Yes, that’s absolutely a consideration for me, as I take several drugs.
1 Like
How do you know those aren’t hallucinations? And how is this better than just using https://promethease.com?
Thanks for flagging pitavastatin availability on cost plus. This is even cheaper than getting it from India
4 Likes
Maybe using ezetimibe plus bempedoic acid might be better for some than a statin.
I know many forum members are not big fans of Nick Norwitz. But he has a PhD from Oxford and an MD from Harvard, so he’s certainly no dummy.
I have been taking atorvastatin for decades, and I have not noticed any effects as dramatic as he has experienced. Perhaps my body has just grown used to the side effects so that I don’t notice them. I am going to switch to pitavastatin soon. In the meantime, I am going to try my own N=1 experiment, stopping atorvastatin and using just bempedoic acid and ezetimibe instead. Also, I am going to see whether replacing atorvastatin affects my glucose levels.
“A common practical approach is combination therapy at lower doses—ezetimibe plus bempedoic acid can achieve LDL reductions approaching moderate-intensity statin therapy without the muscle exposure, which may be why this combo has gained traction for statin-intolerant patients.”
AI response:
What this video is about:
The video documents a blinded $N=1$ crossover trial where Dr. Noritz compares the effects of a “gorilla dose” (80mg) of atorvastatin against a placebo. He tracks his performance using a high-intensity “ski erg” stress test and monitors for symptoms like myalgia (muscle pain) and fatigue. Ultimately, he explores the biological mechanisms behind statin-induced muscle issues and challenges the medical community’s tendency to downplay side effects in favor of drug benefits
This video features Dr. Nick Noritz investigating the controversial relationship between statins (cholesterol-lowering drugs) and muscle impairment. To move beyond observational data, he conducts a blinded, self-directed experiment to determine if high-dose statins directly impact his own physical performance and recovery. Beyond the biological results, the video serves as a social experiment on how personal narratives influence medical discourse compared to large-scale clinical studies.
Key Takeaways:
- The Experiment Design: The trial consisted of two 10-day phases (statin vs. placebo) with a three-week “washout” period in between. To ensure blinding, Dr. Noritz used a cheese grater to match the appearance of the statin and placebo pills.
- Performance Impact: During the statin phase, Dr. Noritz experienced significant leg pain and fatigue, leading to a dramatic decline in his workout performance starting around day six. He was forced to terminate the statin arm early due to a severely diminished quality of life.
- Potential Mechanisms: Several biological explanations are proposed for these effects, including:
- Mitochondrial Inhibition: Statins may inhibit “Complex 4” in the electron transport chain, creating a bottleneck in energy (ATP) production.
- CoQ10 Reduction: Statins can lower levels of Coenzyme Q10, a vital electron carrier for muscle metabolism.
- Fuel Restriction: For those on ketogenic or fat-adapted diets, statins might interfere with the body’s ability to circulate fat fuel.
- The Social Experiment: Dr. Noritz reveals that this personal “N=1” narrative is a test to see if it gains more traction than his previous video covering a formal 300,000-person study. He argues that while science values rigor, humans—including doctors—are evolutionarily wired to respond more strongly to personal stories.
Bottom Line
Statins likely can impair exercise performance and cause muscle symptoms in susceptible individuals — this n=1 trial showed dramatic negative effects within 6-10 days. However, the creator’s deeper message is about science communication: people (including doctors) are evolutionarily wired to learn through personal stories, not dry data. The video argues that medicine should acknowledge real-world side effects more transparently, and that storytelling is a legitimate — perhaps more effective — tool for spreading scientific truth than traditional rigor alone. Whether the performance results generalize to others remains unknown, but the biological plausibility is strong.
3 Likes
The hallucination issue is not related to that specific topic so I will not really address it. Just stating what I use which is Claude Max Opus 4.7 in max thinking mode and with the usual instructions to only use papers from reputable journals, provide citations, sources, etc.
Promethease is just a database of SNP without any mechanistic reasoning. It parses the genotype file and looks up every variant against SNPedia, which is a curated wiki of literature-cited associations.
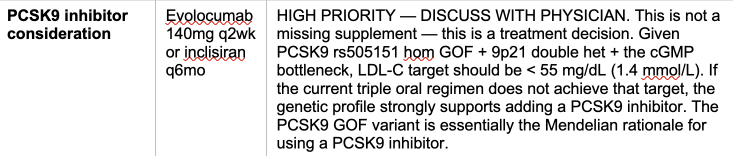
The main point I want to emphasis is how actionable the insights are. For instance I obviously have a plaque building issue as I got a stent at 61 even though no MD had ever told me to take a statin or anything else.
Looking at my genome I found out I have all the worst gain of function for PCSK9 so a PCSK9 inhibitor would be the best intervention.
I don’t have any SNP for Lp(a) and indeed I measured it at 9 mg/dl.
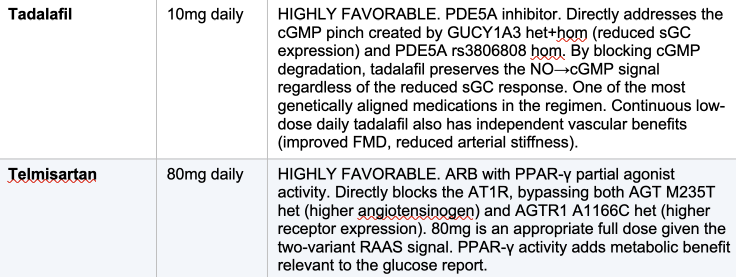
I also have some detrimental SNP on PED5 so tadalafil will help with that.
All that explain why with what was considered a somewhat normal LDL I developed a lot of plaque.
Finally I asked Opus to justify what it does better than Promethease:
5 Likes
For people following that thread here is the direct link. Blood Brain Barrier - A deep dive into genetic pathways for actionable insights
Thanks a lot! I’ll give it a try. Did you use Claude Cowork on the unzipped DNA folder from 23andme? Or did you use full genome sequencing from another provider? Would you mind sharing your prompt? By the way we should maybe discuss that in a new dedicated thread as it’s interesting to compare which model is best, prompts, etc.
1 Like
Sorry if this was covered already but where are you getting your genome from?
People like him make others distrust universities and science.
2 Likes
23andme decodes only about 0.1% of the genome but a full genome sequencing is needed. I used Nebula.org and Sequencing.com both at a 30x level because 100x was not available at that time. I spent days to merge and re-sequence the files to get a 60x. Now that 100x decoding is available, people should go for that if they can.
The prompt used for those reports is here.
I already have a dedicated discussion thread here.
And here is a more in-depth comparison between database lookup like promethease and what I do in those reports.
5 Likes
Thanks a lot!
And that would be?
The Cholesterol Balance Sheet: Why Your Lipid Ratio Outshines LDL for Sudden Death Risk
The Narrative Sudden cardiac death (SCD) remains a devastating cardiovascular outcome, often occurring without warning in individuals with underlying coronary heart disease. Traditional lipid management focuses heavily on individual markers like high-density lipoprotein (HDL-C) or low-density lipoprotein (LDL-C). However, a landmark study from the University of Eastern Finland published in Nutrition, Metabolism and Cardiovascular Diseases suggests that the “balance” between these lipids provides a far more accurate window into fatality risk.
Researchers analyzed data from 2,575 men in the Kuopio Ischemic Heart Disease (KIHD) prospective cohort over a median follow-up of 27.8 years. They focused on the non-high-density lipoprotein cholesterol-to-HDL-C ratio (NHHR). This ratio is calculated by taking total cholesterol, subtracting HDL-C to find the “pro-atherogenic” load (Non-HDL-C), and then dividing that number by the protective HDL-C.
The findings were stark: NHHR exhibited a linear, positive dose-response relationship with SCD risk. Men in the highest quartile of NHHR were 2.23 times more likely to suffer from sudden cardiac death than those in the lowest quartile. Critically, when NHHR was added to clinical models already accounting for smoking, diabetes, and blood pressure, it significantly improved risk prediction—something that measuring Non-HDL-C or HDL-C individually failed to do.
This research highlights that SCD is driven by a complex tug-of-war between plaque formation and cholesterol clearance. By integrating both atherogenic and anti-atherogenic fractions into a single index, the NHHR acts as a comprehensive “balance sheet” for arterial health. Because it can be calculated from routine blood tests without extra cost, it represents a practical, high-utility tool for clinical and personal health optimization.
Actionable Insights
-
Calculate Your Ratio : Monitor your NHHR regularly. In this cohort, the mean NHHR for survivors was 3.77, while those who suffered SCD had a mean of 4.26.
-
Target the Balance : Focus on both lowering atherogenic lipids (Non-HDL-C) and supporting protective HDL-C. Focusing on one while ignoring the other may obscure your true risk profile.
-
Standardize Testing : Blood samples in this study were taken after an overnight fast and 72 hours of alcohol abstinence to ensure accuracy. Replicate these conditions for consistent tracking.
-
Address Shared Risks : SCD risk is exacerbated by smoking, hypertension, and physical inactivity. Management of these lifestyle factors remains the foundation of cardiovascular longevity.
-
Monitor Inflammation : Higher hs-CRP levels (a marker of inflammation) were observed in SCD cases. Chronic inflammation works synergistically with high lipid ratios to promote plaque instability.
Context
- Open Access Paper: Serum non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio and the risk of sudden cardiac death: findings from a prospective cohort study
- Institution : Institute of Clinical Medicine, University of Eastern Finland.
- Country : Finland.
- Journal Name : Nutrition, Metabolism and Cardiovascular Diseases.
- Impact Evaluation: The impact score of this journal is approximately 3.3 to 4.5, evaluated against a typical high-end range of 0–60+ for top general science, therefore this is a Medium impact journal.
4 Likes
My NHHR is 2.2. Maybe I’ll pull through till cyclarity is out.
1 Like
Did we/study establish what an optimal NHHR is? and it is obvious that cohorts in highest quarter percentile would be at VERY high risk since to have a NHHR above 4.5 it would mean their LDL-C is well over 150, since HDL is for most people in the range of 40-60. In other words, I think this study is just proving the obvious.
As an example, at my worst reading I had what I considered poor numbers total 175, LDL-c 124 and HDL-C 39 and even with these numbers my NHHR of 3.5 (last test my NHHR is 1.9) would still be below the mean for the survivors, so this would mean I’m good whereas looking at LDL-C alone tells a different story. So, am I not better off looking at the LDL-C still?
To be fair I’m only going by the summary you posted and did not click on the link for details. .
I wonder if ApoB/HDL-c would be an even better marker for risk ?
When asked, the Medical AI, OpenEvidence.com states: The American College of Cardiology/American Heart Association 2026 Dyslipidemia Guideline recommends apoB alone as the preferred measure of atherogenic lipoprotein burden for ASCVD risk assessment and does not endorse the ApoB/HDL-C ratio as a recommended metric. The guideline emphasizes that apoB directly quantifies the number of atherogenic particles (one molecule per LDL, VLDL, and Lp(a) particle) and predicts ASCVD risk more accurately than LDL-C, particularly in settings of discordance — most commonly in individuals with cardiometabolic disease, diabetes, and/or triglycerides ≥150 mg/dL. In primary prevention, only apoB remained significantly associated with incident MI when assessed together with other atherogenic lipid measures (adjusted HR per 1 SD: 1.27; 95% CI, 1.15–1.40; P 0.001). The guideline recommends integrating apoB into routine risk stratification, supported by large cohort studies and meta-analyses demonstrating its superior predictive value compared with traditional lipid markers. No recommendation is made for lipid ratios incorporating HDL-C as a denominator for apoB-based risk assessment.
I suspect they did not evaluate ApoB/HDL-C for its strength as a risk indicator.
Mine is .76.
My overall risk is not low, but I’ll celebrate the wins!
Drugs are great! Congrats!
So I went to a cardiologist recommended by my doc. He couldn’t figure out how to get me a CCtA with Cleerly paid by medicare so he sent me to her. She got me a echo and ordered a CCTA, but I asked about Cleerly and she hates the machines. No AI for this one. She practically yelled at me. She said she could read better than the machine and the machine doesn’t care anyway. She offered me Leqvio probably because she correctly guessed I’m a person that might back out of the other kind. Thinks she can get it for free. We’ll see what happens after the CCTA, it’s in a couple weeks.
2 Likes
All I can add is that machines are helping the farmer with things I never thought would work. I’m not worried about being replaced though. It can’t do a round without me. But at the end of the day I’m less tired and get more done.
I really think that she could do more working with the machine. More people could see her and her advice could be better. Machines scan more carefully and don’t make mistakes. I’m sure they need to be checked manually, but it would take less time.
Work with the machines!
3 Likes
That paper seems useless. They conclude “NHHR is a stronger predictor of SCD risk compared to non-HDL-C and HDL-C”. OK but we don’t care. The only question is: is it a better predictor of SCD (sudden cardiac death) than apoB (and maybe RW-ApoB: RW-ApoB -- Superior Metric For Lipid Related CVD Risk --- Using Lp(a), ApoB, and Triglycerides)?
We already have a gold standard, it’s apoB. All the BS ratios have been around for decades and haven’t proved to be better than apoB.
7 Likes