We actually do NOT know that blunting spikes and reducing glucose AUC does not reduce incident CVD risk. I believe you are referencing only the ITP. It dosen’t do CAC scans on euthanized mice, only pathological post mortems of lesions.
But glucose is highly implicated in CVD due to it’s damage to the endothelial glycolyax and inflammation. Whether it’s spikes and/or AUC, it’s seems to be a causative progressing agent, in humans and wild type mice. A correlation between diabetes, metabolic syndrome and the #1 cause of death, CVD?
The Diabetes Mellitus–Atherosclerosis Connection: The Role of Lipid and Glucose Metabolism and Chronic Inflammation
“We also discuss the established pathophysiological features that link atherosclerosis and diabetes mellitus, such as oxidative stress, altered protein kinase signaling, and the role of certain miRNA and epigenetic modifications.”
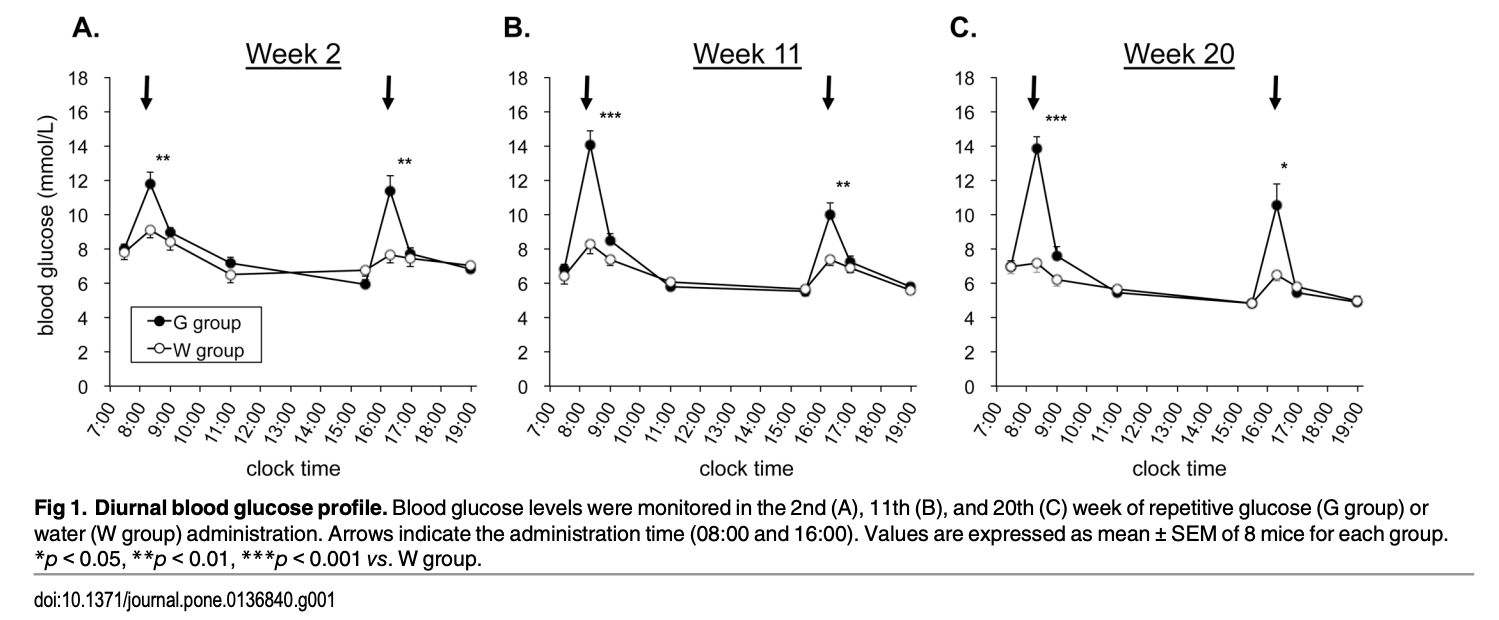
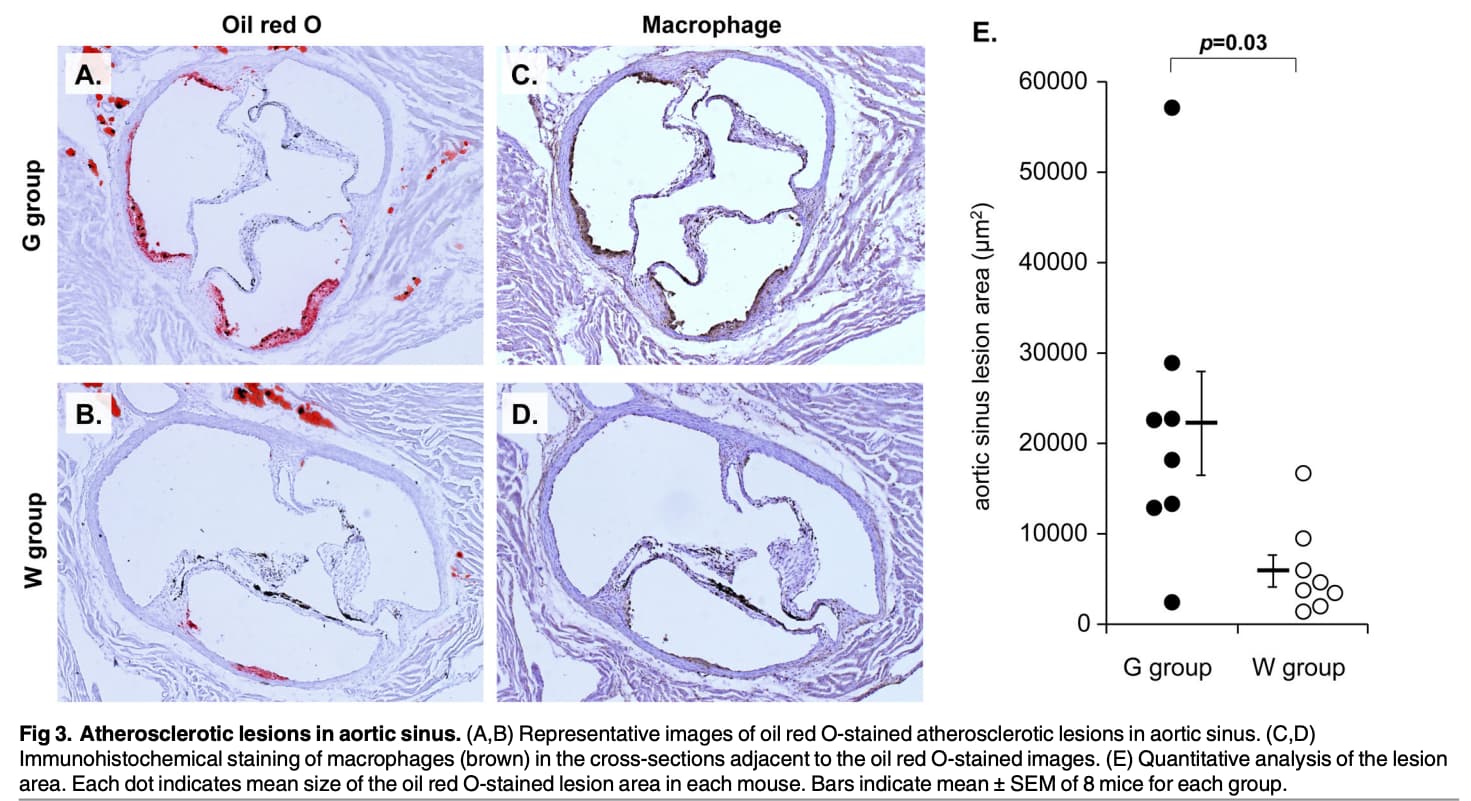
Repetitive Glucose Spikes Accelerate Atherosclerotic Lesion Formation in C57BL/6 Mice
A study using wild type mice, similar to ITP:
Conclusions
“These results indicate that glucose spikes can accelerate atherosclerotic lesion formation, with little influence on other metabolic disorders. Repetitive glucose administration in wild-type mice may serve as a simple and useful approach to better understanding the causal role of glycemic spikes in the development of atherosclerosis.”
I take strong exception to their concluding remark “These results indicate that glucose spikes can accelerate atherosclerotic lesion formation, with little influence on other metabolic disorders”.
The ITP mice on glucose lowering meds live longer by delaying cancer…not an mTOR pathway, so I would suggest a pro-carcinogenic pathway is also implicated (cancer is 2nd leading cause of death in the US).
Canagliflozin extends life span in genetically heterogeneous male but not female mice
https://insight.jci.org/articles/view/140019
“Since most UM-HET3 mice die of neoplastic disease, the effects of Cana on cancer may be particularly relevant for its ability to extend mouse life span. In preclinical studies, Cana administered at high doses to rats increased the frequency of adrenal and renal tubular tumors, and induced Leydig cell hyperplasia and adenomas at all doses in male mice”
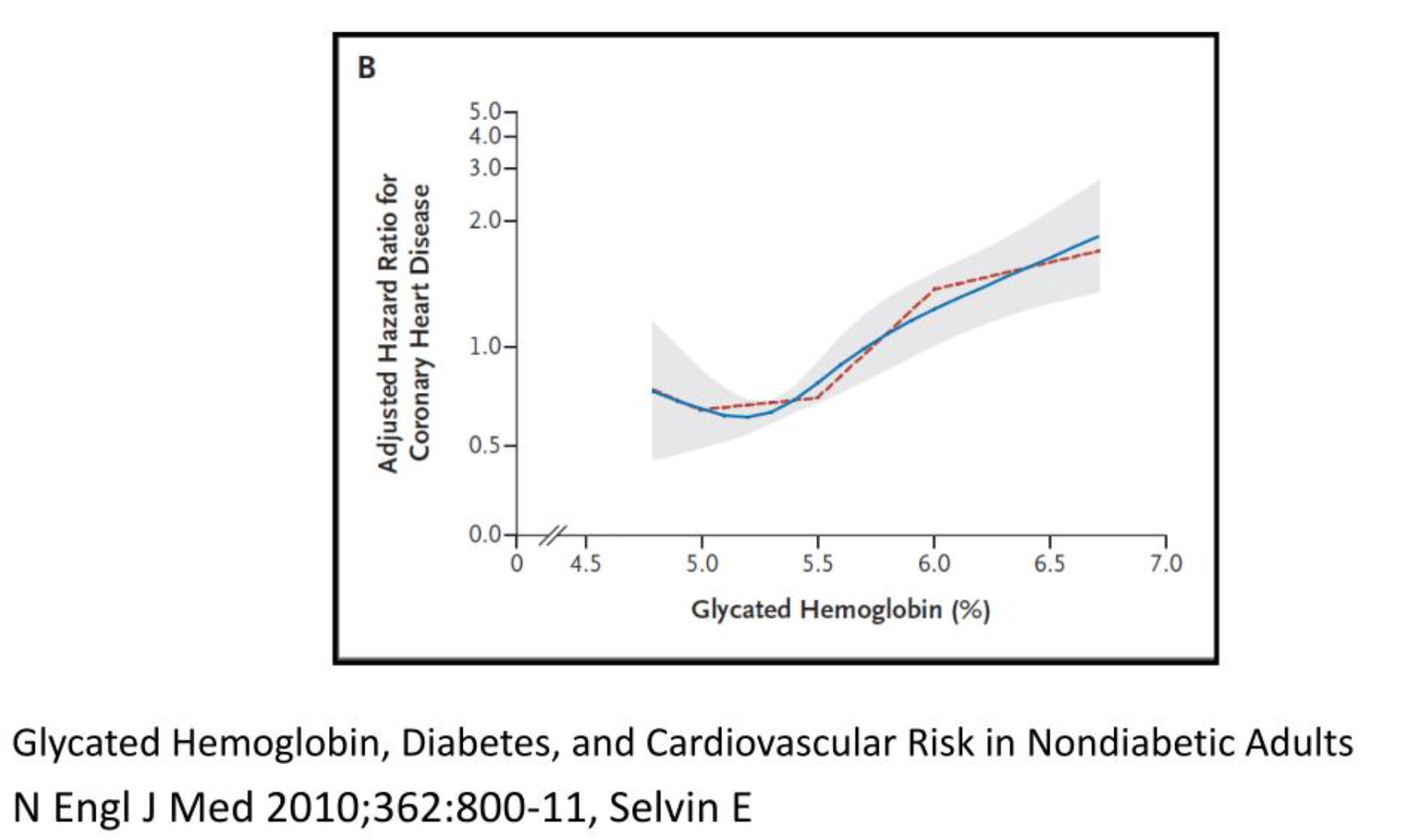
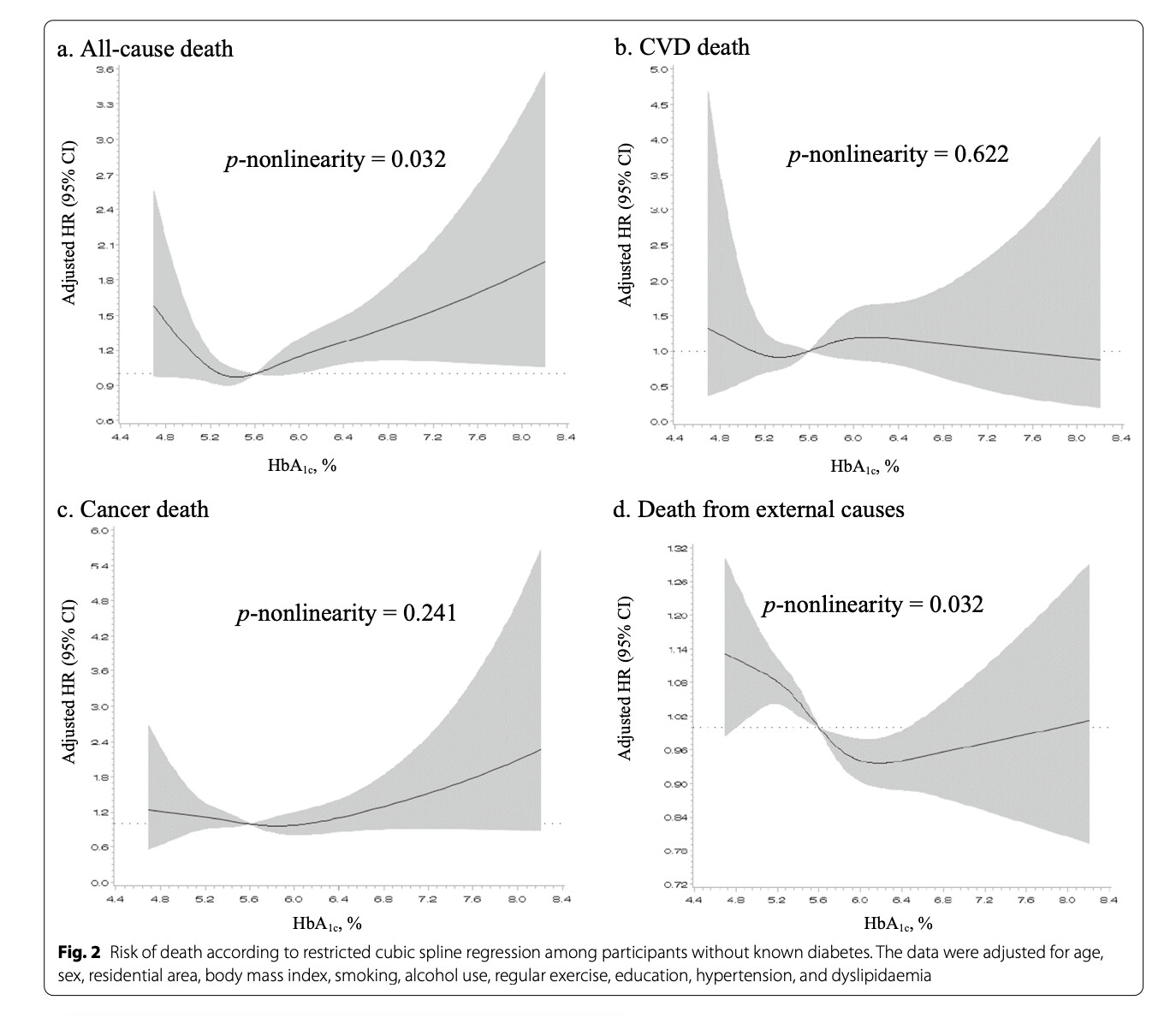
Association between haemoglobin A1c and all-cause and cause-specifc mortality in middle-aged and older Koreans: a prospective cohort study (2022, 16 yr followup, n=9294)
“Conclusions: We found U-shaped associations between HbA1c levels at baseline and over time and all-cause mortality in middle-aged and older Koreans. Additionally, the risk of cancer mortality increased both in low and high HbA1c groups, but CVD mortality increased only in high HbA1c group. In particular, people with liver diseases and low HbA1c levels had a high risk of all-cause mortality. Therefore, more careful management of these groups is suggested to identify any deteriorating health conditions.” (love the little reverse confounder comment on the low end curve…these people are sick, so unless you dabble into preemptive hypoglycemic risks, the lower the better)
Look at the slope of the A1C/cancer graph.
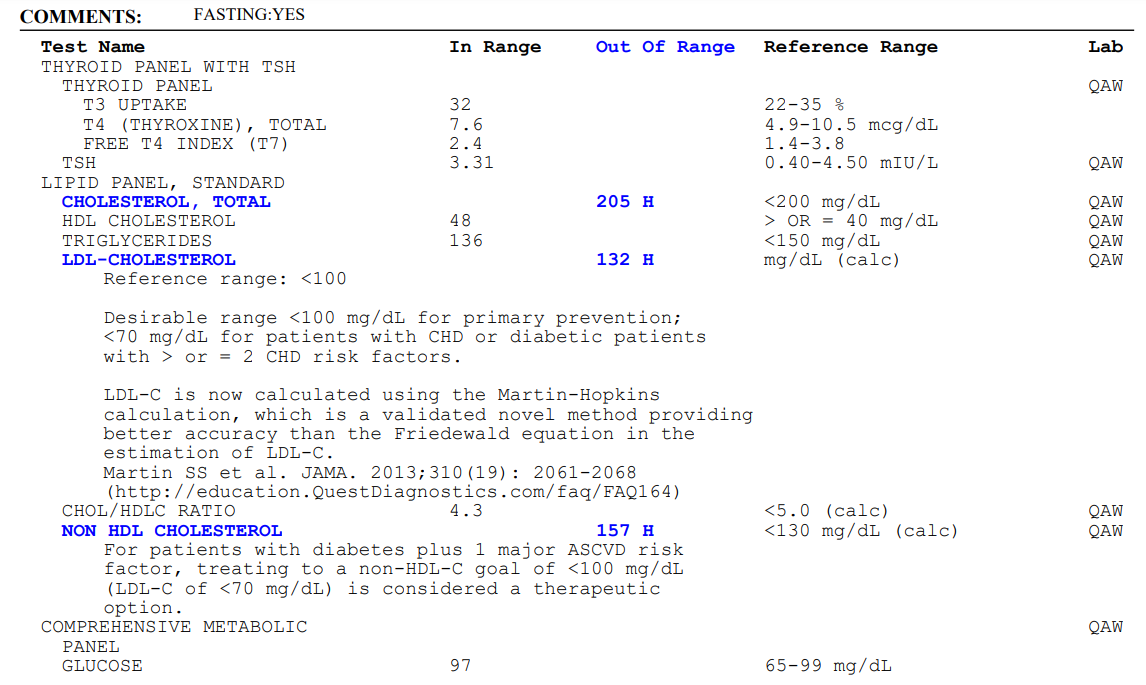
Crushing glucose (keto/OMAD) is a central part of my biohacking stack. My A1c has been 5.0 for years, and my diet precludes spikes. Donating 450mL of blood every 8 weeks also dumps a lot of old gylcated and misfolded proteome junk.