This is something Dudley Lamming at U. Wisconsin has written a great deal about. This thread has some information, and Dudley has a number of papers that touch on the topic, which he provides links to in the thread I share below…
Hey Duncan… David Sabatini explains how continuous rapamycin will stop MTOR 1 from creating MTOR2.
In this podcast with Attia and Kaeberlein…he explains how it happens. Fascinating.
The Drive # 272 ‒ Rapamycin: potential longevity benefits, surge in popularity, unanswered questions, and more
Link: https://youtube.com/watch?v=O67pvKxio10&si=9mWMmDQpy3m-x12i Go to point 47:38 - of 3:01:28
From a Matt Kaeberlein, PhD private message in November Re: Rapamycin higher dose - "I honestly don’t know. I understand Misha’s (Mikhail Blagosklonny) rationale for pushing it as high as possible until you get to side effects. My concern there is that you might be getting to side effects and not know it right away or at all (silent pathology) until it’s too late to reverse the damage. I have no evidence for that, but it’s a concern I have.
I absolutely think it’s possible that 36mg could be net detrimental to health while 6-8 mg could be beneficial. I am certain the optimal dose will be different for different people." Kaeberlein 2023
He hasn’t gone into depth on his rationale, but one of his statements has been that higher doses likely help in getting rapamycin through the blood brain barrier. We’ve had some discussions on this and a look at the research in this area, in this thread: Rapamycin and the Issue of Getting Through the Blood Brain Barrier
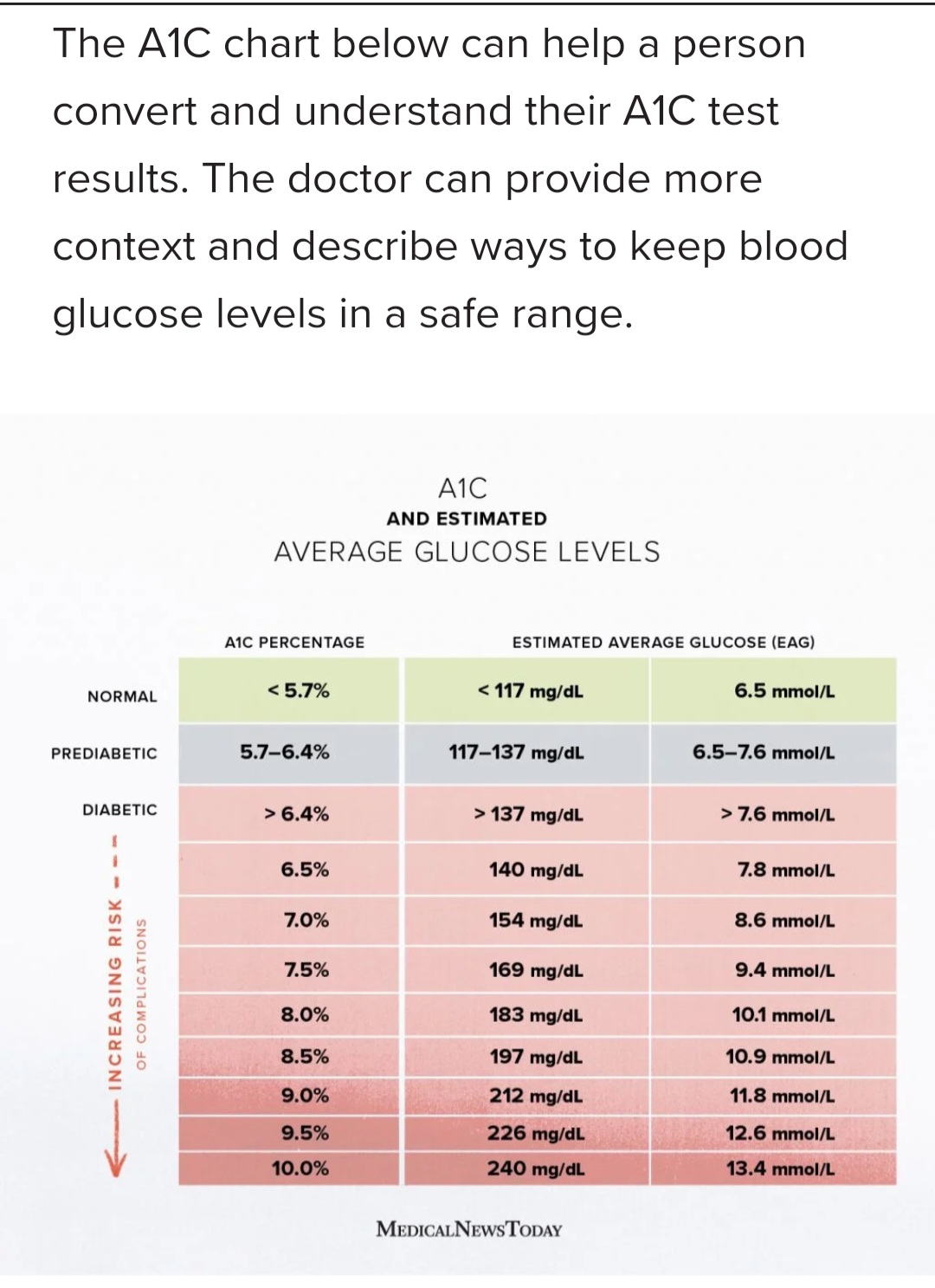
I know this is an old post but if you’re still here, I just had concerning A1C results as well. I had it as low as 4.8 in June 2023 but my recent test was 5.6.
The only two things I can point to are:
discontinuing DHEA (my recent level after stopping was 104, so I just went back on 50mg)
going from 5mg Rapamycin every week to 10mg every other week. It’s the same total dose per two weeks though. I’m going to take a month off and restart at 5mg per week.
I struggle to think of what else could have increased it.
A similar thing happened to me late last year: my hemoglobin, hematocrit, and MCHC were low; 11.3, 36.4, and 30.8. For the previous year I was taking 6mg rapamycin with grapefruit juice every 12 days. The above blood numbers had been trending down before I took notice in November.
Since early January, I have been having 1-2 oz of liver (beef, chicken, pork) per day, doubled by multi-vitamin from 1/2 to 1 full tablet (with iron included), made sure I had black pepper with iron to increase absorption, and separated consumption of iron foods from dairy and high fiber foods that might interfere with iron absorption. And I am taking a break from rapamycin.
I have been using a home hemoglobin test for several weeks (seems pretty accurate), and have gotten it up to a barely normal 13.6. Once I hit 14, I’ll resume rapamycin at a lower level and monitor the situation.
By the way, I also noticed that a late January measure of RDW had suddenly jumped from 14.1 to 15.9. Does that indicate lots of new red blood cells that made the mean width vary, since I understand that new RBCs are larger than mature ones?
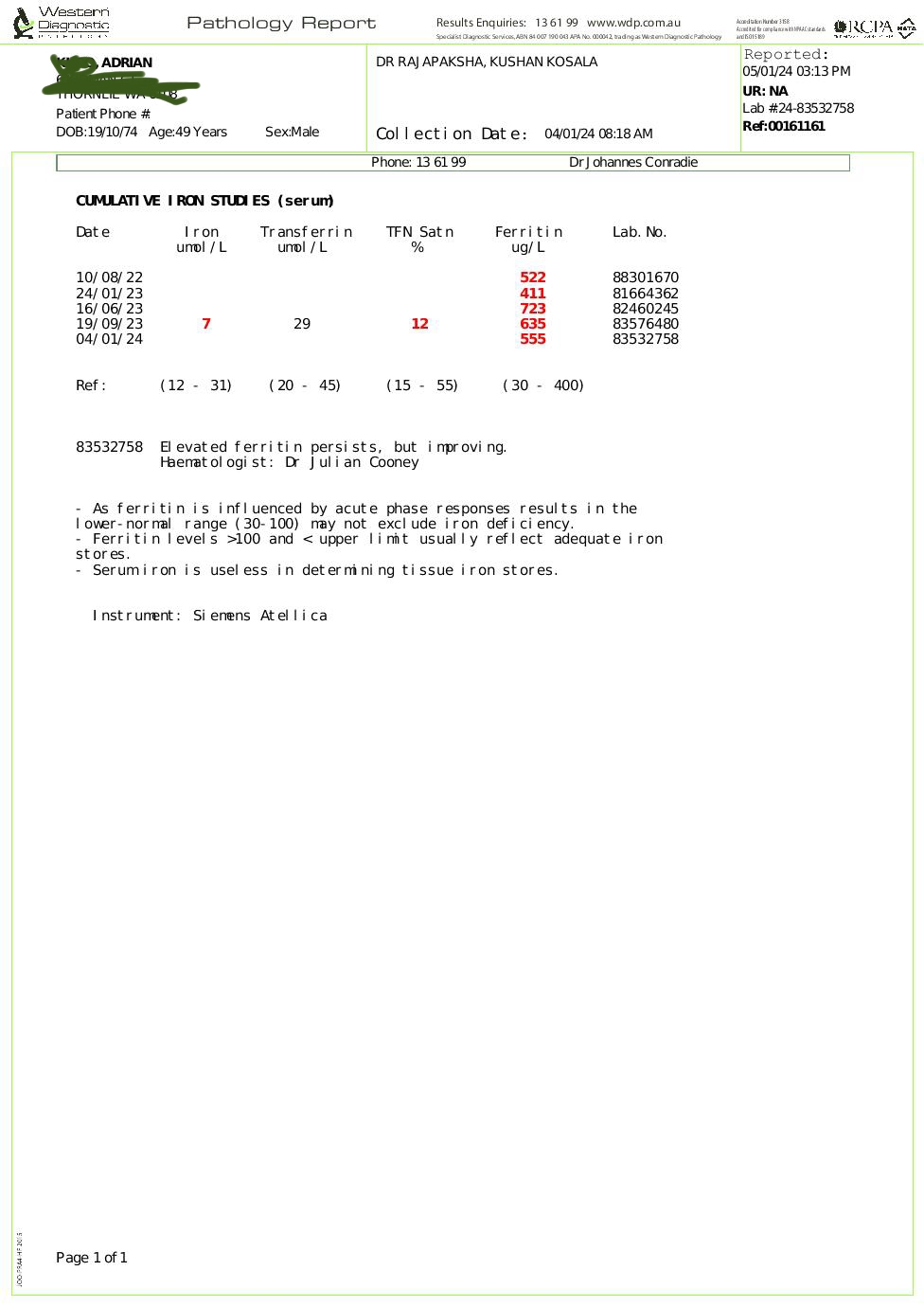
Are we suggesting that rapamycin will lower the iron level in our body? My iron level is been 2x to 3x above the maximum normal level. I hope that is good news for me.
I tried donating blood before. My blood pressure collapse and they told me not to come back . Anyway it used to be 5x over the upper limit. I’ve managed to reduce it but it is still consistently 2x over the limit.
My serum Iron has been reasonably consistent, but ferritiin has trended down. Doing weekly blood tests involves losing 10-15ml of blood a week. However, I don’t think that is the cause of the reduction in ferritin.
I cannot say what caused this beyond that it does not appear to be rapamycin. That is because it mainly dropped before i started rapamycin. It tended to link with citrate, but i cannot say that was the cause.