Finally, the official Astaxanthin and Meclizine results and paper out of Richard Miller’s ITP program:
In genetically heterogeneous (UM-HET3) mice produced by the CByB6F1 × C3D2F1 cross, the Nrf2 activator astaxanthin (Asta) extended the median male lifespan by 12% (p = 0.003, log-rank test), while meclizine (Mec), an mTORC1 inhibitor, extended the male lifespan by 8% (p = 0.03). Asta was fed at 1840 ± 520 (9) ppm and Mec at 544 ± 48 (9) ppm, stated as mean ± SE (n ) of independent diet preparations. Both were started at 12 months of age. The 90th percentile lifespan for both treatments was extended in absolute value by 6% in males, but neither was significant by the Wang–Allison test.
The disappointing news:
Five other new agents were also tested as follows: fisetin, SG1002 (hydrogen sulfide donor), dimethyl fumarate, mycophenolic acid, and 4-phenylbutyrate. None of these increased lifespan significantly at the dose and method of administration tested in either sex.
In genetically heterogeneous (UM-HET3) mice produced by the CByB6F1 × C3D2F1 cross, the Nrf2 activator astaxanthin (Asta) extended the median male lifespan by 12% (p = 0.003, log-rank test), while meclizine (Mec), an mTORC1 inhibitor, extended the male lifespan by 8% (p = 0.03). Asta was fed at 1840 ± 520 (9) ppm [!!] and Mec at 544 ± 48 (9) ppm, stated as mean ± SE (n) of independent diet preparations. Both were started at 12 months of age. The 90th percentile lifespan for both treatments was extended in absolute value by 6% in males, but neither was significant by the Wang–Allison test. Five other new agents were also tested as follows: fisetin, SG1002 (hydrogen sulfide donor), dimethyl fumarate, mycophenolic acid, and 4-phenylbutyrate. None of these increased lifespan … https://rd.springer.com/article/10.1007/s11357-023-01011-0
The lifespan data table:
The controls used for the fisetin studies were unusually short-lived, and it couldn’t even pass this low bar. They tried both a cyclic and a continuous dosing protocol, as advised by James Kirkland: no dice.
A median 12% lifespan extension and a trend towards maximum lifespan extension is great news for astaxanthin. I can see why they are testing a dose 5x lower now.
Maybe this will lead to higher dosed astaxanthin entering the market soon?
The Asta supplied by Cardax consisted of synthetic Asta finely dispersed in a water dispersible beadlet formulation. The superior bioavailability of synthetic Asta beadlets compared to microalgal Asta was demonstrated in a human pharmacokinetic study (approximately threefold higher exposure in plasma over 24 h; [66]
[…]
Importantly, synthetic Asta is a pure form of Asta, whereas microalgal and other natural extracts of Asta are complex mixtures of Asta esters, Asta, and other byproducts [68,69,70].
[…]
Synthetic Asta has demonstrated efficacy across a range of human, animal, and cell culture studies, for example [72,73,74], and its excellent safety profile has been well established in rigorous toxicity studies [20, 75].
[…]
Synthetic Asta beadlets are also utilized in the following commercially available dietary supplements: ZanthoSyn® (Cardax, Honolulu, HI) and AX3™ (AX3 Life, Honolulu, HI).
Yes, I have bought it from Amazon.
The question is: Do we need still another mTORC1 inhibitor?
Maybe, if it inhibits mTORC1 but leaves mTORC2 alone.
If it doesn’t affect mTORC2 then it might be worthwhile.
I have used it in the past and found it to be a worthwhile sleep aid. (discussion in another thread)
This is the brand I bought:
Yes… from other threads: Post from Meclizine discussion here:
Here is the math:
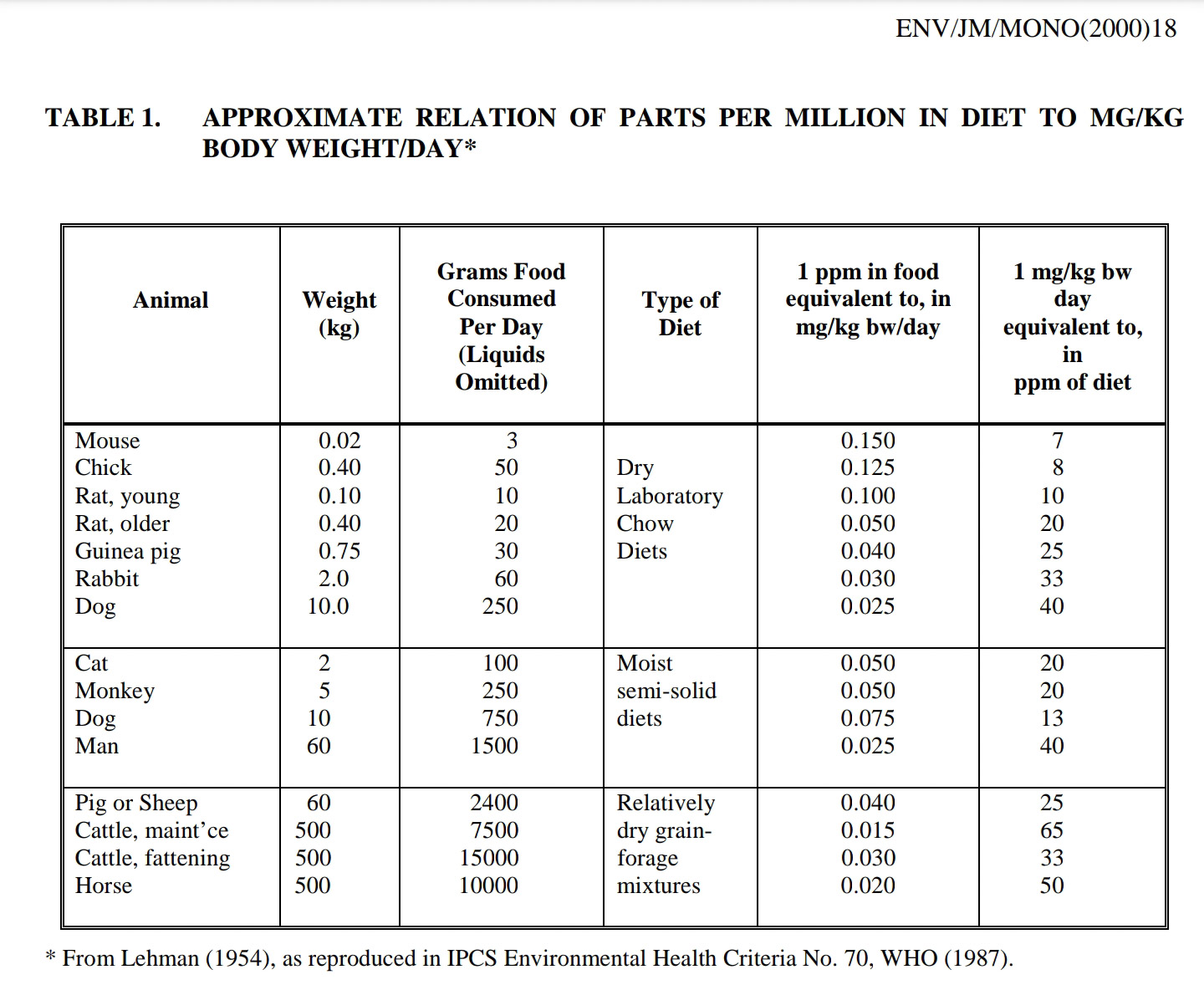
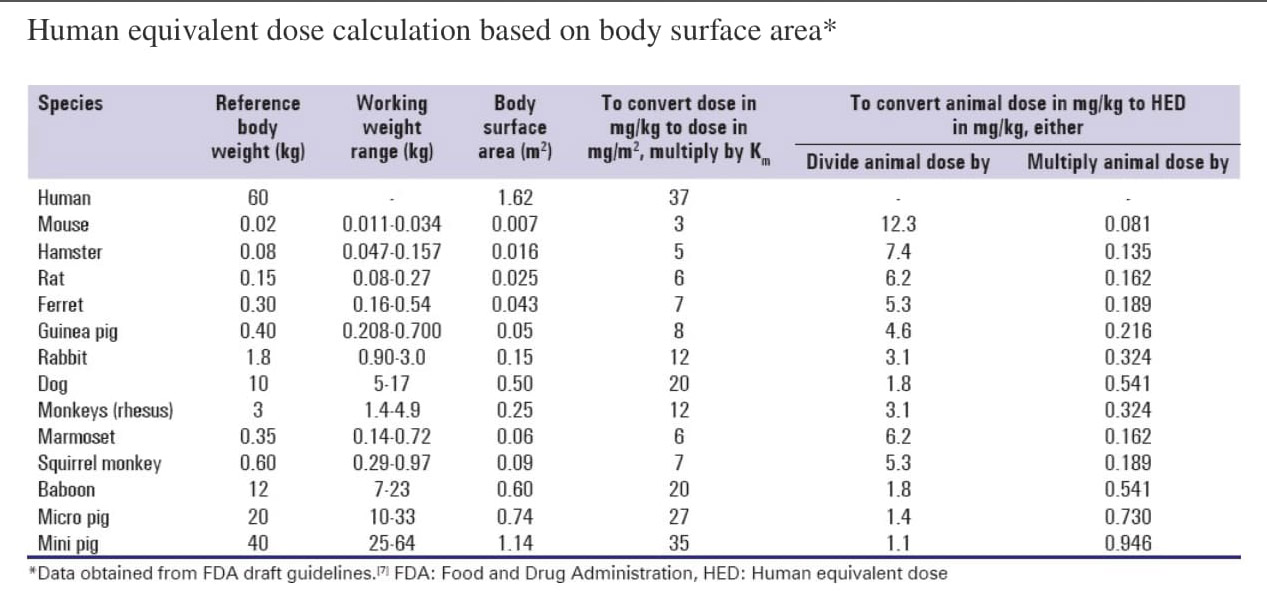
The ITP used 800ppm in food (see attached photo). And 800ppm is 0.08%. A typical mouse weighs about 0.025kg and eats about 4g of food per day, so 0.08% is 3.2mg of Dramamine for the mouse per day. That is a dose of 3.2mg/0.025kg=128mg/kg. Divide by 12.3 to allometrically scale to humans, to get a human equivalent dose of (128mg/kg)/12.3=10.4mg/kg. So for a 70kg human, that would be 728mg of Dramamine per day.
That’s a disappointment. As I’ve said previously, I think DMF is modestly promising. Can anyone with more knowledge on the mouse literature comment on the dosing? In particular, what is the rough human equivalent to the doses they used?
I don’t think that’s meant to be taken literally as perfect translation. Something can be much more potent in humans. Different animals after all.
Does anyone know what the rapamycin dose is in mice studies equivalent to humans?
Different animals, yes — but the HED dose and allometric scaling already take account of a lot of that, and but we have at present no rational reason to suppose that humans would need less rather than more or the expected amount of asta they suggest. I note that the European Food Safety Administration found a NOAEL of 10 mg astaxanthin/kg bw per day (in rats, so do the full conversion) based on prothrombin time (bleeding) and some evidence of liver toxicity. https://efsa.onlinelibrary.wiley.com/doi/epdf/10.2903/j.efsa.2014.3757
See this handy if depressing table from our intrepid administrator:
Can we use what is deemed safe in humans afaik (0.5 mg a day or 5 mg weekly) rapamycin, and base the dose of astaxathin on it? From information of mice-safe human conversion?
(*) Nair A, Morsy MA, Jacob S. Dose translation between laboratory animals and human in preclinical and clinical phases of drug development. Drug Dev Res . 2018;79(8):373-382. doi:10.1002/ddr.21461.
(**) Nair AB, Jacob S. A simple practice guide for dose conversion between animals and human. J Basic Clin Pharm . 2016;7(2):27-31. doi:10.4103/0976-0105.177703
I’m sure baby doses of Astaxanthin have some effect. Whether that is the full effect or not is debatable. It does seem to help prevent sunburn at a 10 mg daily dose.