FWIW
Klickstein states there should be a break.
Review Attia interview;
#118 – Lloyd Klickstein, M.D., Ph.D.: Rapamycin, mTOR inhibition, and the biology of aging
FWIW
Klickstein states there should be a break.
Review Attia interview;
#118 – Lloyd Klickstein, M.D., Ph.D.: Rapamycin, mTOR inhibition, and the biology of aging
We certainly don’t know the long-term safety effects of rapamycin either.
I can’t find any long-term safety studies for meclizine, but it has been around for a long time and I don’t see any particular warning flags other than the anticholinergic effect.
I also think mTORC1 suppression is dose-dependent with meclizine, as it is with rapamycin.
The 25 mg. daily dose of meclizine is at the low end of dosages used in studies.
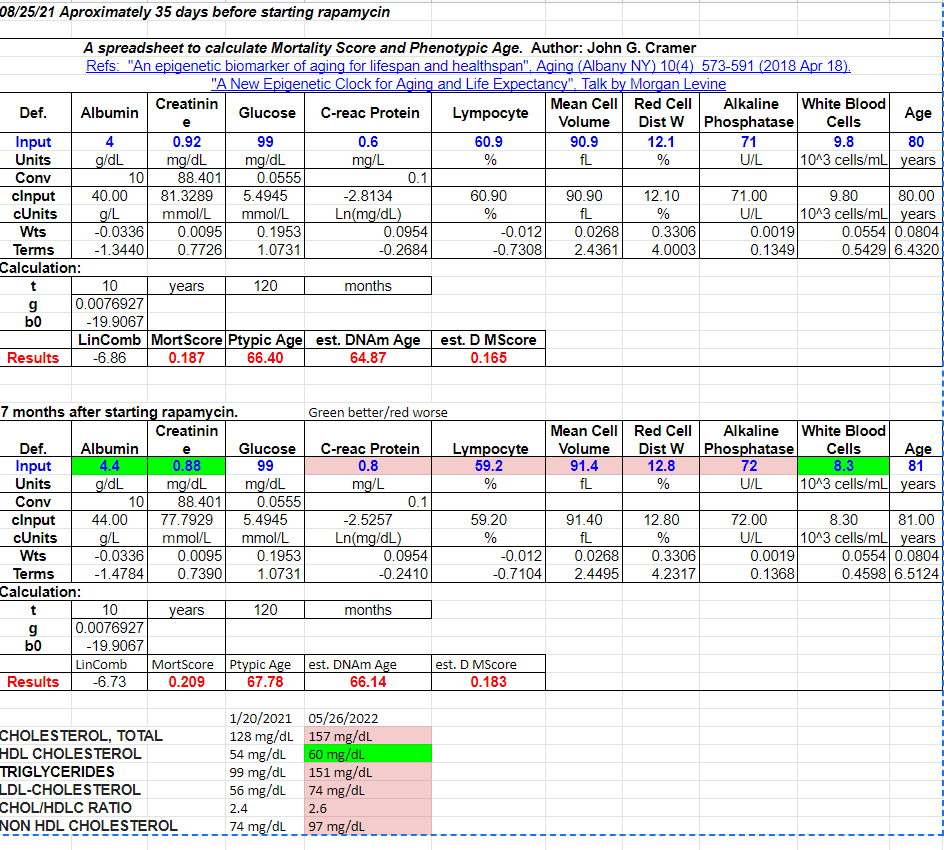
Because I was already in pretty good shape from using keto and time-restricted feeding, both of which lower mTORC1, my Levine spreadsheet biomarkers were not improved by the use of rapamycin for 8 months.
Only my HDL improved, and that is a questionable marker. Meanwhile, my lipid panel certainly took a turn for the worse.
Two other adverse effects I noted were delayed wound healing, especially if happened right after a dose of rapamycin, and the thinning of my fingernails.
“side effects associated with long-term rapamycin treatment, many of which are due to inhibition of a second mTOR complex, mTORC2, have seemed to preclude the routine use of rapamycin as a therapy for age-related diseases.”
In any case, I will keep a close eye on my physical and mental health while taking meclizine.
“A study evaluated the memory effects of meclizine 25 mg, lorazepam 1 mg, promethazine 25 mg”
“The authors found that meclizine produced the least amount of detrimental memory effects in that it did not significantly decrease overall accuracy of answer choices or increase the time to make a choice,”
“Since 1962, there have been several trials demonstrating meclizine’s safety in pregnancy.29,30 One study evaluated a total of 50,282 mother-child pairs.30 Of these, 1,014 mothers had taken meclizine during the first four months of pregnancy. The rate of all malformations combined among those not exposed to meclizine was similar to that in the exposed group”
Meclizine: Safety and Efficacy in the Treatment and Prevention of Motion Sickness
https://journals.sagepub.com/doi/full/10.4137/CMT.S6237
“Moderate Inhibition of mTORC1 Signaling is Sufficient to Extend Lifespan and Healthspan
Fascinatingly, short-term late-life rapamycin treatment is sufficient to extend longevity”
“side effects associated with long-term rapamycin treatment, many of which are due to inhibition of a second mTOR complex, mTORC2, have seemed to preclude the routine use of rapamycin as a therapy for age-related diseases.”
I stand to be corrected, but I thought fingernails/toenails constantly thickened with age, therefore the thinning of such might be a sign of turning the clock back???
I would do a washout period, though. It will be interesting to see whether your lipids then improve, how much and how fast. If they improve well and fast, it might indicate that you dosed rapamycin too aggressively.
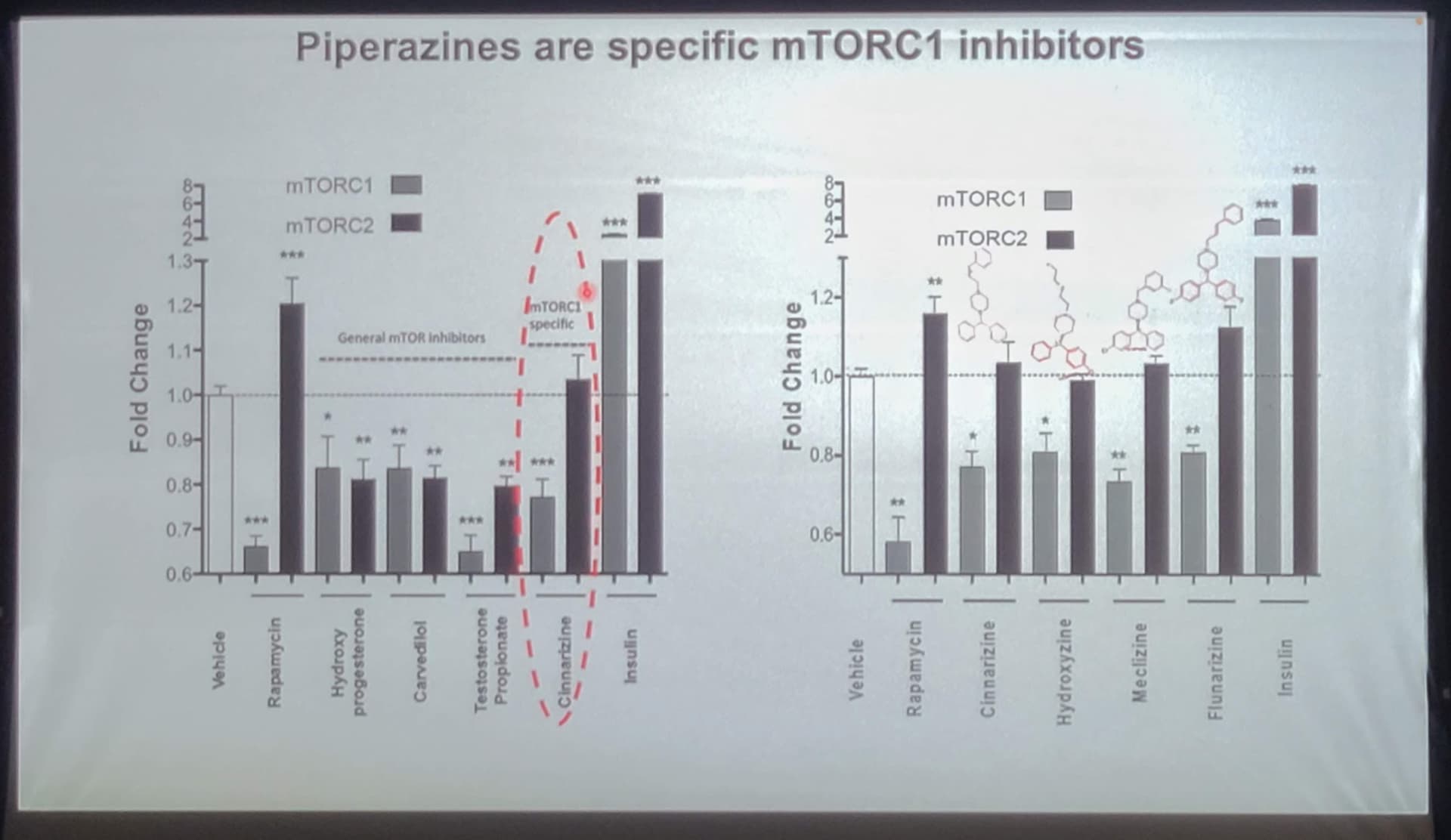
And I have to say I’m still skeptical about that “specific mTORC1 inhibitor”. Actually, when you look at the results on the slide above (that I copy below), it looks like C1 is less inhibited by this new candidate than by rapamycin, while C2 is more inhibited. But perhaps I don’t read it correctly?
The only clearly positive point of those slides (to my eyes) is the extended lifespan in mice.
Yes - that is true. In this study, Meclizine was not as good an mTORC1 inhibitor as was rapamycin, but the reason they are looking at all these drugs is that they would like to find a drug with similar (or at least close) mTORC1 inhibition, but no mTORC2 inhibition (and therefore, the theory goes, fewer negative side effects such as immune suppression at high doses).
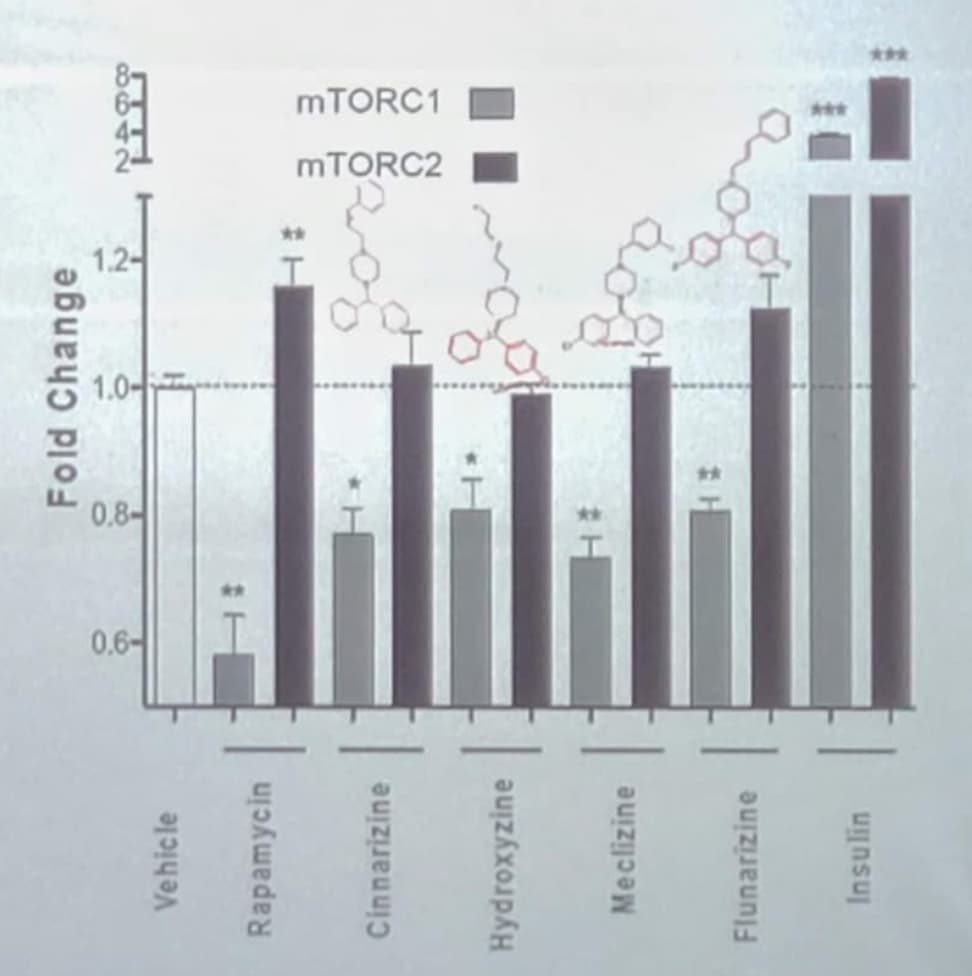
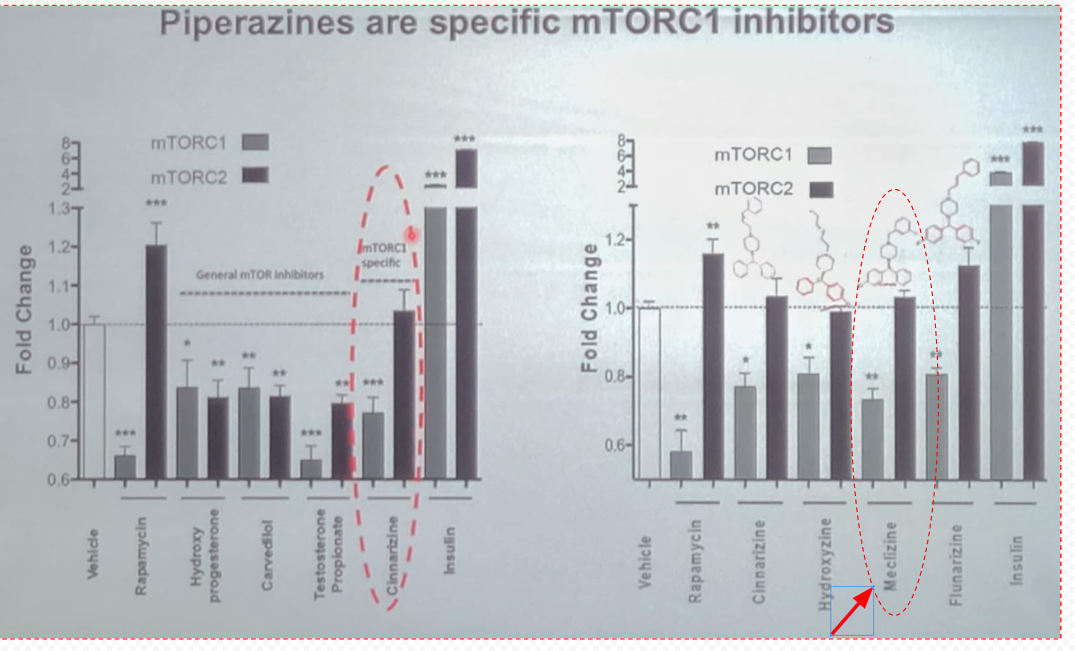
In the above slide (I’ve pulled out the one graph to focus on below) you can see that Meclizine is the best of this bunch (other than rapamycin) at inhibiting mTORC1, with minimal effect on mTORC2. An interesting question that was brought up earlier in this discussion is whether mTORC2 inhibition naturally starts happening over time any time you start inhibiting mTORC1 for longer periods of time? This is a good question - we’ll need to ask the researchers about this issue.
An Additional note - the other drugs listed here all do a pretty good job (other than Insulin, obviously, which I think was just included for comparison to something that obviously has a pro-aging effect with the IGF-1 connection). So the drugs:
Would all seem to be good potential anti-aging drugs also. I suspect that all of them likely increase lifespan if they were tested in mice. If someone has the time - perhaps they can look into these mTORC1 inhibitors also - and see if any of them have obviously better side effect profiles.
We need to look more into this - its an area I have not explored. It seems there is a scale of anticholinergic drugs, and since Meclizine is not listed as one of the typical anticholinergic drugs, I wonder how anticholinergic it is relative to the other drugs on that list.
I do see this when I look up anticholinergic drugs:
Conflicting conditions
Anticholinergics can be used to treat many conditions, but they aren’t for everyone. For example, these drugs aren’t usually prescribed for older people.
Anticholinergics are known to cause confusion, memory loss, and worsening mental function in people who are older than 65 years. In fact, recent studiesTrusted Source have linked use of anticholinergics with increased risk of dementia.
Also, people with the following conditions shouldn’t use anticholinergics:
- myasthenia gravis
- hyperthyroidism
- glaucoma
- enlarged prostate
- hypertension (high blood pressure)
- urinary tract blockage
- increased heart rate (tachycardia)
- heart failure
- severe dry mouth
- hiatal hernia
- severe constipation
- liver disease
- Down syndrome
This research paper below is cited in the above reference on Healthline.com:
gray2018.pdf (631.8 KB)
There are certainly some pros and cons.
Pros:
Cons:
Not unless you’re talking baby. My fingernails became very thin and tear easily.
More on this topic of anticholinergic drugs and brain impact. It seems that Meclizine is a pretty strong anticholinergic, and is high on the anticholinergic cognitive burden scale. See below.
In 2008, Indiana University School of Medicine geriatrician Malaz Boustani developed the anticholinergic cognitive burden scale, which ranks these drugs according to the severity of their effects on the mind. It’s a good idea to steer clear of the drugs with high ACB scores, meaning those with scores of 3. There are so many alternatives to these drugs.
NOTE: Meclizine has a score of 3, on the cognitive burden scale as shown below. (So this is not looking good in that respect)
Source: Harvard Health
Anticholinergic-cognitive-burden-scale.pdf (309.4 KB)
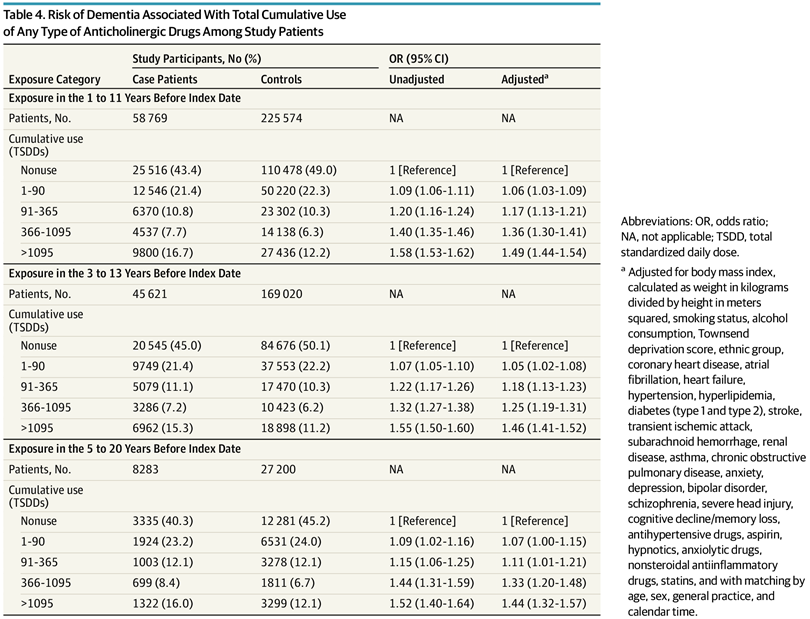
Here is a large, recent study published in JAMA on this topic:
According to my reading, Meclizine does not suppress mTORC2. Perhaps someone more expert in these things can interpret this chart?
As I posted before, the primary cause of dementia is old age.
Yes - that is true. I had a video call with the researchers to discuss the paper (they were very friendly and accommodating).
They did the assay only once, after I think a single dose. So while we know meclizine doesn’t have a direct impact on mTORC2, we don’t know if there are subtle feedback loops with mTORC1 or other pathways that could eventually (with daily use) result in mTORC2 inhibition (as with rapamycin). I encouraged the researchers to do a longer-term study to see if this might be the case.
True, and as the researchers in the JAMA study mentioned:
The researchers are quick to caution that the association isn’t necessarily causal – meaning, there could be other factors among this group of people that increases the risk. If it is a cause and effect relationship, however, the authors point out that anticholinergic drugs could account for 10% of all dementia diagnoses.
Thank you. The bottom line for me right now is to try something new, as rapamycin has not done anything positive for me that I can tell. I achieved good results on the Levine aging spreadsheet by using the tried and true methods of, diet, exercise, and previously taking antiaging supplements known to me at the time, namely; melatonin, metformin, lithium rotate, and a few others. Here are the results of my rapamycin adventure:
(As you can see the primary result was an increase in lipid levels)
It’s an interesting discussion.
A colleague of mine with no medical history tried rapamycin at about the same time that I did. He felt no effects after several months and stopped it.
But he didn’t have much of a comparison point since he felt perfectly fine to begin with.
You’re not going to feel, and it’s very difficult to measure things like autophagy, mitophagy, decrease in cell proliferation and cell size, cancer inhibition, stem cell rejuvenation, cardiac output, immune enhancement especially viral, inhibition of geroconversion senescence, and possible cardiovascular and dementia prevention. Almost forgot longevity.
Will meclizine exceed those effects that have been fairly well studied of rapamycin?
Will the side effects be more clinically relevant?
Let us know, but a fair trial to compare the two may take a while.
I just looked over some of my past responses and to be sure there were two very positive effects. My actinic keratoses cleared up and my “essential tremors” went away. Not sure about absolute cause and effect.
One reason I didn’t feel any subjective improvements is because I was in good health when I started, and remain, essentially pain-free. At my age, at least for me, I am looking for increased energy, stamina, and endurance beyond what is normal for my age.
Actually, those improvements are significant. The one involves pre cancerous lesions and the other a genetic neurological tremor, and both in about a 6 month time frame. Nothing to sneeze at.
Energy can be challenging. For me it depends on a great night sleep, first and foremost , and then not overdoing the exercise.
After that, I like 600 mg of pine bark, NR 2-3 times a week max, a good dose of coffee, and even boron 3 mg.
Just looking more at these drugs… Hydoxyzine is another anticholigenergic drug, so again the same side effects as meclizine.
The other two drugs however are not on the list so may not have the same side effect issues:
These common side effects happen in more than 1 in 100 people.
Talk to your pharmacist or doctor if the side effects bother you or do not go away:
- feeling sleepy during the daytime
- feeling sick
- indigestion
- putting on weigh
People with the following conditions should discuss taking flunarizine with their doctor.
The main side effects of flunarizine are tiredness, drowsiness, weight gain and low mood.
- Tiredness and drowsiness can be reduced by starting with a low dose and taking it at night. The dose will then be increased gradually once your child becomes tolerant to these effects. Some patients experience a second wave of tiredness after several weeks or months and it would be advisable to either try a lower dose or use the medicine on alternate days. This should be discussed with your doctor
- Possible weight gain is caused by an increase in appetite and can be avoided by your child following his or her usual diet without any increase in portion size. In our experience, this happens in one in ten children taking the medicine.
- If your child develops low mood or depressive symptoms, the medicine should be discontinued. You should take advice from your family doctor (GP) whether specific treatment may be necessary for the treatment of depression if the symptoms do not disappear within one month.
There have also been reported cases of flunarizine causing symptoms as seen in Parkinsons’s Disease (extrapyramidal symptoms) which usually disappear when flunarizine is stopped. Other side effects that have been reported include: sickness and upset stomach, insomnia, dry mouth, weakness and muscles aches, and a skin rash. If you are concerned about any of these, please tell your doctor.
Cinnarazine would be worse since one of its side effects involves the extrapyramidal reaction of tardive dyskinesia. Sometimes irreversible and caused by depleting dopamine.
Not good especially in the elderly.