As a physician, It’s time that i put this myth to bed, As it has become too widespread and I haven’t seen anyone correcting it. The best case scenario is people wasting their money, Worst case is subjecting their bodies to the side and long-term effects of drugs that do not actually do what they think they do.
SGLT inhibitors (Canaglifozin, Dapagliflozin…etc) don’t affect post-prandial (Post meal) spike of glucose in healthy people. At all. Tada! (Healthy meaning their maximal glucose level doesn’t go beyond 150mg/dl after a heavy carb meal)
If you’re taking them because you want to replicate the anti-aging effect seen in the ITP trials, Then I have bad news for you. Unfortunately, this glaring misconception is the result of abstract and skim reading the scientific papers without a deep and thorough understanding.
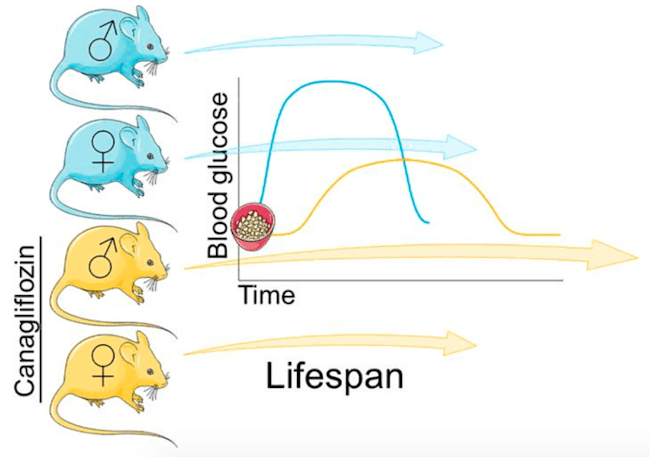
First of all it’s important to understand why the ITP actually chose ‘Canaglifozin’.
After the promising results of Acarbose, They wanted to test the hypothesis that the reduction in glucose spike after meals that is responsible for the increased median and maximal lifespan of the mice. So they choose the SGLTI ‘Canagliflozin’. Now Cana is unique compared to the others in it’s class. While they all inhibitit SGLT2 receptiors in the kidney and help excerte glucose. Cana is the only one that also inhibits SGLT1 receptors found in the intestines. So to mimick acarbose they decided to always mix cana with the food.
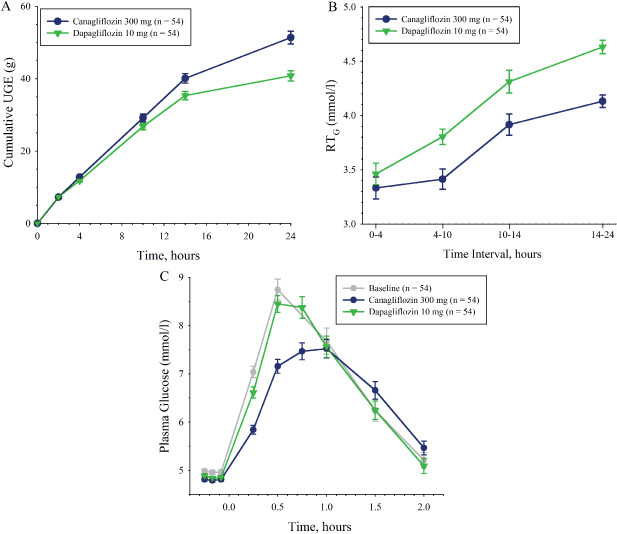
Yet that’s not how Canagliflozin is consumed or works in humans. SGLT2 inhibitors like dapagliflozin or empagliflozin have zero effect on SGLT1 receptors in the gut, Meaning they have no effect on postprandial glucose in healthy people (Assuming the peak doesn’t go over 160mg/dl. those with IGT or DM are another story). Canagliflozin also has no effect, Unless it is consumed just before the meal, And it’ll work for that meal only with no effect on subsequent meals, And you’ll need to use the maximal dose (300mg) to achieve any noticeable effect and it’ll still be weaker than a dose of acarbose.
So the prevailing notion that if someone doesn’t like the gases or discomfort after acarbose and they can switch to an SGLTI because it also supposedly prevents the glucose spike and extended healthspan in ITP, Is not only misguided But also categorically wrong.
It’s true that SGLT inhibitors have been shown in the literature in humans, To decrease damage to the heart and kidney, Improve HbA1c…etc (Cardiac protective effects are thought to be independent of any glucose effect) However, this does not necessarily mean this will definitively translate to anti-aging effects in healthy humans. I’d love to see an ITP study that uses Dapagliflozin in mice to see any healthspan effect and if there is a glucose spike-independent anti-aging effect of these drugs. However, until that happens, SGLTI should never be seen as a substitute for Acarbose. If someone wants to take them together then that’s another story.
Although keep in mind that SGLTI comes with rare but potentially extremely serious side effects. Which will be relevant if you’re taking them for many years, If not decades.
Of course, SGLTI are amazing drugs with certain established clinical entities with massive literature to back up their benefits, Such as:
1- established cardiovascular disease or High risk of CVD
2- Heart failure or high risk for heart failure
3- High risk of stroke
3- Diabetes, Or impaired glucose tolerance
…etc
I even predict it’ll be beneficial to those taking rapamycin and have a glucose spike larger than 160mg/dl 45-60 minutes after meals, Which Rapamycin is known to induce. Assuming they absolutely cannot tolerate or are not willing to tolerate acarbose. As the latter will always be the first choice and much more effective.
TLDR: Stick to Acarbose.