Is it better than blueberry or other anthocyanins do you think?
Oops…
Results . LDL increased with pterostilbene monotherapy (17.1 mg/dL; ) which was not seen with GE combination (). Presence of a baseline cholesterol medication appeared to attenuate LDL effects. Both systolic (−7.8 mmHg; ) and diastolic blood pressure (−7.3 mmHg; ) were reduced with high dose pterostilbene. Patients not on cholesterol medication () exhibited minor weight loss with pterostilbene (−0.62 kg/m2; ). Conclusion . Pterostilbene increases LDL and reduces blood pressure in adults.
https://www.clinicalnutritionjournal.com/article/S0261-5614(18)32477-4/fulltext
However, as summarized in Table 1, daily administration of NR plus pterostilbene produced a dose-dependent and clinically statistically significant increase in total cholesterol driven entirely by increased low density lipoprotein cholesterol (LDL-C).
You would need to eat several pound’s of blueberries.
FWIW
1 Like
From the paper you posted
“(1) pterostilbene 125 mg twice daily; (2) pterostilbene 50 mg twice daily; (3) pterostilbene 50 mg + grape extract (GE)”
These where very low amounts.
FWIW
I would be taking 1g per day minium.
But this clinical trial suggests that it would increase your LDL-C! How can that be desireable?
1 Like
I am more interested in
…“protects vascular endothelial cells against oxidized low-density lipoprotein”…
In short I am in the camp that oxidized lipoprotein in between the endothelial cells and the blood vessels walls is the major issue/problem. There are some people{one of Attia’s patients as covered in his podcast # 07]with cholesterol levels over 500 and they have a 0 calcium score.
I repeat this - We are all looking for the black cat in the dark room.
Science is not what most people think it is.
As per – Stuart Firestein, The pursuit of Ignorance.
1 Like
Well, that protection was demonstrated in model organisms, so it is a “maybe”, whereas the higher LDL-C was observed in a clinical trial, so it is almost certain. And yes, some people have high LDL-C but zero plaque, it can happen, but it is another maybe.
This is a scary game, not science. But good luck!
2 Likes
Very few thing are “almost certain”
FWIW
The paper you referenced has;
"Conflict of interest
CB developed intellectual property exclusively licensed and developed by ChromaDex for nutritional and therapeutic uses of NR."
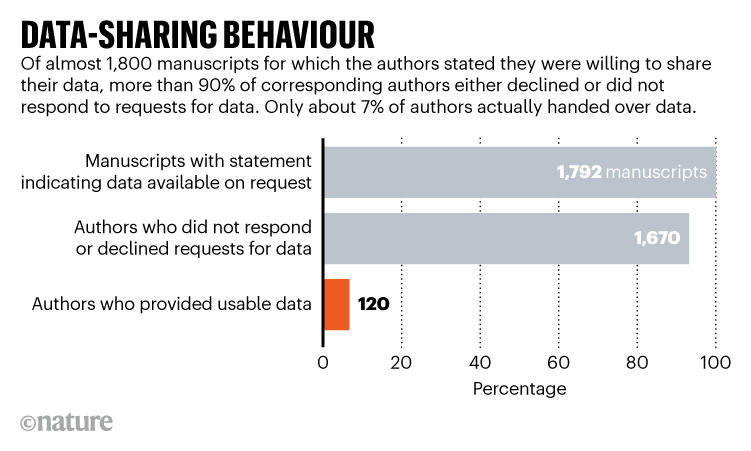
They did not even publish the data.
“The authors did not release their primary data for independent assessment of significance and did not disclose results previously reported for pterostilbene”
1 Like
The conflict of interest is about NR, not about PT.
And as for publishing the data, you cannot say “not even”: not publishing data is the rule, alas…
FWIW
n=1
At the cost of less than $1.56 a day for 1,000mg of pterostilbene for 30 day, my order for the pterostilbene is in.
My assayed rapamycin powder is taking longer.
I keep looking for the black cat in the dark room.
Still trying to sound profound but actually sounding a bit silly…
If a molecule fails the ITP it doesn’t deserve attention here.
In your view.
Not in others.
2 Likes
Pterostilbene failed the ITP?
Where did you source that? All dosages I see are much lower (50 to 150 mg)
Rapamycin increased my LDL_C. How can that be desirable?
Indeed. And as you wrote recently,
To be frank, I have been a little underwhelmed by rapamycin, I don’t doubt its positive effects, but I was hoping for a little more subjective well-being and energy. Perhaps its negative effects on mTORC2 account for that fact, or, maybe I am just too old.
Higher LDL-C are very problematic, and should be a sign that an intervention is not desirable. There may be exceptions to this rule, as there almost always are. But in the case of higher LDL-C, I think that the line is very thin. When I’ll try it, if my LDL-C goes up as a result, I’ll call it quit.
1 Like
I think he’s referring to resveratrol, and it seems that chemically its quite close to Pterostilbene. See: Resveratrol and pterostilbene: A comparative overview of their chemistry, biosynthesis
I think the general criticism of Pterostilbene, and most supplements in general, are that you can find dozens of research papers with small sample sizes that purport health benefits, but very, very few extend lifespan in mammals in larger well-controlled studies like the NIA ITP program. While people’s biology may differ, so people may get healthspan benefits from a given compound, more broadly you have to wonder how big a healthspan benefit there is that people can get from a given compound if there is no lifespan improvement. Ultimately, if healthspan is truly being improved, then lifespan should follow… and that is what Richard Miller of the ITP program is saying.
It seems the biggest argument “for” some of these compounds would be if they either significantly prevent or delay some specific diseases (e.g. perhaps something like macular degeneration, etc), or brain/cognitive decline - which, conceivably could happen without greatly increasing lifespan. I would classify these as “quality of life” types of supplements, which obviously would be valuable, but its just so hard to parse out the actual benefit you might expect, and to parse out the risk of negative interactions with all the other drugs/foods/supplements you are taking.
3 Likes
Anecdotal obviously but mine has gone down dramatically since on Rapa (from around 90 to 30).
1 Like
Desertshores,
You were the one that brought up this paper:
https://onlinelibrary.wiley.com/doi/abs/10.1111/eci.13194
It says higher cholesterol is as good as a statin for all cause death. Of course these were CAD patients who were in trouble to start with, so maybe doesn’t apply. Still, they’re saying cholesterol is good. It looks to me like all treatments were equal except the guy with low cholesterol and not on a statin. He was in trouble. Possibly sick and the problem lowered his cholesterol.
Having said that Rapa increased my lipids and I backed off the dosage to 6/2weeks and everything went back to normal. I’ve decided to call life extension and try to get mine checked. I want to see what’s going on. I’ll check after 12 hours or so then in a week.
2 Likes
Nice to know the dosage that took you back to normal. I am off of rapamycin for 6 months or so while I give meclizine a trial. One of the things I find odd is that lipids are not one of the markers on the Levine phenotypic age calculator that many of us are using. My CRP also increased while I was taking rapamycin at higher doses. The Levine spreadsheet is used by Michael Lustgarten, Ph.D. and he is someone I trust.
3 Likes