In mice! Complete wishful thinking it fully translates to humans living beyond 100+
Implicitly yes, but yet…I’ve never seen a paper looking at lipids and CVD on mice taking Rapamycin. Mice on rapamcyin don’t die of classic CVD, only cancer. (90%+)
So let me see, we are to pick and chose a la carte which pathological mechanisms we “like” (eg mTOR inhibition), and dismiss others (eg lipids, neutropenia, thrombocytopenia) with respect to human translation of Rapamycin, even though no data exists showing mice with elevated lipids on Rapamycin?
Now this I agree is perhaps THE best translation data pool we can learn from. Not perfect, but would be great if someone would collate and try to statistically extract some semblance of efficacy signals. You would think there would be a number of patients tracking lipids and a subset perhaps CIMT/CAC or any CVD event.
I can’t believe that this isn’t being done. Yeah, I get it, not an RCT but I don’t care. All of those anecdotes would give us a ton of information, and in humans yet.
Not just lipids either, but also skin infections, CBC results, etc. Some of this information may be revealed in Matt’s study, but why not both.
We don’t need to just concentrate on adverse reactions, we can also gather data on positive health effects as well.
I’m not suggesting that Alan would have to undertake this project but someone should be able to do it.
So Alan G tells me that he sees a transient elevation of LDL in his elderly population “ but no CAD”. By that I assume he means no cardiac events. He feels that the anti inflammatory mechanism of rapamycin is protective.
Thanks for following up. What does he mean when he says transient? Short term, then reverts back to pre intervention?
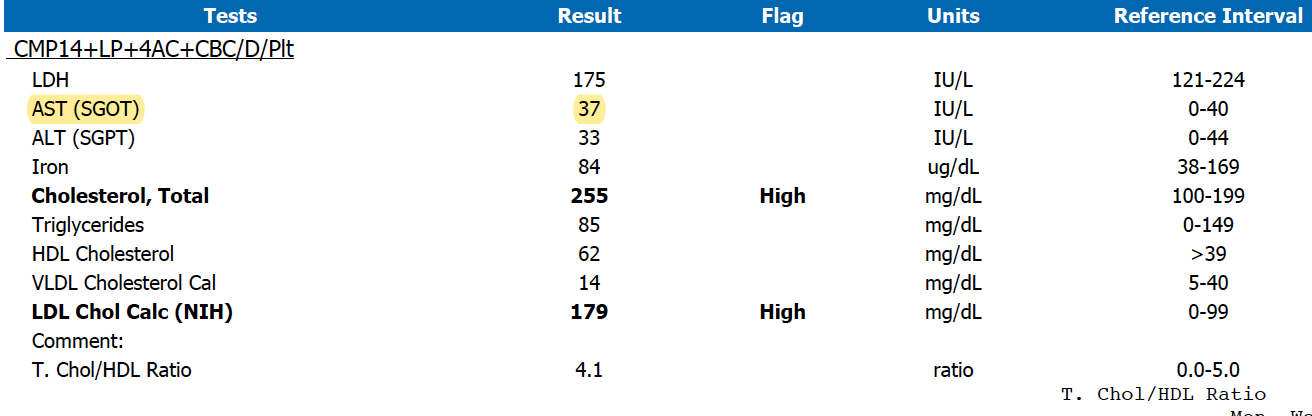
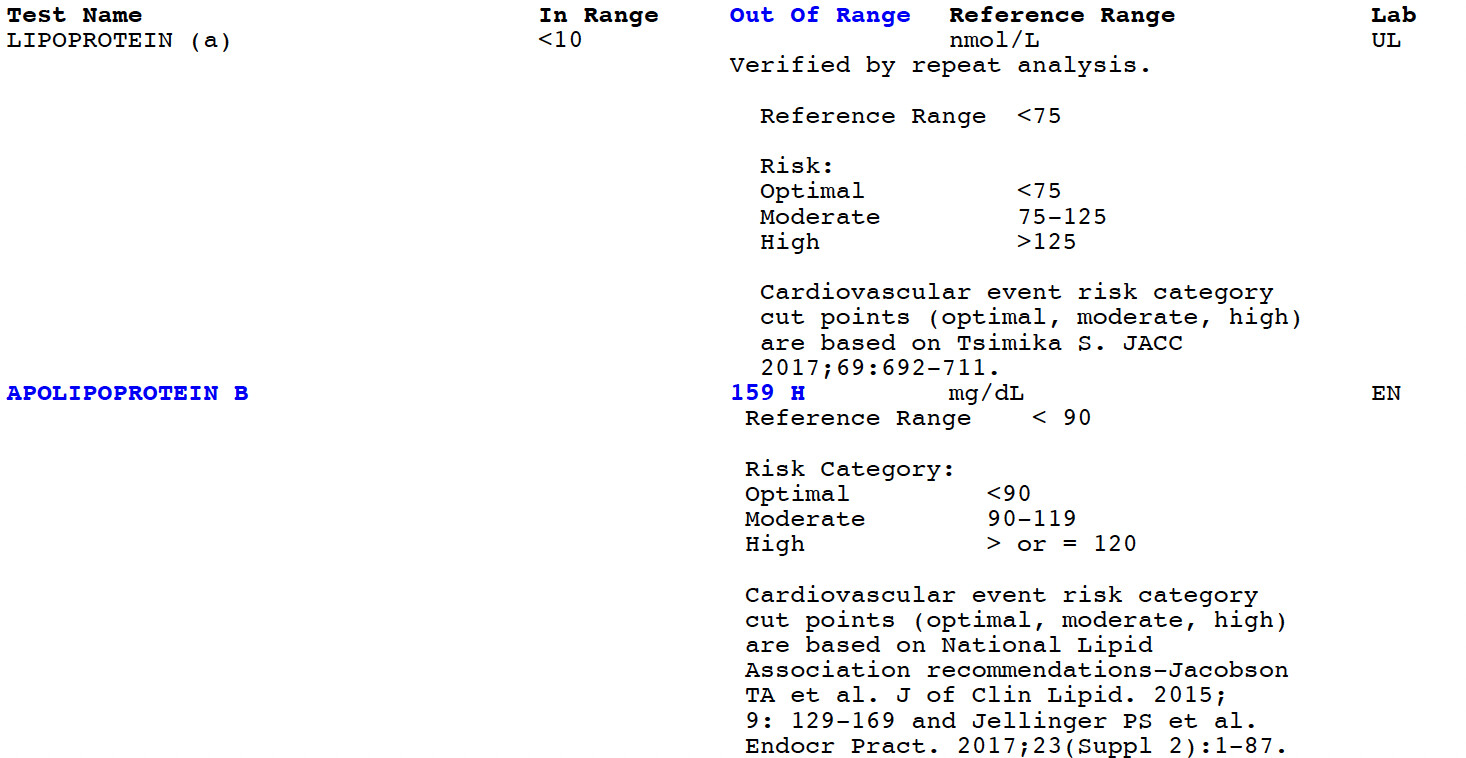
But we already know LDL is not the culprit, it’s the TG/HDL and oxSDL? What does he report on this metric? LDL is not, in and of itself, a meaningful report (you’ve intimated such several posts)…we already know rapamycin raises LDL.
Now the no CAD events, well, that is the more important signal outcome, which is at least a good longitudinal data point so far. No reason to jump off the train!
Not sure what he means by transient. To me that would be maybe 6 months or so and then revert it back to pre rapa levels. He may have a different definition.
Yeah, I asked about lipids and he centered on LDL.
Cardiovascular events are certainly the bottom line. Atherosclerosis is very common and so are plaque ruptures which heal themselves with fibrotic caps. The fact that out of a thousand elderly people he’s not seeing events is reassuring, though not definitive.
When discussing inflammation he focused on gingivitis which he seems to believe is a good proxy for CAD. There’s some evidence for this, but it’s only an association, and many people have gingivitis without CVD and many people with CVD don’t have gingivitis.
Noted, but as you say, not definitive. We’d have to go deep in the weeds of his patient pool and have sufficient population power to infer anything more. At least it does not seem to be quickly flipping say the at risk subset to events? You’d think Dr G would see that within his 1000 total patients…he’d have at least some high risk CVD patients.
Yes - its a problem I’m working on addressing. I’ve almost always been on a low fat diet, mostly vegetarian (including avacados), fish and limited carbs, almost all “Whole Foods”.
My Total and LDL numbers have gone up about 50 points since starting rapamycin.
The Peter Attia Podcast on Cardio Risk seems to counter this perspective (see below) a little. A CAC score of zero seems to be not a bad thing, especially if you’re over 60, but low numbers don’t seem to be a cause for a completely relaxed perspective.
Calcium score (CAC)
This is done by doing a very quick CT scan of the heart without any intravenous contrast
It looks at the amount of calcification in the coronary arteries
This is very late in the disease process
Once you have calcium formation around coronary arteries you’re at the 2nd to last stage of atherosclerosis
It’s a late stage of healing
Calcium formation is a very advanced finding of disease but it doesn’t tell you much about what’s happening at the point of calcification
Just yesterday, Peter got a patient’s calcium score back and it was not a very high number, but it wasn’t 0
That’s already a big red flag
It was at one part of their heart, but that doesn’t really tell much
The fact that they have a score of, say 15 at one part of their left anterior descending really means nothing about what’s happening there
But that becomes a real global alarm given that person’s age (early 40s)
Further, if they have a calcified point right there, they undoubtedly have atherosclerosis elsewhere
The CT angiogram (CTA) is a much better test
But it comes at a higher cost and it comes with more radiation
At really good places, it should be in the ballpark of 2 millisieverts of radiation
That’s a very small dose of radiation, about 4% of your annual allotted radiation, according to the NRC
Tons of evidence that a CAC score of zero puts you at very low risk of a CV event. Highly prognostic, easy to do, and inexpensive. Even a score of 1-100 would be considered low risk, but of course it’s more concerning in a 40 year old than in someone over 65.
Thank you. That is a very good article on taurine. I didn’t realize what extensive benefits it had. I did not for example know that it lowers cholesterol.
After reading the article taurine goes onto my top ten supplement list.
I was taking it as a sleep extension aid. Then I stopped when I started getting a good night’s sleep after taking rapamycin for months.
Good exchange if you expand to the twitter feed. Agindoc1 at least concedes, intervening with lipid lowering meds is “individual specific”, looking at complete profile, as @rivasp12 has repeatedly advocated. The participants do not seem to accept that rapamycin and lipids rise is benevolent. Dr B comes across as too whimsical dismissing lipids, perhaps a result of confirmation bias to his beloved rapamycin miracle drug.
Certainly, ANYONE messing with rapamycin needs regular blood panels, and a complete evaluation by PCP and/or cardiologist if lipids dsyregulated. Get a CAC folks! There is no debate here.