Gas as my body adjusted but nothing since.
1 Like
Butyrate Reverses Structural and Inflammatory Hallmarks of the Aging Heart
The aging heart is a slow catastrophe. Year by year, the left ventricle stiffens and swells, filling with scar-like proteins, becoming increasingly unable to relax and fill properly between beats. This condition — diastolic dysfunction — is the dominant driver of heart failure in older adults, a syndrome called HFpEF (heart failure with preserved ejection fraction) that currently has almost no effective treatments. Finding an intervention that reverses this process, especially when started late in life, has been a central challenge in cardiac geroscience. This week, researchers at Stanford published a preprint that suggests something sitting at the bottom of your fiber supplement jar might help: butyrate, a short-chain fatty acid naturally produced by gut bacteria when they ferment dietary fiber.
The big idea is not just that butyrate is good for you — that has been suspected for some time — but that when given to aged mice as a daily supplement, starting at an age equivalent to roughly 60 years in humans and continued for ten months, it measurably reversed multiple hallmarks of a failing old heart. Mice receiving sodium butyrate (NaBu) in their drinking water showed less left ventricular enlargement, better diastolic filling dynamics, and improved surrogates of filling pressure compared to untreated aged mice of the same age. These are not trivial outcomes: they are the same metrics used in human echocardiography to grade diastolic dysfunction and HFpEF severity.
What elevates this work above a simple “butyrate is good” finding is the mechanistic depth. The Stanford team used a multi-omics framework — bulk left ventricular proteomics on a state-of-the-art Orbitrap Astral mass spectrometer, combined with single-nucleus multiome profiling (simultaneous RNA and chromatin accessibility mapping) — to map what butyrate was actually doing at the molecular level inside individual cardiac cell types.
The picture that emerged is striking. Aging drives the heart toward an inflammatory, extracellular-matrix-remodeling state dominated by complement system activation and immune priming of the vasculature. Butyrate partially reverses this, suppressing the classical complement cascade (the C1q complex), restoring metabolic proteins that decline with age, and — most compellingly — silencing an interferon and MHC-I “inflammatory priming” program in cardiac endothelial cells. This endothelial quieting was confirmed at both the RNA and chromatin level simultaneously, suggesting this is a genuine regulatory reprogramming event, not a transcriptional artifact.
Actionable Insights
The study highlights that targeting short-chain fatty acid pathways late in life can directly combat age-related cardiac remodeling and microvascular inflammation. For longevity biohackers, expanding the systemic pool of butyrate via targeted dietary fiber intake (e.g., resistant starch, inulin), prebiotic supplementation, or direct oral consumption of butyrate salts represents a highly practical strategy to protect cardiac elasticity in advancing age.
The real-world magnitude of these purported benefits is demonstrated by the large physiological effect sizes extracted directly from the study’s advanced echocardiographic and structural data:
- Left Ventricular Mass Normalization: Untreated aging caused absolute left ventricular weight to balloon from 95 mg to 120 mg. Long-term NaBu treatment almost entirely blunted this hypertrophic remodeling, reducing absolute LV mass back down to 98 mg—a near-complete structural rescue.
- Diastolic Function Recovery: The transmitral inflow velocity (E/A ratio), a key metric of passive filling performance, deteriorated by 50% during aging, dropping from 1.8 to 0.9. NaBu intervention restored the E/A ratio to 1.3, translating to a 44.4% structural recovery of age-induced diastolic filling decline.
- Filling Pressure Reduction: The noninvasive surrogate marker for left ventricular filling pressure (E/E’ ratio) spiked from 25 to 42 in aged controls, signaling high ventricular stiffness. NaBu suppressed this spike down to 31, eliminating roughly 64.7% of the age-associated filling pressure escalation.
Source:
- Open access paper: Butyrate preserves cardiac health during aging
- Institution : Department of Genetics, Center for Genomics and Personalized Medicine, Stanford University School of Medicine.
- Country : United States.
- Journal Name : bioRxiv Preprint, Posted June 08, 2026.
- Impact Score: The impact score of this journal is 0 (Un-peer-reviewed Preprint).
Analyst Note : While bioRxiv operates outside traditional citation impact metrics because it hosts pre-peer-review manuscripts, the study was generated by the laboratory of Michael P. Snyder, an elite, highly cited pioneer in functional genomics and multiomics. The rigorous generation of matched bulk proteomic and single-nucleus multiomic datasets warrants significant technical consideration despite its preprint status.
Critical Limitations
Despite the compelling multiomic landscape presented, several severe methodological and statistical vulnerabilities prevent immediate, high-confidence clinical translation:
Small Sample Size and High Multiomic Uncertainty
The single-nucleus multiome dataset (snRNA + snATAC) was generated utilizing only one single library per condition across the aging and NaBu comparison arms. As explicitly acknowledged by the authors under the “Limitations” section, a sample size of n=1 library per condition lacks any biological replication.
It is completely unpowered for population-level statistical inference or for capturing subtle cell-type composition changes accurately. These specific multiomic results must be interpreted purely as descriptive localization of candidate cellular states rather than definitive, generalizable proof. Furthermore, the bulk proteomic phase was limited to n=3 per group, leaving it highly vulnerable to sample variance, batch effects, and overestimation of biological effect sizes.
Exclusive Use of Male Cohorts
The study evaluated only male C57BL/6J mice. Due to pronounced sexual dimorphism in baseline gut microbiota compositions, varying baseline inflammatory dynamics, and distinct pathways governing left ventricular hypertrophic development between sexes, these data cannot be extrapolated to female cohorts [Confidence: Low].
Suprahysiologic Supplementation Dosing
The mice were administered a 1% w/v concentration of sodium butyrate continuously in their drinking water. This represents an enormous, highly suprahysiologic dosage that is unfeasible to replicate in human clinical settings via standard dietary fiber consumption alone. The study lacks any data establishing a dose-response curve or testing whether achievable, physiological human systemic concentrations can exert identical epigenetic or transcriptional remodeling inside highly structured cardiac tissues
5 Likes
Ideas on Actionable Interventions
1. Targeted Exogenous Sodium Butyrate (NaBu) Therapy
The Core Strategy
This intervention involves the oral administration of unesterified sodium butyrate to directly replicate the late-life treatment paradigm established in the study. The strategy targets systemic histone deacetylase (HDAC) inhibition and cardiac metabolic substrate utilization. The primary biological mechanism is the suppression of the classical complement cascade initiation complex (C1qa, C1qb, and C1qc) and the reversal of age-associated endothelial inflammatory priming (specifically dampening interferon-gamma pathways, Vcam1, Icam1, and MHC-I expression). The intended longevity outcome is the attenuation of age-induced left ventricular hypertrophy, reduction of myocardial filling pressures, and recovery of cardiac diastolic filling dynamics.
Translational Dosing Protocol
- Preclinical Paradigm: The study administered a 1% w/v concentration of NaBu continuously in the drinking water of mice.
-
Raw Mouse Dose Calculation: A standard 30-gram (0.03 kg) mouse consumes approximately 5 mL of water per day. At a 1% concentration (10 mg/mL), this translates to a daily intake of 50 mg of active compound.
Mouse Dose = 50 mg / 0.03 kg = 1,666.67 mg/kg/day -
Human Equivalent Dose (HED) Math: Using Body Surface Area (BSA) normalization where Mouse Km = 3 and Adult Human Km = 37:
HED = Animal Dose * (Animal Km / Human Km)
HED = 1,666.67 mg/kg/day * (3 / 37) = 135.14 mg/kg/day -
Total Human Daily Dose: For a standard 70 kg adult:
Daily Dose = 135.14 mg/kg/day * 70 kg = 9,459.8 mg/day (~9.5 grams daily) - Pharmacokinetics: Uncoated sodium butyrate exhibits poor systemic pharmacokinetics due to rapid, localized absorption by epithelial cells in the upper small intestine. Free butyrate possesses an exceptionally short plasma half-life of under 5 minutes because of rapid uptake and oxidation by colonocytes and robust hepatic first-pass clearance. Delayed-release microencapsulation is required to survive gastric transit and achieve measurable systemic levels.
Literature Validation & Source Verification
The necessity of utilizing advanced microencapsulation technology to optimize the release profile, clinical tolerance, and systemic efficacy of oral butyrate has been comprehensively reviewed by Pieszka et al., 2026. The direct molecular mechanics of sodium butyrate in repressing downstream inflammatory mediators, restoring barrier functions, and mitigating NF-kB and NLRP3 pathways have been validated in human epithelial and macrophage models by Wang et al., 2025.
Safety, Toxicity, & Interaction Profile
- NOAEL: The rodent No Observed Adverse Effect Level (NOAEL) for oral sodium butyrate is documented at 1,000 mg/kg/day. Doses exceeding 2,000 mg/kg/day can induce transient gastrointestinal distress, osmotic diarrhea, and localized upper mucosal irritation.
- Toxicity Signals: Liver and kidney toxicity signals are completely absent at standard translated doses.
- CYP450 Interactions: Sodium butyrate does not act as a direct competitive substrate for core cytochrome P450 enzymes. However, long-term HDAC inhibition can indirectly alter the transcriptional expression profiles of CYP1A1 and phase II conjugation pathways, potentially modifying the clearance rates of co-administered xenobiotics.
Longevity Stack Compatibility
- Rapamycin: Fully compatible; no overlapping clearance mechanisms or target contradictions.
- Metformin: Synergistic. Metformin alters the gut microbiota to enrich for butyrate-producing strains; co-administration of exogenous NaBu can amplify initial gastrointestinal side effects (bloating, cramping) but yields positive metabolic convergence.
- SGLT2 Inhibitors: Complex interaction. SGLT2 inhibitors shift systemic energy substrate utilization toward ketone body oxidation. Because butyrate also serves as an oxidative short-chain fatty acid substrate within the myocardium, concurrent dosing may introduce cardiac metabolic substrate competition.
- Acarbose: Similar to metformin, acarbose increases the delivery of unfermented carbohydrates to the colon, spiking endogenous SCFA production. Concurrent high-dose exogenous NaBu may generate significant gastrointestinal distress.
- 17-Alpha Estradiol & PDE5 Inhibitors: Fully compatible; no known overlapping clearance pathways or mechanistic contradictions.
2. Exogenous Tributyrin (Butyrate Prodrug) Protocol
The Core Strategy
Tributyrin (glyceryl tributyrate) is a structured triglyceride containing three butyrate molecules esterified to a glycerol backbone. This strategy is explicitly designed to circumvent the severe pharmacokinetic limitations of free sodium butyrate salts. By utilizing a prodrug architecture, butyrate is protected from immediate absorption in the upper stomach and is instead progressively cleaved and liberated throughout the small intestine and proximal colon via pancreatic lipases. This delivers a sustained, continuous systemic trough of butyrate that closely mimics the chronic, long-term exposure model utilized in the Stanford mouse study. The biological target remains the down-regulation of endothelial interferon-gamma activation and vascular cell adhesion molecule-1 (Vcam1) expression to treat microvascular inflammaging.
Translational Dosing Protocol
- Preclinical Paradigm: Preclinical models utilizing tributyrin to achieve reliable systemic target engagement apply an average of 1,500 mg/kg/day in rodents.
-
Human Equivalent Dose (HED) Math:
HED = 1,500 mg/kg/day * (3 / 37) = 121.62 mg/kg/day -
Total Human Daily Dose: For a 70 kg human:
Daily Dose = 121.62 mg/kg/day * 70 kg = 8,513.4 mg/day (~8.5 grams daily) - Pharmacokinetics: Tributyrin exhibits vastly superior lipophilicity and oral bioavailability compared to standard sodium butyrate. It remains stable during gastric transit and possesses a prolonged plasma half-life of approximately 40 minutes. Human clinical data demonstrates that target engagement and systemic anti-inflammatory actions can be successfully achieved at much lower pragmatic doses due to this enhanced bio-efficiency.
Literature Validation & Source Verification
The clinical utility, safety, and organ-specific target engagement of oral tributyrin in humans were successfully demonstrated in an open-label human trial conducted by O’Connor et al., 2026. Utilizing carbon-11 labeled butyrate positron emission tomography (PET) imaging, the investigators confirmed that an oral regimen of 1,500 mg daily (split into three 500 mg doses) successfully achieved direct organ-specific uptake in the heart, liver, and brain, while inducing distinct systemic anti-inflammatory modifications.
Safety, Toxicity, & Interaction Profile
- NOAEL: Broadly recognized as safe with an animal NOAEL of 1,680 mg/kg/day.
- Toxicity Signals: Extreme overdosing in rodent diets (exceeding 5% of total dietary volume) has been noted to produce reversible gastric mucosal lesions and localized epithelial irritation due to excessive high-volume local acid release.
- CYP450 Interactions: No direct competitive inhibition or activation of major cytochrome P450 enzymes has been reported.
Longevity Stack Compatibility
- Rapamycin, Metformin, SGLT2 Inhibitors, Acarbose, 17-Alpha Estradiol, PDE5 Inhibitors: Showcases an identical compatibility profile to sodium butyrate, but presents significantly reduced gastrointestinal bloating and improved compliance due to the absence of the volatile, rancid-butter odor characteristic of free butyrate salts.
3. High-Amylose Resistant Starch (HAS) Endogenous Fermentation
The Core Strategy
Instead of introducing exogenous short-chain fatty acids, this intervention leverages the metabolic capacity of the host gut microbiome to optimize endogenous butyrate production directly within the colon. Type-2 and Type-4 resistant starches escape enzymatic digestion in the upper gastrointestinal tract and arrive intact in the large intestine. Here, they serve as specialized substrates for primary fermenting bacteria (such as Faecalibacterium prausnitzii and Eubacterium rectale), shifting the microbiome toward a highly butyrogenic profile. The continuous slow-release absorption of colon-derived butyrate enters the portal and systemic circulation, exerting long-term, non-toxic systemic HDAC inhibition to blunt myocardial complement complex deposition (C1qa/b/c) and reduce cardiac filling pressures.
Translational Dosing Protocol
- Preclinical Paradigm: Preclinical models typically replace 5% to 10% of standard rodent chow with pure resistant starch to induce robust systemic butyration shifts, translating to an average animal dose of approximately 10,000 mg/kg/day.
-
Human Equivalent Dose (HED) Math:
HED = 10,000 mg/kg/day * (3 / 37) = 810.8 mg/kg/day -
Total Human Daily Dose: For a 70 kg human:
Daily Dose = 810.8 mg/kg/day * 70 kg = 56,756 mg/day (~56.7 grams daily) - Pharmacokinetics: Resistant starch provides an ideal, sustained-release pharmacokinetic profile. Rather than creating a sharp, transient spike in plasma butyrate (as seen with oral salts), microbial fermentation occurs continuously over a 6 to 24-hour colonic transit window. This ensures steady, continuous exposure of the vascular endothelium to low-dose butyrate. Human clinical trials prove that a pragmatic intake of 20 to 40 grams daily of high-purity Type-2 or Type-4 resistant starch is sufficient to optimize systemic butyrate production and generate therapeutic immune modifications.
Literature Validation & Source Verification
The capacity of resistant starch type 4 (RS4) to drive butyrogenic shifts and downregulate fundamental pro-inflammatory pathways via specific chromatin modifications has been validated in vivo by Martinez et al., 2016. They demonstrated that RS4-derived butyrate increases tri-methylation of lysine 27 on histone 3 (H3K27me3) to directly repress the promoter of the pro-inflammatory master-regulator nuclear factor-kappa-B1 (NF-kB1). Furthermore, a systematic review and meta-analysis of 16 randomized controlled trials by Wang et al., 2021 confirmed that resistant starch supplementation significantly reduces circulating C-reactive protein (CRP), interleukin-6 (IL-6), and oxidative stress biomarkers in human clinical cohorts.
Safety, Toxicity, & Interaction Profile
- NOAEL: Safety Data Absent for an upper toxic limit; classified as a safe dietary fiber macronutrient component.
- Toxicity Signals: Exceeding 60 grams daily can induce benign, dose-dependent gastrointestinal side effects including flatulence, abdominal distension, tympanites, and transient loose stools due to accelerated microbial gas production (hydrogen and methane).
- CYP450 Interactions: Completely inert; zero direct interaction with any cytochrome P450 enzyme cascades.
Longevity Stack Compatibility
- Metformin & Acarbose: Highly interactive but mechanistically synergistic. Both metformin and acarbose independently shift carbohydrate transit to reinforce butyrate-producing microbial populations. Combining them with high-dose resistant starch will significantly compound initial gastrointestinal gas production, requiring careful, upward titration of fiber dosing over several weeks to build tolerance.
- Rapamycin, SGLT2 Inhibitors, 17-Alpha Estradiol, PDE5 Inhibitors: Completely compatible.
4. Creatine Monohydrate Adjuvant Therapy
The Core Strategy
A key discovery within the Stanford study’s bulk proteomic dataset was that natural cardiac aging causes a severe, coordinated downregulation of critical bioenergetic and cellular homeostasis networks—specifically prioritizing a major collapse in mitochondrial creatine kinase (Ckmt1) and glycogen phosphorylase (Pygl) expression. Butyrate administration successfully reversed this direction, placing both proteins into the core 92-protein “rescue” module. To directly target and fortify this specific metabolic network from an actionable standpoint, oral Creatine Monohydrate supplementation is utilized. By maximizing intracellular phosphocreatine reserves, this strategy preserves the essential creatine kinase phosphagen shuttle within excitable tissues. This enables immediate, non-glycolytic ATP regeneration during periods of high myocardial workload, directly combatting the energetic deficits that drive age-associated left ventricular hypertrophy and diastolic stiffness.
Translational Dosing Protocol
- Preclinical Paradigm: Rodent models for optimizing tissue-specific creatine kinase kinetics typically utilize a 1% w/w concentration of creatine in standard chow. For a 30-gram mouse eating 4 grams of food daily, this equates to 40 mg of creatine per day, yielding an animal dose of 1,333.33 mg/kg/day.
-
Human Equivalent Dose (HED) Math:
HED = 1,333.33 mg/kg/day * (3 / 37) = 108.11 mg/kg/day -
Total Human Daily Dose: For a 70 kg human:
Daily Dose = 108.11 mg/kg/day * 70 kg = 7,567.7 mg/day (~7.5 grams daily) - Pharmacokinetics: Creatine monohydrate displays near-complete oral bioavailability (~99%) and reaches peak plasma concentration within 1 to 2 hours. It is actively extracted from circulation into cardiomyocytes and skeletal muscle fibers via the specific sodium/chloride-dependent plasma membrane creatine transporter (CrT). A standard human loading protocol of 20 grams daily (split into four 5-gram doses) for 5 to 7 days rapidly achieves full tissue saturation, which is then indefinitely maintained via a single daily dose of 5 grams.
Literature Validation & Source Verification
The structural architecture and necessity of the myocardial creatine kinase shuttle in preventing left ventricular contractility reserve depletion and mortality have been thoroughly mapped out by Santacruz et al., 2021, establishing a direct clinical rationale for supplemental creatine to defend myocardial energy reserves. Furthermore, the application of creatine supplementation to counteract multi-organ physiological, muscular, and cellular decline during human aging has been comprehensively reviewed by Clarke et al., 2026.
Safety, Toxicity, & Interaction Profile
- NOAEL: Extensively documented human safety profile; continuous dosing at 5 to 10 grams daily shows zero adverse effects over multi-year timelines.
- Toxicity Signals: Anecdotal concerns regarding renal toxicity are clinically unfounded in individuals with healthy baseline kidney function. Supplementation predictably increases serum creatinine levels (a benign byproduct of non-enzymatic creatine degradation), which can artificially alter estimated Glomerular Filtration Rate (eGFR) calculations without signifying authentic structural renal damage.
- CYP450 Interactions: Completely inert; does not interact with cytochrome P450 pathways.
Longevity Stack Compatibility
- Metformin: Fully compatible; no negative interactions.
- SGLT2 Inhibitors: Synergistic fluid dynamic profile. SGLT2 inhibitors act as mild diuretics and alter systemic volume status, whereas creatine promotes osmotic intra-cellular water retention within excitable cell types. Co-administration requires adequate daily hydration but offers highly robust cellular hydration characteristics.
- Rapamycin, Acarbose, 17-Alpha Estradiol, PDE5 Inhibitors: Completely compatible.
Part 2: Strategic Feasibility & Target Engagement
Sourcing & Financial ROI Evaluation
A comparative evaluation of procurement status, structural access tier, and estimated monthly cost-to-benefit ratio for maintaining the calculated translational dosing protocols in a human longevity regimen:
1. Targeted Exogenous Sodium Butyrate (NaBu)
- Procurement Status: Over-The-Counter (OTC) Supplement / Food Additive.
- Access Tier: Readily accessible via commercial channels. However, standard raw sodium butyrate powder is highly unpalatable and rapidly cleared. Biohackers must source specialized, third-party tested, enteric-coated or microencapsulated formulations (e.g., calcium/magnesium/sodium butyrate matrices) optimized for delayed colonic release.
- Estimated Monthly Cost: $45 – $75 per month (to consistently achieve a target intake of 4 to 6 grams daily of active microencapsulated butyrate).
- Cost-to-Benefit ROI Assessment: Moderate-Low. Due to inherently high first-pass clearance and poor systemic retention, large oral doses of raw salts yield sub-optimal systemic bioavailability, making it an expensive route to sustain the high therapeutic trough concentrations highlighted in the data.
2. Exogenous Tributyrin (Butyrate Prodrug)
- Procurement Status: OTC Supplement / Advanced Nutraceutical.
- Access Tier: Commercially available through premium, specialized supplement manufacturers. Products must explicitly state “Tributyrin” or “Glyceryl Tributyrate” on the Certificate of Analysis (COA) rather than vague “butyric acid blends”.
- Estimated Monthly Cost: $60 – $110 per month (dosed clinically at 1,500 mg to 3,000 mg daily).
- Cost-to-Benefit ROI Assessment: High. Given its stable lipid-ester structure, it bypasses upper gastric degradation, possesses a prolonged systemic half-life, and achieves direct organ-specific and cardiac tissue uptake at highly achievable oral doses. This delivers a superior pharmacokinetic ROI compared to raw NaBu salts.
3. High-Amylose Resistant Starch (HAS)
- Procurement Status: Whole Food Ingredient / Raw Bulk Macronutrient Powder.
- Access Tier: Highly accessible and inexpensive. Can be procured as unmodified, raw potato starch (unheated), green banana flour, or chemically cross-linked Resistant Starch Type 4 (RS4) powders.
- Estimated Monthly Cost: $15 – $30 per month (to sustain a continuous daily intake of 30 grams).
- Cost-to-Benefit ROI Assessment: Elite. This represents the most financially efficient and highly sustainable strategy to chronically upregulate systemically available butyrate. It maximizes endogenous production along the entire length of the large intestine, ensuring stable, 24-hour systemic delivery while avoiding the compliance obstacles of exogenous supplementation.
4. Creatine Monohydrate
- Procurement Status: OTC Supplement / Bulk Sports Nutrition.
- Access Tier: Universally accessible. Biohackers should purchase pure Creapure or micronized creatine monohydrate powder with verified heavy metal clearances on the manufacturer’s COA.
- Estimated Monthly Cost: $10 – $20 per month (for a standard 5-gram continuous daily maintenance protocol).
- Cost-to-Benefit ROI Assessment: Elite. Creatine has an incredibly low cost-of-entry coupled with a virtually flawless human safety profile and absolute structural necessity for sustaining cardiac and skeletal muscle phosphagen pools during aging. It directly addresses the critical Ckmt1 bioenergetic target highlighted in the paper’s proteomic data.
1 Like
Follow-on Prompt:
List and identify and link to any available off-the shelf Delayed-release microencapsulated sodium butyrate, include approximate pricing and calculate the price per gram for each option. Provide links to the websites where the product may be purchased.
Gemini Response:
To achieve reliable systemic target engagement without rapid upper gastrointestinal degradation or unpalatable compliance issues, several specialized off-the-shelf formulations utilize advanced delayed-release microencapsulation or molecular-trap technologies.
Below is an objective, technical evaluation of the primary commercial options available on the international and domestic markets, including absolute pricing metrics and calculated costs per gram of active compound.
1. Debutir Forte (Silesia / Polfa Łódź)
- Technology & Mechanism: This formulation represents a true microencapsulated sodium butyrate matrix (MSB). The active sodium butyrate salt is structurally embedded within a protective triglyceride core matrix (primarily composed of hydrogenated palm oil derivatives). This lipid shield remains stable in gastric acid and is only broken down gradually as it encounters pancreatic lipases in the small intestine and distal colon, preventing early gastric dissociation.
- Package Specifications: 60 capsules per box; 300 mg of microencapsulated sodium butyrate per capsule.
- Total Active Yield: 60 capsules x 0.300 grams = 18.0 grams of sodium butyrate per container.
- Approximate Retail Pricing: ~55.00 PLN (~$14.00 USD) across European pharmaceutical networks.
-
Price Per Gram Calculation:
$14.00 USD / 18.0 grams = $0.78 USD per gram - Purchase Storefront Link: Debutir Forte is classified as a medical food in Europe and can be procured via major international pharmacy fulfillment portals and regional aggregators such as Ceneo Pharmaceutical Network or Apotheke DE Directory.
2. ProButyrate (Ecological Formulas)
- Technology & Mechanism: ProButyrate circumvents upper GI clearance by employing a unique molecular entrapment architecture known as a cycloamylose clathrate matrix. Rather than a physical lipid shell, the butyrate molecule is trapped inside the hydrophobic core of a cyclodextrin ring structure. This molecular proxy for microencapsulation resists gastric degradation and delays liberation until the compound undergoes competitive displacement in the lower intestinal tract.
- Package Specifications: 120 capsules per bottle; 200 mg of active butyric acid core equivalent per capsule.
- Total Active Yield: 120 capsules x 0.200 grams = 24.0 grams of active butyrate equivalent per container.
- Approximate Retail Pricing: ~$42.00 USD on domestic clinical supplement platforms.
-
Price Per Gram Calculation:
$42.00 USD / 24.0 grams = $1.75 USD per gram - Purchase Storefront Link: This formulation is readily available in the United States through clinical supply houses and professional-grade supplement distributors such as PureFormulas Storefront or directly via the manufacturer’s network at Ecological Formulas.
3. Butyrose (SILA S.p.A.)
- Technology & Mechanism: Butyrose consists of microencapsulated granules optimized for colonic release. The sodium butyrate is coated in a specialized fat-based shell designed for a delayed, step-wise release curve that targets the distal colon. It has been extensively utilized in European clinical trials evaluating microvascular and bowel mucosal inflammation.
- Package Specifications: 30 capsules per container; 500 mg of microencapsulated granules per capsule, yielding approximately 200 mg of active butyrate core per capsule after subtracting the weight of the lipid encapsulation matrix.
- Total Active Yield: 30 capsules x 0.200 grams = 6.0 grams of active butyrate core per container.
- Approximate Retail Pricing: ~€24.00 (~$26.00 USD) across Mediterranean pharmaceutical networks.
-
Price Per Gram Calculation:
$26.00 USD / 6.0 grams = $4.33 USD per gram - Purchase Storefront Link: Available as a specialized gastrointestinal medical food through European pharmacy distribution networks and direct manufacturer pipelines including SILA S.p.A. Official Portal and Farmacia Loreto.
Critical Procurement Summary
From a financial and structural efficiency perspective, Debutir Forte delivers the highest raw return on investment at $0.78 per gram, making it the most viable option for executing high-dose translational longevity protocols in humans. However, because it is an overseas pharmaceutical product, domestic users inside the United States may face shipping delays or import logjams. For immediate domestic availability, ProButyrate provides a reliable molecularly-delayed alternative at $1.75 per gram without the compliance friction of customs border processing.
1 Like
A new related video and transcript summary:
2 Likes
Hi, Sorry took so long. I do not think the fiber had much to do with weight loss. I have been doing Inulin and psyllium husk for over a year with not much noticeable weight change. I think it was the combination of Rapamycin and Tributyrin-max. I stopped both for past 8 weeks and stayed at 189lbs. I plan to restart them both using the 2 week schedule mentioned above when mixing them with weight training. Also weird and maybe coincidental with adding Tributyrin is like some switch tripped in my body and did not reset during the 8 weeks off. Maybe my 67 years finally caught up to me and i just got old… It is frustrating to continue going to gym 3 days a week (take 5g Creatine every day also) and not see any gains for past months. Now with 2 week cycle, ill focus more on cardio and reserve last 4 days of cycle to hard work in gym… Will see. My doctor just prescribed Tesamorelin peptide since i complained how hard it is to maintain muscle mass… Will see here too. Planning to try 1 month. Apparently it stimulates human growth hormone to reduce visceral fat while building more muscle with the added benefit of reducing fatty liver (which when i was measured 2 years ago I was in 27th percentile).
1 Like
Hi Sorry late reply. I attribute the drop to adding the Tributyrin-max daily for 2-3 months prior to 0.2 test (sometimes I took 2 pills per day (Moring / bedtime)). I read the mix with rapamycin enhances/makes more efficient mTor1 effects as well as hitting the Ampk pathway with Tributyrin. It seems one of the original posts from RapAdmin mentioned to expect a good drop in hs-crp. Frankly I was shocked - like maybe they mixed up my blood. I mean also my cholesterol panel all green never happened to me - i was always high with LDL and number and particle size, etc. Also ApoB was never below 100 till last test. Will see when i go back for another draw next month if the last tests were some anomaly.
2 Likes
8 things to know about the gut microbiome and keeping yours healthy
3 Likes
A Butyrate Optimizing Protocol example
Maximizing colonic butyrate is less about megadosing one fiber and more about feeding several different degrader guilds at once, because butyrate output depends on a relay: primary degraders break down fiber → produce acetate and lactate → cross-feeders (Faecalibacterium, Roseburia, Eubacterium, Anaerostipes) convert those into butyrate. So the protocol below deliberately spreads across fiber classes rather than loading one. Treat all numbers as titration targets, not day-one doses — ramp over 3–4 weeks or you’ll just generate gas and quit.
Fiber targets (grams/day, ramped)
| Fiber class | Target/day | Why it matters | Practical sources |
|---|---|---|---|
| Resistant starch (RS2/RS3) | 20–40 g | The single most butyrogenic class; feeds R. bromii (keystone RS degrader) → cascades to butyrate producers | Raw (unmodified) potato starch ~8 g RS/tbsp → 2–4 tbsp in cold liquid (never heat it); green banana flour 1–2 tbsp; cooled cooked rice/potato (a few g each); cooked-then-cooled legumes (lentils/beans, ~1 cup) |
| Inulin-type fructans / FOS | 5–15 g(start 3–5 g) | Bifidogenic; drives the acetate cross-feed that supplies F. prausnitzii | Chicory inulin ~5–10 g, or whole food: 2–3 garlic cloves + ½ onion + 1 leek + asparagus + Jerusalem artichoke |
| Beta-glucan | 3–6 g | Strongly butyrogenic, especially barley > oat | 60–80 g dry oats ≈ 3 g; pearl/whole barley is richer per gram |
| Arabinoxylan / whole-grain fiber | 5–10 g | Well-tolerated butyrogenic fiber, low FODMAP | Wheat/oat bran, rye, whole grains |
| Pectin + mixed soluble fiber | ~5–10 g | Moderately butyrogenic, adds diversity | Apple with skin, citrus, carrot, psyllium (~1 tbsp) |
| Total fiber | 35–50 g | Diversity is the real lever | Aim ~30 distinct plant species/week |
The RS line is where most people under-dose, and it’s the highest-leverage one. Raw potato starch is the cheapest way to reliably hit RS targets, but it does nothing if heated, so it goes in cold water, kefir, or a smoothie. Resistant starch only converts well to butyrate if you actually harbor Ruminococcus bromii — response is genuinely individual, so judge by tolerance and effect, not the spreadsheet.
One correction worth holding onto from before: the cooled rice/potato/green banana foods are resistant starch, while garlic/onion/chicory are inulin/FOS — different guilds. Running both lists simultaneously is the point, because it feeds parallel degrader populations that converge on butyrate.
Probiotics that support the chain
Direct butyrate-producing probiotics barely exist commercially — F. prausnitzii is extremely oxygen-sensitive and still only in development as a live biotherapeutic, not on shelves. So most useful strains work by feeding the cross-feeding network rather than making butyrate themselves. In rough order of on-target relevance:
Clostridium butyricum (the MIYAIRI 588 strain, sold as Miyarisan in Japan/Asia) is the closest thing to a direct butyrate-producing probiotic you can actually buy. Bifidobacterium adolescentis and B. longum are the acetate engines for the cross-feed — pairing them with inulin is the synergy your original post was reaching for. Lactate-producing lactobacilli (Lactiplantibacillus plantarum and others in any decent multi-strain blend) feed the lactate→butyrate step via Anaerostipes and Eubacterium hallii. Akkermansia muciniphila (now sold in pasteurized form) doesn’t make butyrate but reliably stimulates butyrogenic populations via mucin cross-feeding. Spore-based Bacillus blends have modest evidence for shifting communities toward SCFA production.
Realistically, probiotics are a minor lever next to consistent fiber — the resident community does the heavy lifting, and you can’t colonize what you don’t feed.
Fermented foods
Their role isn’t to deliver butyrate directly (most contain little to none) — it’s diversity, anti-inflammatory signaling, and supplying lactate/acetate-producing live microbes that feed the relay. The relevant evidence is the Stanford trial (Wastyk et al., Cell 2021), where a fermented-food diet raised microbiome diversity and lowered inflammatory markers — notably outperforming the high-fiber arm on inflammation. That study escalated to roughly 6 servings/day, which is a reasonable ceiling to build toward.
Practical mix, variety mattering more than volume: kefir (~1 cup) and live-culture yogurt as the dairy base; sauerkraut and kimchi (2–4 tbsp each, raw/unpasteurized — shelf-stable canned versions are dead); miso (~1 tbsp, stirred in off-heat); natto or tempeh for Bacillus and a different microbial profile. Kombucha counts but is lower priority given the sugar. Start at one serving and add one every few days.
Caveats
The inulin/FOS and allium sources are high-FODMAP — if you have IBS or SIBO, these are exactly the foods that trigger bloating and pain, and “maximize” is the wrong frame for you; start minimal and titrate, or substitute the better-tolerated arabinoxylan/RS routes. There’s also a tolerance ceiling where more fiber just means more gas with no extra butyrate, so diversity beats brute dose. And I’m giving you mechanism and population-level ranges, not personalized medical advice — if you have a GI condition or are managing one, run this past a clinician who knows your case.
Butyrate_Protocol.pdf (33.9 KB)
3 Likes
I’ve gotten different answers from AI on TMAO. Whether RS makes it worse or unbearable or whether it even matters to heart disease. Whether I should take it with phosphatidylcholine, it says I should. Also it says to take Garlic extract with it because it inhibits the TMA Lyase enzyme, which stops the TMAO altogether. Berberine does this also and is actually better at it. I think to be safe levels should be tested probably before and after a week or so of RS. Some have to worry more than others.
3 Likes
@CronosTempi and @cl-user
How do you guys make homemade kefir(recipe). I know how to make yogurt but never made kefir.
1 Like
ok, but what was it before? meaning what was the delta?
1 Like
I wouldn’t feed nitrate to my worst enemies (probably would to my ex m-in low though LOL). Just recently read an article that it can be very dangerous to liver and kidneys.
1 Like
Really easy:
- buy the kefir grains, eg: Amazon.com: Simply Life Probiotics Milk Kefir Grains,Turkish Strain, Pajaritos de Leche, Bulgaros, Homemade Kefir, Live Probiotics : Grocery & Gourmet Food
- Put grains in jar for 2 days (or so) with milk, and let sit at room temperature.
- Kefir is ready.
4 Likes
I fluctuated between 0.6 and 0.9 HS-CRP in the year prior. Not sure of the error bars on these tests, so it may not be significant.
2 Likes
I see, oh well if the number went down that’s better than up, regardless of error bars.
1 Like
For kefir, you will also need a strategy for separating the grains from the kefir when finished. I am experimenting with reusable cotton tea bags.
2 Likes
Paper:
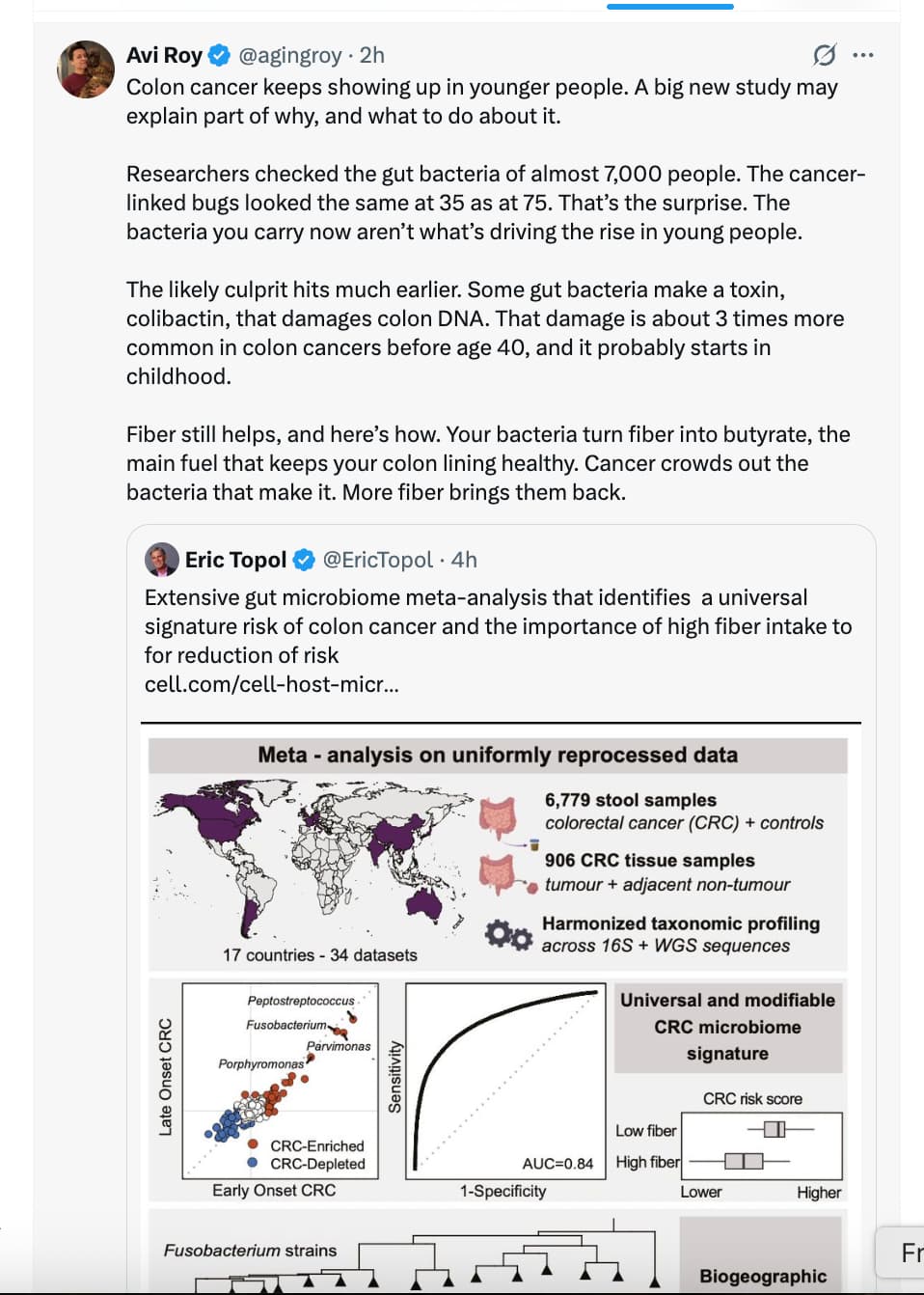
Meta-analysis reveals microbiome signatures for colorectal cancer that are universal across age groups and sequencing methods
https://www.cell.com/cell-host-microbe/fulltext/S1931-3128(26)00223-4
1 Like
Yes, nitrates can be toxic in excess, but we were discussing citrates.
1 Like
RapAdmin has it, yes it’s very simple. Just buy grains that come in a little reusable floater, that way you don’t have to worry about separating the grains after kefir is made, Just drop the floater into the container with milk, let the kefir form, remove the floater, rinse it thoroughly under flowing water and put it into a small dish with a bit of milk and put it in the fridge if not using. But if you are using it continuously, just pop it into a new batch. My wife makes kefir 1-2 times a week, so I consume it 1-2 times a week. Key point of maintenence: make sure that you rinse the grains thoroughly, so only they remain. The floater itself should also be cleaned - obviously don’t use chemicals to clean, or you’ll kill the grains.
1 Like