I saw this posted on Twitter yesterday and it got me curious as to whether anyone else here is testing the highest range of dosing for rapamycin, and what their experiences have been.
Obviously, anyone doing this should be very careful, and ideally do blood testing to make sure all the regular blood markers are suggesting good health.
From many of the experts - Matt Kaeberlein, AgingDoc1 (on Twitter), and others, I’ve seen increasing warnings about blindly testing higher doses of rapamycin.
Be careful people, we don’t want to see any seriously bad outcomes or adverse events in our community. The risk, as some researchers highlight, is that these higher doses (if done at a frequency that results in higher mTORC2 inhibition) could result in the type of compromised immune system that puts people at risk of serious infections.
Charles has been very active sharing his rapamycin journey.
My response:
Charles is sort of the poster child of rapamycin use on Twitter:
No, a blood panel after a few weeks would definitely be in order, including a test for rapamycin trough at the end of the dosing period. At that high dose, observing side effects isn’t enough.
Yes, I have done 4 doses of 20 mg. with grapefruit juice and 1, 20 mg dose with grapefruit juice plus fat. These were spaced 14 & 15 days apart. I am using the same brand, Biocon/Rapacan 1mg tablets that are in Charles Nelson’s picture.
The first 3 times I dosed with 20 mg I felt a good somewhat elated mood elevation 2-4 days after the dose. Maybe placebo effect, I don’t know. On the day after a dose and for 3 - 5 days I also had a lot of flatulence and loose stools and mild diarrhea. On the fifth dose taken with grapefruit juice and fat, I had real diarrhea and a lot of flatulence and had to take some anti-diarrhea medication. I also am no longer getting the mood elevation I was expecting.
So, I am going to dial back to 10 mg with grapefruit juice every 14 days.
This is great real world n=1 human data. If you would ever come to do some Sirolimus trough/spike blood testing (and other blood biomarkers connected to Rapamycin dysregulation/improvement), please do share.
I take 6mg with fresh squeezed (8oz a few hours before and 8oz with administration of medication). From my understanding of the literature, this should equate to approx a 20 to 25 mg dose of rapa. I consider myself a bit of a risk taker and “envelope pusher” but I really can’t wrap my head around people taking doses equivalent to up to 80 mgs per dose, especially when we do know that suppressing Tor2 is something we know we want to avoid at all costs and there is zero data or practices by any experts (IE: Green or Blagosklonny) suggesting that these high doses are either safe, or beneficial.
After listening to the recent AMA I backed my dose off to 8mg/wk. FWIW Dr Green strongly warned against using grapefruit, “you want a quick peak and for it to clear quickly”.
IMO, if you want to try a higher dose, you should pay the $$$ and just take more Rapa. There are too many unknowns with GF…
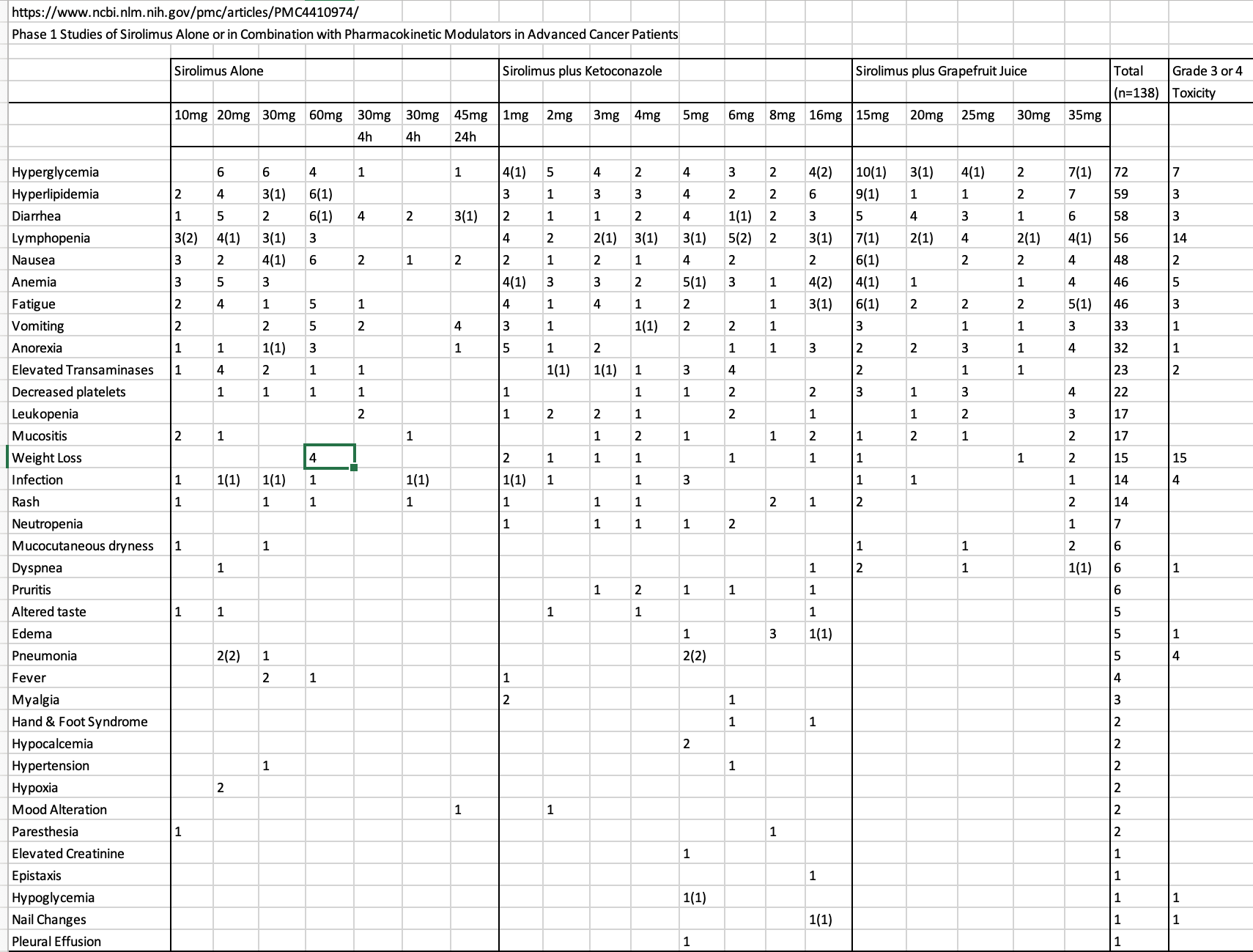
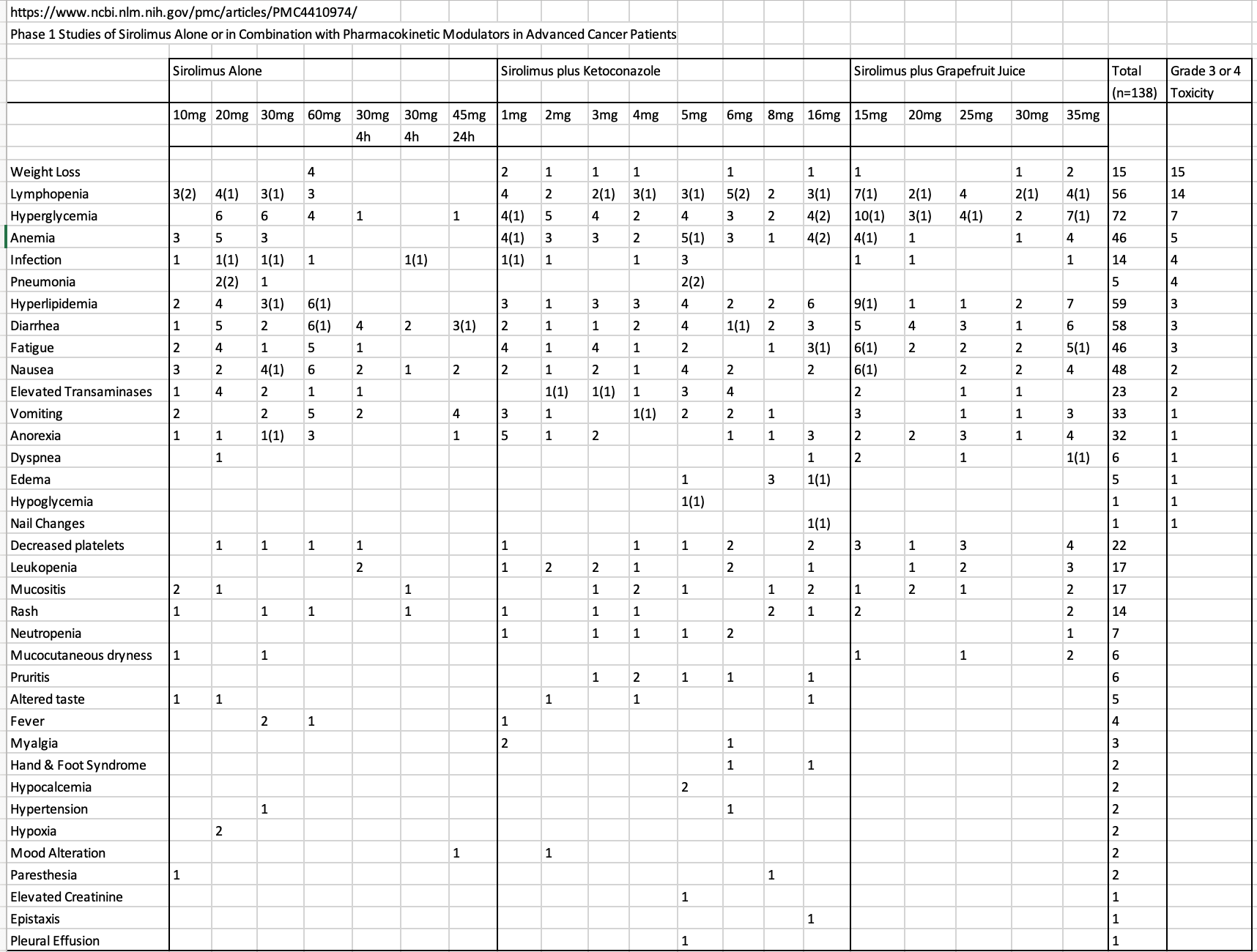
I’ve taken the adverse summary data of the Sirolimus/Cancer/GFJ/Ketoconazole study and filtered to rank by # of adverse advents and by # of dose 3/4 toxicities.
The one marker that I’d be perhaps most concerned with is Lymphopenia. Exceeded DLT for 14 of the 138 participants (relatively small % but not insignificant, and who in the cohort by age/health status reached this threshold?). Certainly, most all adverse events would reverse once you ceased dosing, but lymphocytes are 24/7 important for the immune system (covid!), and could increase the risk of triggering a major non reversible event? Elevated glucose and lipids (highest frequency adverse events), once observed, could be reversed/managed, and nevertheless, would take time to impact health.
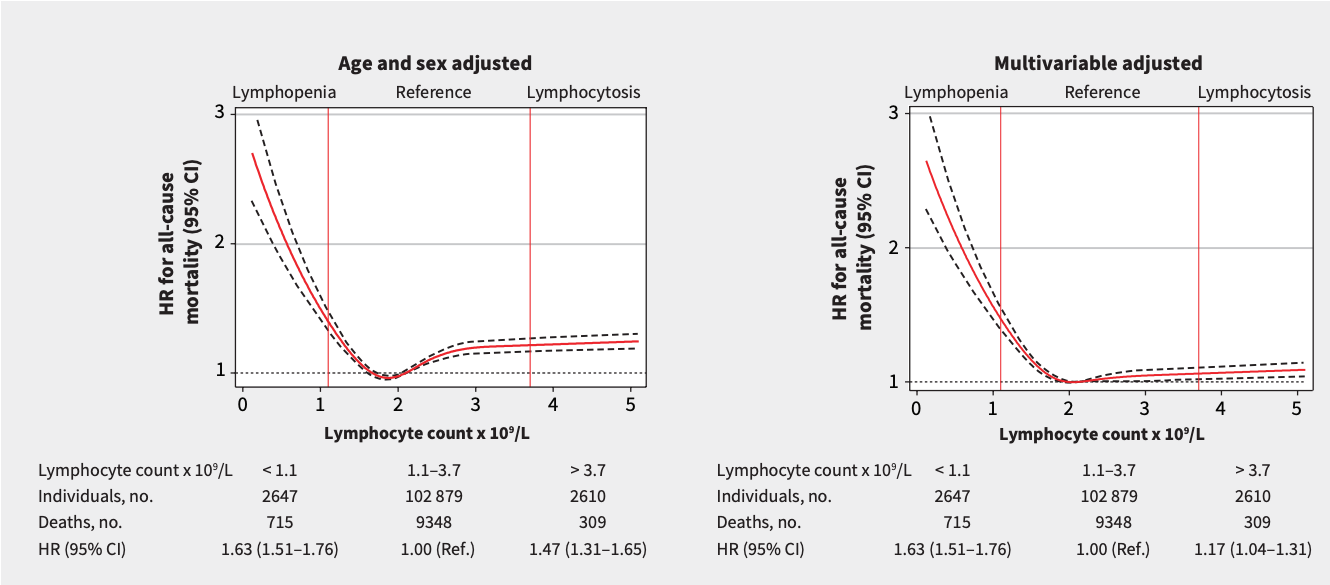
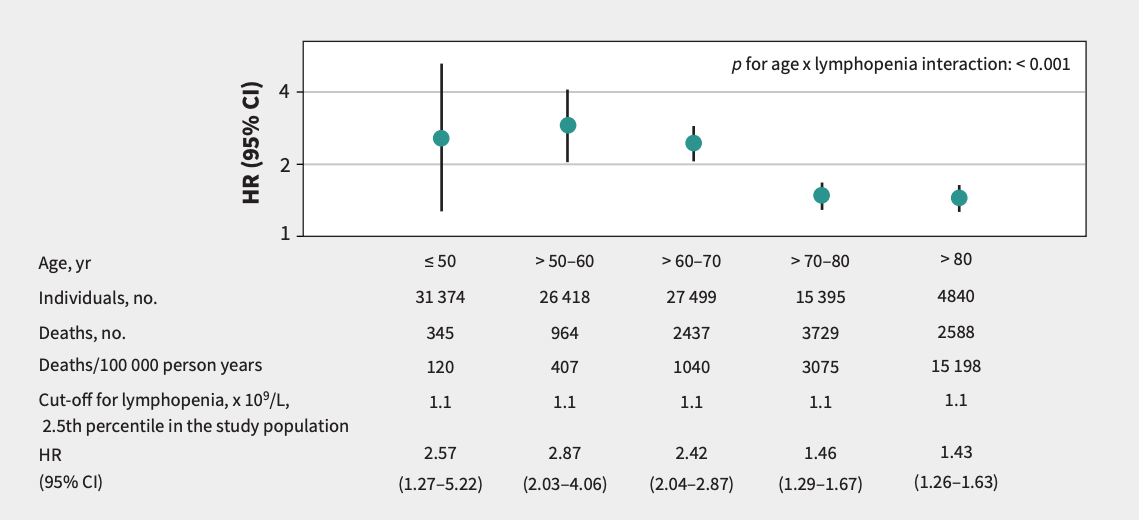
Incidental Lymphopenia and mortality: a prospective cohort study
“The cohort included 108,135 participants with a median age of 68 years. During a median follow-up of 9 years, 10,372 participants died. We found that participants with Lymphopenia (lymphocyte count < 1.1 × 109/L) compared with those with a lymphocyte count in the reference range (1.1–3.7 × 109/L) had higher mortality with multivariable adjusted hazard ratios (HRs) of 1.63 for all causes, 1.67 for non-hematologic cancers, 2.79 for hematologic cancers, 1.88 (95% CI 1.61–2.20) for cardiovascular diseases, 1.88 for respiratory diseases, 1.86 for infectious diseases, and 1.50
for other causes. For all-cause mortality, the highest absolute 2-year risks of death were observed in women (61%) and men (75%) who smoked and were aged 80 years or older with lymphocyte counts less than 0.5 × 109 /L. Participants with a lymphocyte count higher than the reference category had increased mortality, adjusted HR 1.17”
1.63 HR for ALL causes. (This is an association study, does not prove causality)
So here we are trying to reduce/delay cancer incidence with Rapamycin, but yet low lymphocytes is “associated with” significantly increased all cause mortality risk. A pendulum of balancing risks in humans, not captured in the sterile/only die of cancer mice world.
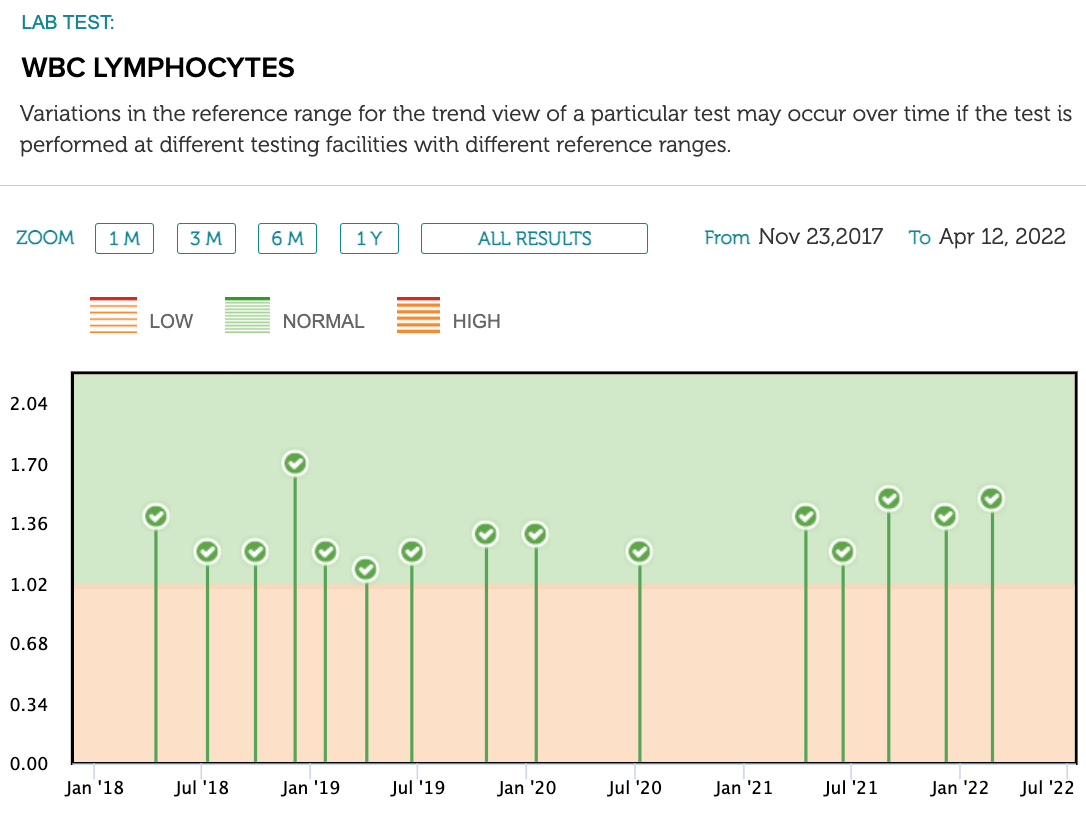
This is my Lymphocytes trending graph. Local lab reference range 1-2.9. I started Rapamycin Jan '21, but starting to ramp up experimenting. Every CBC I’ve done, all markers have always been in the normal range, although I do trend in the lower half of normal. My overall average is 1.23. 57 yo male, daily exercise, very lean/fit, excellent diet. Haven’t had a cold in forever, or caught COVID (triple vaxxed). No history of cancer, CVD in the family, only neurodegenerative.
The study posted by MAC. This looks like a nice study compare with and w/o GFJ. But it raises questions to me.
The data show that sirolimus alone at 20 mg had more side effects overall than when admin with grapefruit juice at 20 mg. GFJ is supposed to increase intake by 350%, thus the GFJ dose was equal to 70 mg without the juice.
It is unfortunate that the study did not run equal doses of Sirolimus alone and Sirolimus with GFJ, so the nearest straight comparison is at 20 mg, which for us is way high. And also be useful to start the trail at a bit lower dose…say 5 mg with and without.
It seems that one would want to determine how much the low doses of sirolimus are affected by GFJ as they do with keto and even there the sirolimus and keto added doses are not comparable at lower doses.
Yep…other anomalies here too. Big disconnect in what we assume on this. Given all the other work on GFJ and drugs it seems that the boost is real. How much is the issue and timing, etc. I started using it to boost an 8 mg weekly dose with zero side effects (which now seems low compared to other reporting).
I take 8 oz fresh squeezed with pulp 2 hours before. Still no side effects. going to park here.
I figure if at max it increases 3.5 x then that’s a lot (equal to 28 mg) but also build in the fact that it might really be 2x for lots of reasons reasons…so that 16 OK too. at least for now.
Final note…the effect of GFJ varies widely by drug. I think for the 3.5x we are using some other drug as the base (one of the statins I think). Anybody have this multiplier specifically for Rapa?
“I will add that I have serious reservations about the use of Sirolimus for general prophylactic purposes, since the drug can cause both serious interstitial lung disease, as well as anemia due to impaired iron utilization”.
Has Dr Green given this adverse effect warning?
Also, on elevated glucose and lipids…“that’s how you know it’s working”. I’ve not even reached this state yet, so I have runway.
He provided no references to the lung disease assertion/context other than I assume his clinical practice. I donate blood every 8 weeks to expressly dump iron, whilst taking Rapamycin, and have zero side effects to date. I would be classified as iron deficient without anemia (self-induced), although my hemoglobin is normal. (But I’m also homozygous H63D…so maybe I have deep cellular iron storage reserves not captured in blood tests)
Regarding Interstitial Lung Disease (ILD) and mTOR inhibitors:
“In February 2017, after completion of chemotherapy she was started on Sirolimus 2mg daily. The level was maintained at 5–10 ng/ml. In July 2017, the patient presented with dry cough, fever and dyspnea on exertion for six weeks. In November 2017, sirolimus was discontinued and she was switched to everolimus at 0.75 mg twice daily. The level was maintained at 4–8 ng/ml. Within one week the patient experienced improvement in her symptoms and she was back to her baseline level of activity after two months”
Here’s another:
“The literature review identified 57 publications on ILD in solid organ TxR receiving everolimus or sirolimus. ILD presented months or years after mTORi initiation and symptoms were nonspecific and insidious. The event was more frequent in patients with a late switch to mTORi. In most cases, ILD was reversed after prompt mTORi discontinuation. ILD induced by mTORi is an uncommon and potentially fatal event warranting early recognition and drug discontinuation. Out of the 1,473 de novo TxR receiving everolimus in Phase III trials, everolimus-related ILD was confirmed in six cases (one kidney, four heart, and one liver TxR) representing an incidence of 0.4%”
ILD wasn’t even a noted adverse event in the Sirolimus/GFJ trial, only anemia (DLT in only 5 of 138 persons)? It appears to be something associated with chronic daily Sirolimus administration and some significant length of time (malignant cancer/transplant setting), you can feel it coming on, and thus, backing off dosing, reversible.
I am not perturbed in an intermittent dose model. As long as you closely monitor blood markers and side effects, whenever it reaches tolerance levels, you just back off. The effects of Rapamycin are reversible, hundreds of studies have shown this.
You’ve said “20mg, which for us is way high”, and “max increases 3.5X, then that’s a lot (equal to 28mg”. Define high and a lot?
Unless you do your own n=1 experiment, monitoring blood markers and side effects, you just don’t know your limit, whatever that target might be for YOU. We don’t even know what level of mTOR suppression in humans reaches high percentile to flatten the aging curve?The GFJ study gives some insight for cancer target (and it’s higher than what most of us take)…is this “the” target for longevity?
Genetic predisposition to CYP3A4 enzyme polymorphisms/expression, mTOR polymorphisms, GFJ type/dose, gastric processing, base levels of nutrient signalling, timing, etc will all have major impacts on your personal pharmacokinetics/response. Different cell lines/organs have varying degrees of mTOR suppression.
GFJ/drug interaction is highly specific. GFJ can have a HUGE impact on some statins.
“In a randomized cross-over study with two phases, 10 healthy volunteers ingested grapefruit juice 200 ml or water (control) for 3 days. On day 3, a single 40-mg dose of simvastatin was administered with grapefruit juice 200 ml or water. Plasma concentrations of simvastatin and simvastatin acid were determined up to 24 h. Grapefruit juice increased the area under the plasma concentration–time curves from 0 to 24 h [AUC(0–24)] of simvastatin 3.6-fold and that of simvastatin acid 3.3-fold (range 2.1–5.6-fold; respectively. The peak concentrations (Cmax) of simvastatin and simvastatin acid were increased 3.9-fold and 4.3-fold (range 2.7–7.9-fold;
by grapefruit juice.”
“This crossover study consisted of 5 study days, during which 10 healthy volunteers ingested 40
mg simvastatin with water (control), with “high-dose” grapefruit juice (200 mL double-strength grapefruit juice three times a day for 3 days), or 1, 3, and 7 days after ingestion of “high-dose” grapefruit juice. For safety reasons, the study was performed in three parts to allow simvastatin-free days between the study days. Serum concentrations of simvastatin and simvastatin acid were measured by liquid chromatography–tandem mass spectrometry up to 12 hours. When simvastatin was taken with grapefruit juice, the mean peak serum concentration (Cmax) and the mean area under the serum concentration-time curve [AUC(0-∞)] of simvastatin were increased 12.0-fold (P < .001) and 13.5-fold (P < .001), respectively, compared with control. When simvastatin was
administered 24 hours after ingestion of the last dose of grapefruit juice, the Cmax and AUC(0-∞) were increased 2.4-fold (P < .01) and 2.1-fold (P < .001), respectively, compared with control. When simvastatin was given 3 days after ingestion of grapefruit juice, the Cmax and AUC(0-∞) were increased 1.5- fold (P = .12) and 1.4-fold (P = .09), respectively, compared with control”
“In a randomized, four-phase crossover study, eight healthy subjects consumed either GFJ or water t.i.d. for 4 days in each trial. On each final day, a single dose of 4 mg pitavastatin or 20 mg atorvastatin was administered. GFJ increased the mean AUC 0-24 of atorvastatin acid by 83% (95% CI 23–144%)and that of pitavastatin acid by 13% (-3 to 29%).”
“We determined the validity of current medical advice to avoid grapefruit juice consumption while taking 3 widely used statins. A daily glass of grapefruit juice increases blood levels of simvastatin and lovastatin by about 260% if taken at the same time (about 90% if taken 12 hours apart), and atorvastatin by about 80% (whenever taken). Simvastatin 40 mg, lovastatin 40 mg, and atorvastatin 10 mg daily reduce low-density lipoprotein (LDL) cholesterol levels in a 60-year-old man with an LDL cholesterol of 4.8 mmol/L by 37%, reducing ischemic heart disease risk by 61%. When simvastatin or lovastatin are taken at the same time as grapefruit juice, the estimated reduction in LDL cholesterol is 48%, and in heart disease is 70%. If the juice is taken 12 hours before these statins, the reductions are, respectively, 43% and 66%, and for atorvastatin, 42% and 66%. The increased rhabdomyolysis risk from grapefruit juice consumption due to the increased effective statin dose is minimal compared with the greater effect in preventing heart disease. Grapefruit juice should not be contraindicated in people taking statins.”
Am I missing something? In the data tables shows the gfj portion with higher, not lower starting sirolimus levels than sirolimus alone. Would you not think if concerned about high levels with gfj the dose there would start at 5 mg or so…not 15 which is higher than the sirolimus alone low dose.
I did read lots on the lung disease side effects. Worrisome at first but reading the detail gets me over that.
As far as my comments on dosing and 20 mg weekly being “high” I base that on reports from users which is about the only thing to go on right now. Even with all of your testing you are not sure you are on the best dose for results. So I am hedging side effects against results…not the live to 110 years results but the health extension ones…aches, performance,etc. I have no big “obvious” problems to overcome so cannot measure on that. Green got into this with 6 mg and great results. That seems a good
starting point…until we have real trials…a long time away….this type of estimation is about all we have to go on. Blood tests every month are great but not necessary. You can drive yourself crazy doing all that and still not have it figured out.
My results so far. Eight weeks in. Got rid of a few nagging but not really debilitating aches and stiffness in shoulder. Maybe imagination. Some facial aging blemishes seem to have almost cleared. Have no noticed an increase in “fitness” as some report and nothing with weight…need to lose 15 lbs. This on 8 mg….last 2 weeks did with gfj. This is the 28 mg I refer to…8 plus 3.5 multiplier with the juice. So seems to be moving in the right direction. Will continue to ten weeks and the a break.
Great. Slow and steady. At minimum, unless you reach one or more side effects, you are probably not pushing mTOR down sufficiently. I am trending slowly and methodically to try and trigger some of these, whilst trying to tease out “improvements”. Blood markers, how I feel, and the study adverse table summary will serve as my guide.
I personally think you are getting much more than 350% increase taking 16 oz of GFJ. The GFJ protocol is as important as the dose of rapa when posting results. The more GFJ you take = the more bioavailability of Sirolimus. Most studies used 240 cc appx. 8 oz GFJ. I adjusted my personal protocol to 250 cc GFJ, 30 minutes before ingestion of SIrolimus and feel that I am getting 300-350%.
Have there been any studies on varying amounts of GFJ (or ketoconazole or the like) for inhibiting drug clearance? It stands to reason that more GFJ would give more inhibition, but probably only up to some maximum? 8oz? 16? 32?