I think @A_User brings up a good point tangentially…
I think the key issue you’re missing is “measuring / testing” aspect. You can inexpensively get blood tests (in many parts of the USA) to track your lipids / APOB, blood sugar levels and responses (Insulin, HOMA-IR, A1C, etc.). Blood Testing Cost Comparison
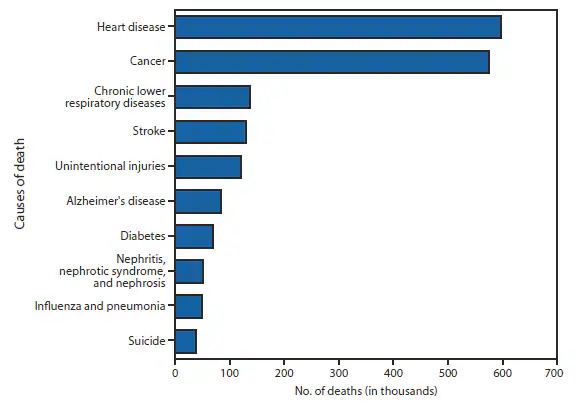
The key issues at a young age are avoiding trending physiologically towards any of the major killers… so you want to avoid things that contribute to the leading causes of disease. So - top on the list is heart disease, so you want to track your lipid levels to make sure you’re not building up plaque at an early age as many people do. Statins may be necessary if testing suggests that…
Metabolic disorders are key contributors to hear disease and cancer too… thus the need to track your blood sugar, A1C levels, etc.
We see plaque regression anywhere from 60-80mg/dL in the studies. Lowering that further just enables further regression, but I haven’t seen evidence yet that plaque can continue to grow at those levels.
It appears that even small differences in other risk factors are the cause for this progression even at levels below 60mg/dL. Rather than paying for expensive PCSK9i, lowering blood glucose and blood pressure levels is more promising.
It would be really nice to see results by LDL-C level stratified by Lp(a) level. I.e. three panels with one panel per Lp(a) tertile, age on X-axis, % disease free on Y-axis, and curve for each LDL-C level. If you are lucky enough to have low Lp(a), you probably do not need to be as aggressive in lowering LDL-C, but I have never seen evidence that shows the risk based on both. (That does not mean it does not exist.)
No one has mentioned this but why are you taking Dutasteride at such a young age? Are you experiencing hair thinning? If not, why not wait until you do (if ever)? I’ve never heard of Dutasteride or Finasteride helping skin.
I was able to lower my total cholesterol from 239 to 154 primarily by supplementing with citrus bergamot and flaxseed. I think citrus bergamot is an easy addition with minimal side effects for most people (just take it in the morning to avoid heart burn). I’m not against statins or other cholesterol-lowering medications, but I’d personally rather try lower side effect options first.
Yes I started to see mild hair loss, I also have very oily skin and as dut also inhibits type 1 it helps massively with acne. DHT is also somewhat responsible for a breakdown in elastin in the skin so it will help with overall skin aging.
Mainly though I see no reason not to considering I have 0 side effects and it stops hair loss and acne for me.
In young ppl, caloric restriction is arguably more important than exercise [1]. Exercise by itself encourages anabolic hyptertrophy and activation of the mTor/IGF-1 axis, which constitutes the opposite mechanism underlying the longevity benefits of validated interventions like rapamycin. In addition, exercise in general increases oxidative stress and after a particular point it has further negative effects (i.e overtraining). 7h/week is already far above the minimum recommended 2.5h/week.
Of course, exercise will always be incomparably better than being sedentary. Also, consider the option of combining caloric and protein restriction, with moderate exercise; it’s harder, but it’s the regimen I’m personally following. Regardless whether you choose to do a form of dietary restriction (but moreso if you do!), I would suggest you begin tracking your dietary micronutrients meticulously.
Probably minimal… See Joan mannick’s comments in the first video at this link. She says they have seen minimal penetration of the blood brain barrier with rapamycin…