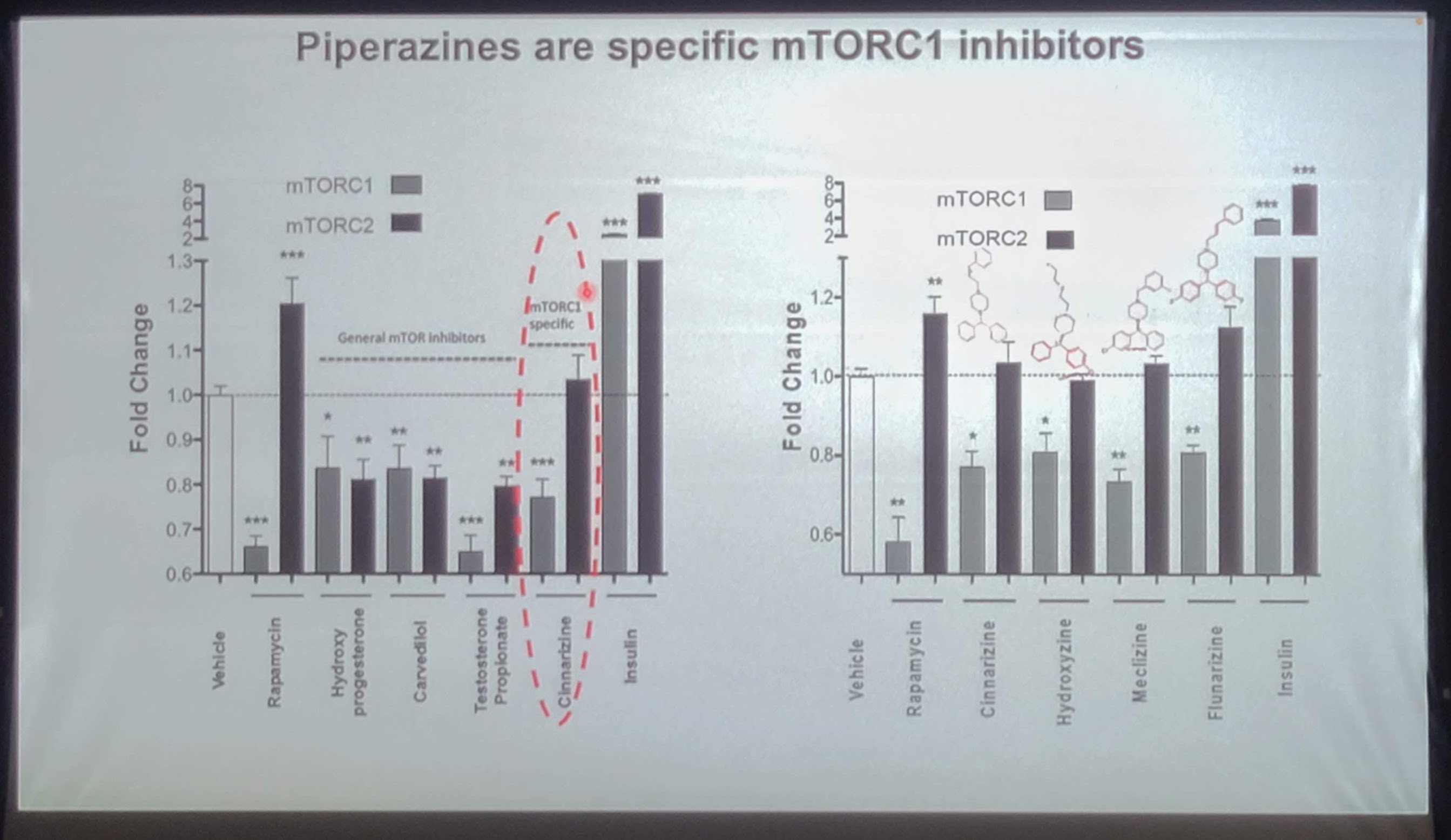
So Meclizine looks to be another drug for longevity that people may want to research. If Meclizine has no impact on mTORC2 in long term administration (it showed no mTORC2 inhibition in a short-term assay), it seems that a dosing strategy in humans that might be evaluated would be some sort of dosing combination of rapamycin and Meclizine. Since people only dose rapamycin for anti-aging once every week or two, perhaps there is a dosing strategy where Meclizine is dosed on some of the days that rapamycin is not taken, that would further increase lifespan and healthspan. This seems to be an area ripe for additional research and/or personal experimentation.
Thank you for all of the work and sharing you do.
Minor note
Dramamine® All Day Less Drowsy is the Meclizine HCI 25mg version.
I have tried it and didn’t notice any drowsiness personally.
Thanks RapAdmin, you are a hero.
In your opinion, would it be smart to cycle Meclizine the same way as with Rapamycin, once a week? Or is it confirmed that this works best as a daily?
Ok, I understand that it is daily dosing now. However if you have enlarged prostate as most guys over 50 have in some ways, you are recommended not to take this…Bummer.
728mg a day for a person at 70 kilo is also a extremely high dose.
There is no indication that Meclizine blocks mTORC2, so daily is likely fine.
Later this summer I think I might try Meclizine - lower doses initially and then slowly increase.
My thinking right now is that I would take it daily for 3 or 4 days on a schedule that is basically opposite to Rapamycin - so on the last 4 days of the week after dosing rapamycin (so if we dose rapamycin on day 1, wait until day 3 or 4 and then dose meclizine for 3 or 4 days). My thinking here is that you don’t want to completely shut down mTORC1, so I’d avoid dosing Meclizine at the same time as rapamycin.
I would take Meclizine just prior to bed, since it can cause drowsiness.
It seems like a fairly low risk medicine, as an over the counter (OTC) drug.
Here is the Meclizine Package Insert - so everyone can read all the details on the drug:
I have taken a lot of Meclizine while sailing offshore. It definitely gets “in your head.” By this I mean you feel a little weird. You can have trouble concentrating, and at higher doses I’ve even had faint hallucinations in my peripheral vision. I think it’s pretty benign, but you’ll certainly notice it more than rapamycin.
Having read up on Meclizine, and gone through the reviews of people using it. I highly advise potential users to also take stinging nettle at the same time. It looks like Meclizine is a potential prostate irritator, just like the first generation anti histamines. If you don’t have a swollen prostate already, take it from me, this is something you don’t want to struggle with. Stinging nettle blocks the conversion of testosterone to DHT. Better be safe than sorry.
neither does rapamycin, which only blocks mtorc1 but chronic mtorc1 inhibition leads to mtor2 inhibition, so it’s likely chronic meclizine use will lead to the same. Personally I would stick to rapamycin, which has only one target (mtorc1) unlike meclizine which has many different targets unless you have a hard time getting rapamycin
As I understood, rapamycin actually inhibits mTOR, which is part or both complexes, that is, its binding site is in fact with mTOR, and while this site stays accessible in mTORC1, it is not with mTORC2. Rapamycin will thus inhibit mTORC1 any time, and it will inhibit mTORC2 before its formation, if it can bind with mTOR. That’s why we must pulse it for antiaging purposes, to limit the inhibition of mTORC2 via the binding with mTOR (before formation of the complex 2). No?
There is a great deal to be learned about mTor inhibition with Meclizine., But, it is definitely an exciting new possibility that should be thoroughly explored. I looked on Ebay and see several sellers offer 1000 25mg tablets for under $40. Meclizine therefore is OTC and very economical. The possibilities should and will be tested. I am very interested in seeing what Dr. Richard Miller and the ITP report.
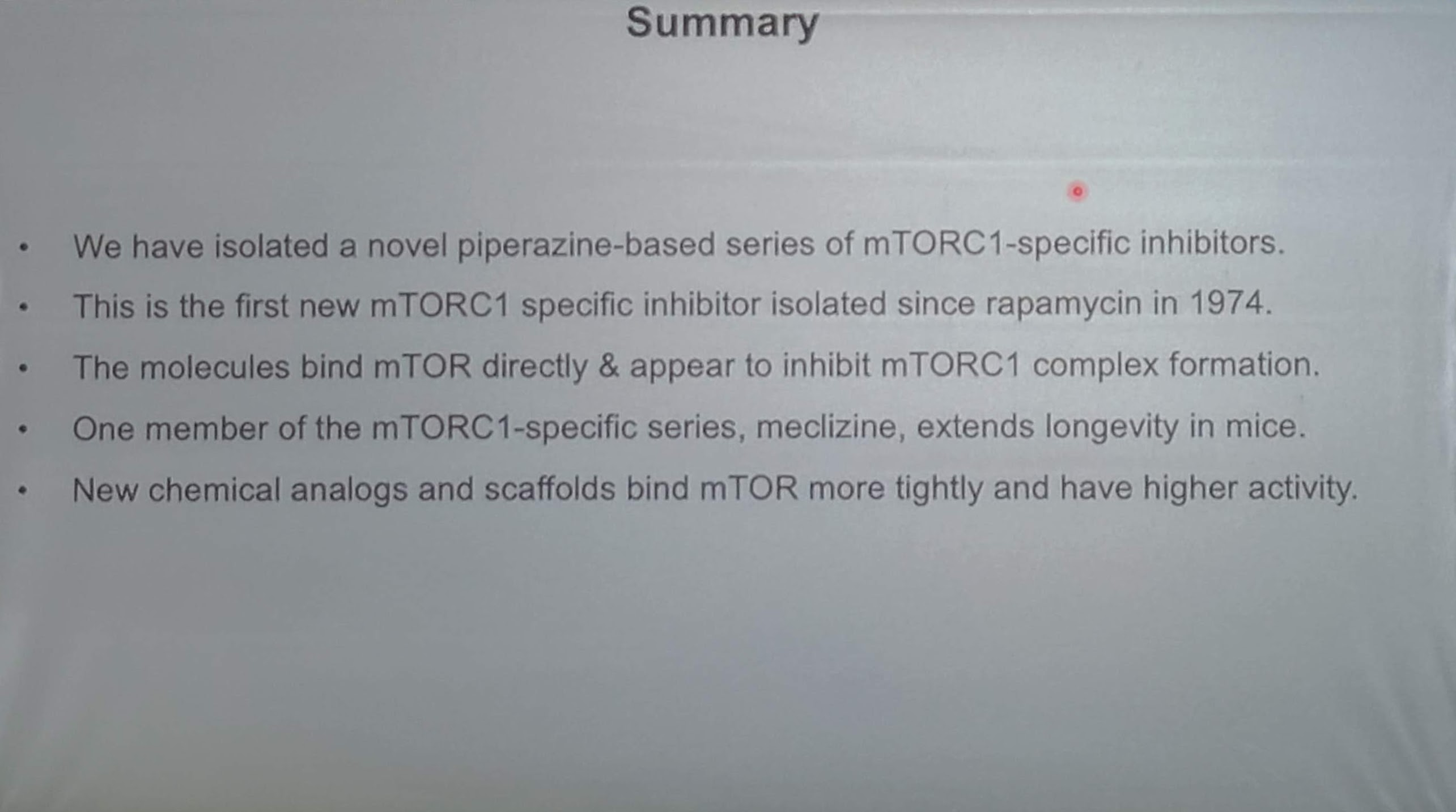
“The molecules bind mTOR directly” and “the first mTORC1 specific inhibitor since rapamycin”?
Either they bind mTOR and will inhibit all mTOR complexes, at least because they will have binded the mTOR that will be included in the complexes, or they bind mTORC1 only, and they are specific.
As I have posted earlier, I tend to sail with the wind. I am too old to do anything else.
At the halfway point of this year, it seems reasonable to me to switch from rapamycin to meclizine. After reading many papers I am looking forward to giving meclizine a trial run.
I will get my blood work done in ~ 3 weeks, ~30 days after my last rapamycin dose which was 15 mg taken with grapefruit juice. This will establish a personal baseline to measure the meclizine results against. The plan is to get my basic bloodwork done monthly.
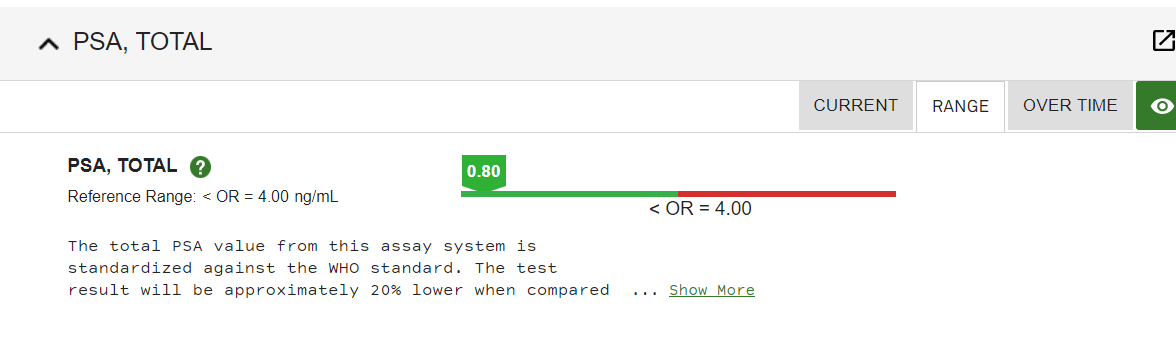
I will be taking meclizine at the 25 mg dose nightly. It was once part of my sleep stack so I am familiar with the possible side effects. It had no effect on my prostate that I am aware of. Meclizine didn’t have any effect on max urine flow. I have been taking tamsulosin for over 25 years and my PSA is 0.80 ng/mL
Meclizine seems to suppress mTORC1 without suppressing mTORC2. This is my main reason for switching at least temporarily.
The fact that meclizine is anticholinergic is not much of a worry to me as these first-generation anti-histamines are being purchased by the boatload by elderly people as part of their constant fight to get a good night’s sleep. The danger, while real, is also small.
To be frank, I have been a little underwhelmed by rapamycin, I don’t doubt its positive effects, but I was hoping for a little more subjective well-being and energy. Perhaps its negative effects on mTORC2 account for that fact, or, maybe I am just too old.
I am excited to be embarking on a new track for a while.
As you can see my doctor only orders this test every few years.
It’s an interesting experiment but I wouldn’t do it. This is especially true in the elderly.
Many drugs have an anticholinergic component and the list of side effects is significant, More than rapamycin actually ,and I’ll frankly be shocked if you feel younger with it, but who knows.
Also, if you’re suppressing mTOR daily, isn’t that similar to what renal transplant patients do?
The difference as I understand it, daily use of rapamycin also suppresses mTORC2. As I said, I have taken meclizine daily, in the evening, in the fairly recent past for 60 days or so, and experienced no adverse effects. I wasn’t aware at the time that it was an mTORC1 suppressor. I will be keeping a close eye on things.