What was it that you think contributed to such a big drop. 0.2 is pretty amazing.
After examining the evidence, this article concludes that both Stalin’s disease course and the properties of warfarin make it highly unlikely that he was deliberately assassinated.
2 Likes
I read that one of the people who was with him the night before claimed that he & his buddies had poisoned him. That doesn’t make it true, but it does make a good story. ![]()
1 Like
I had big issue with reflux and acidosis also and tried a lot of things, and nothing seemed to work, until recently that I started taking Nattokinase 10000 FU and Serrapeptase 240.000 and my symptoms have totally disappeared. It was a nice surprise/side effect as my reason for taking them initially was for blood thinning and inflammation which they seem to do a good job at that also.
1 Like
Did you measure/do labs pre and after or you are basing it in the way you feel.
I’ve never had an hs-CRP test, mainly because of cost. And I was mistaken about ginger. It does help with indigestion but doesn’t do much for inflammation. I’m waiting for the tributyrin and lactoferrin to kick in.
1 Like
“Swanson PectiPure Modified Citrus Pectin Cellular and Digestive Health Supplement for Wellness-Conscious Adults - 82% Galacturonic Acid (60 Capsules, 600 mg Each)”
Nothing notable except they are a trusted brand with reasonable prices.
Actually, I think ginger does help but I was wondering if you had real measurable results. I bought it couple days ago and I think it will be something I’ll continue taking it daily as part of my daily regimen.
Acid Reflux and Acidosis are two different things. Those two enzymes could have helped you with reflux, but they couldn’t do anything for acidosis. Acidosis is an imbalance of hydrogen ions, bicarbonate, and carbon dioxide. It is managed naturally by the body’s chemical buffer systems, the lungs (excreting CO_2), and the kidneys (excreting hydrogen ions and reabsorbing bicarbonate). Because Nattokinase and Serrapeptase digest proteins rather than balancing electrolytes or altering hydrogen ion concentrations, they have no biochemical mechanism to impact or reverse acidosis.
2 Likes
Thanks for clarifying. You must be right as I assumed they go together. All I know is that if I dared to drink my morning coffee the burning in my chest would be so bad I’d think there’s a fire inside me, and then I started with Nattokinase and Serrapeptase and was totally gone. I now have 2-3 coffees each morning and no sign of acid reflux or burning.
1 Like
A cardiologist eats 90 grams of fiber a day without trying. Here’s her breakfast, lunch, and dinner.
2 Likes
1 Like
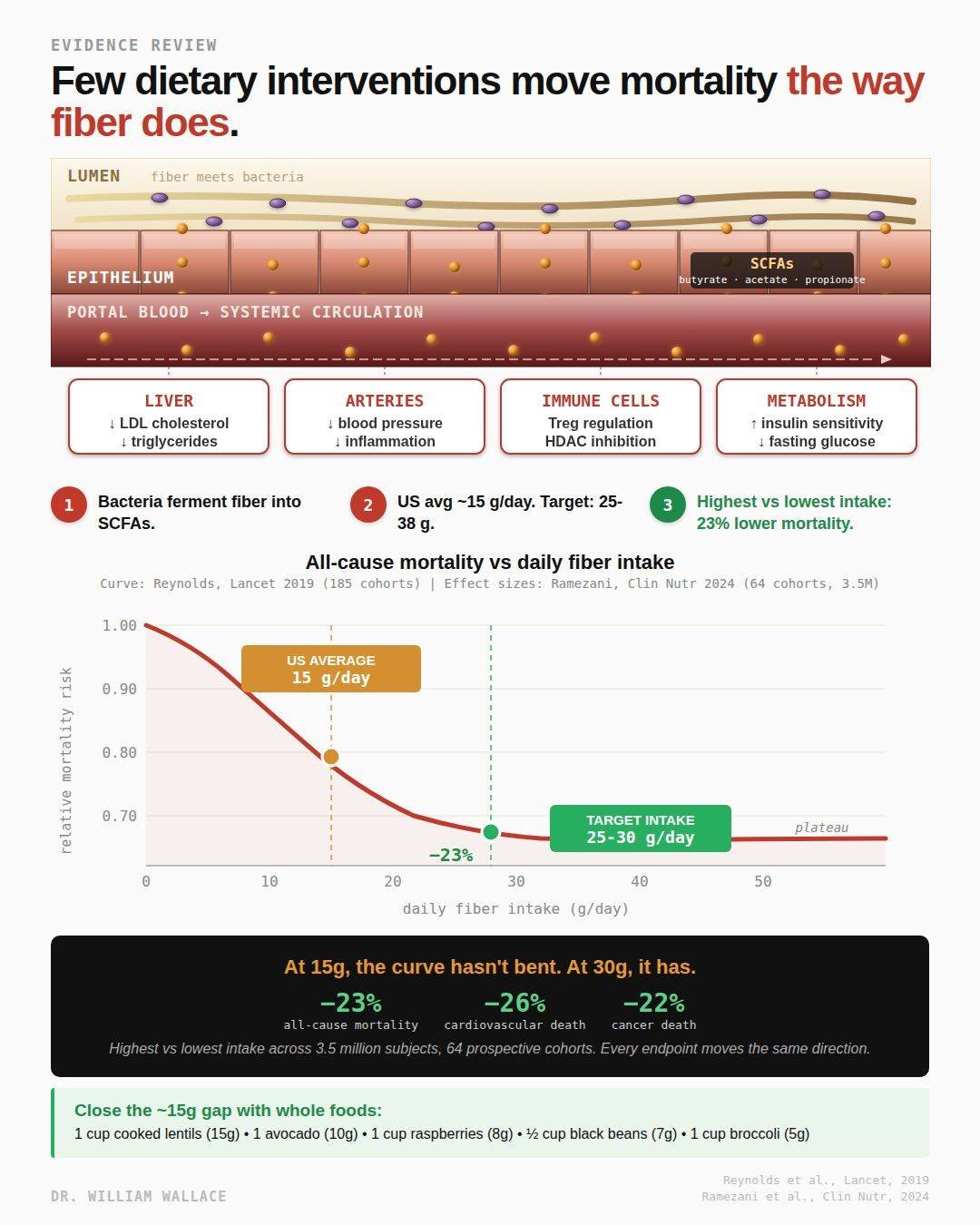
Fiber gets treated as nutrition advice and rarely as a mortality intervention. The meta-analysis data suggests it should be both.
The 2024 Ramezani systematic review in Clinical Nutrition pooled 64 prospective cohorts totaling 3.5 million subjects. Comparing the highest fiber consumers to the lowest, all-cause mortality was 23% lower. Cardiovascular mortality was 26% lower. Cancer mortality was 22% lower. Every endpoint measured moved in the same direction. Effect sizes of this magnitude from observational data on a single nutrient are rare.
The 2019 Reynolds Lancet meta-analysis fills in the dose-response shape. Pooling 185 prospective cohorts, mortality risk drops sharply from near-zero intake up to about 25 grams per day and then plateaus. Below 25 grams, each additional gram is associated with measurable risk reduction. Above 30 grams, the curve is mostly flat. The inflection point sits almost exactly where the Institute of Medicine set the daily target, which is 25 grams for women and 38 grams for men.
US adults average around 15 grams per day. That is roughly halfway up the risk curve, not at the top.Published intake surveys suggest about 95% of American adults fail to hit even the low end of the target range. Closing that gap is arguably the single largest preventable nutrition-related mortality signal in the current evidence base.
The mechanism connects the colon to systemic physiology, but the specific pathways matter. Fiber escapes digestion in the small intestine and reaches the colon intact. Some of that effect is direct. Viscous soluble fibers like beta-glucan from oats and psyllium bind bile acids in the intestinal lumen and increase their fecal excretion, which forces the liver to pull more cholesterol out of circulation to synthesize replacement bile acids. This is how fiber lowers LDL, and it happens without bacteria needing to be involved.
The other layer is fermentation. Resident bacteria in the colon ferment carbohydrate-rich fibers into short-chain fatty acids, primarily acetate, propionate, and butyrate. These molecules cross the epithelial barrier into the bloodstream. Propionate reaches the liver and appears to inhibit cholesterol synthesis, adding a second mechanism behind fiber’s lipid effects. Butyrate regulates gene expression in immune cells, supports regulatory T cell populations, and serves as the main energy substrate for the cells lining the colon. SCFAs also signal through receptors on immune cells, enteroendocrine cells, and fat cells, influencing insulin sensitivity and inflammation.
Several caveats are worth flagging. The mortality evidence is observational, not randomized, so residual confounding is real. Fiber intake correlates with overall diet quality, physical activity, body weight, smoking status, and socioeconomic factors, all of which independently affect mortality. The Ramezani and Reynolds meta-analyses adjusted for major confounders, but causal claims require more caution than the raw numbers suggest. Randomized fiber-intervention trials on hard mortality endpoints do not exist at this scale and likely never will due to cost and duration. What the evidence does support strongly is that higher fiber intake is associated with lower mortality, the relationship is graded by dose, and the associations are consistent across dozens of independent cohorts and mechanistically plausible.
One subgroup finding worth knowing. In the Ramezani analysis, insoluble fiber showed stronger mortality associations than soluble fiber, and fiber from nuts and seeds specifically was associated with 43% lower cardiovascular mortality. The mortality signal is strongest for whole food fiber from diverse sources, not for single-source supplements or powders.
Practically, closing a 10 to 15 gram per day gap is achievable with basic food swaps. One cup of cooked lentils contributes about 15 grams. One avocado is about 10 grams. A cup of raspberries is about 8 grams. A half cup of black beans is about 7 grams. A cup of broccoli is about 5 grams. Most adults can move from 15 to 30 grams per day by adding one serving each of a legume, a whole grain, and a fibrous vegetable.
For the magnitude of mortality associations backed by this scale of observational evidence, few single nutrients compare. The gap between what the data points to and what most Americans eat is unusually wide.
Sources:
Ramezani F, et al. Clin Nutr. 2024;43(1):65-83.
Reynolds A, et al. Lancet. 2019;393(10170):434-445.
Source: https://x.com/WilliamWallace/status/2057207626740511027?s=20
9 Likes
I have been taking C Butyricum probiotic for over a decade to grow my own butyric acid. Brand is Miyarisan. I discovered it after my doc ordered a stool test and found I had low butyric acid. The product she suggested tasted like vomit and I decided I would rather take the probiotic then take vomit.
Here is a post from a chronic fatigue syndrome patient page with many references about C Butyricum.
There are also some Asian papers I read many years ago about it being efficacious with c diff infection.
2 Likes
Thanks for sharing this study on the importance of dietary fiber. The reason dietary fiber is important is because it is “food” for the beneficial bacteria in your gut microbiome. The bacteria ferment dietary fibers (and polyphenols) which results in the production of postbiotic metabolites.
Read my papers on this topic:
-
Postbiotic Metabolites: The New Frontier in Microbiome Science https://townsendletter.com/postbiotic-metabolites-pelton/
-
THE MICROBIOME THEORY OF AGING: The Microbiome Theory of Aging (MTA) - PMC
ALSO…here is a link for a FREE copy of a booklet I wrote titled DR. OHHIRA’S PROBIOTICS & POSTBIOTIC METABOLITES: Probiotics & Postbiotic Metabolites | Ross Pelton | The Natural Pharmacist
Healthy regards, Ross
2 Likes
Modeling the microbial contribution to human energy balance using the Digestion, Absorption, and Microbial Metabolism (DAMM) model
Pop-sci:
Have We Gotten Calories Wrong All This Time? Study Challenges 130 Years Of Nutrition Science
1 Like
Dr. Carvalho weighs in.
8 Foods That Men & Women NEED To Heal Your Gut (via Nutrition Made Simple!)

1 Like
I. Executive Summary
The core thesis of this video outlines a pragmatic, evidence-based, food-first framework for optimizing human gastrointestinal health while systematically dismissing high-cost commercial fads like “detoxes,” “cleanses,” and unstandardized probiotic supplements. The metabolic argument pivots on a dual mechanism: introducing live symbiotic microorganisms through specific fermented foods, and systematically nourishing these populations with precise prebiotic substrates, namely viscous fibers and resistant starches. This symbiotic paradigm modulates the gut microbiome, expanding alpha diversity and generating functional downstream metabolites—primarily short-chain fatty acids (SCFAs) like butyrate—that fuel colonocytes, preserve tight junction barrier integrity, and optimize systemic metabolic metrics including insulin sensitivity, atherogenic lipid profiles, and blood pressure.
Clinical and lifestyle translation requires precise individual customization based on baseline gastrointestinal pathology. For instance, viscous fibers and sorbitol-rich whole foods act as osmotic laxatives or fecal bulk-forming agents, providing definitive efficacy for functional constipation but posing potential tolerability risks for diarrhea-predominant irritable bowel syndrome (IBS-D). Furthermore, the absolute efficacy of any gut-health protocol depends entirely on the kinetic rate of its introduction. Shifting rapidly from a low-fiber Western diet to high-prebiotic intake routinely causes acute dysbiosis, gas, and abdominal bloating, mimicking pathological intolerance when it is merely a transient physiological adaptation lag.
Ultimately, the optimal strategy for long-term microbiome resilience requires dietary diversity over massive singular volume. This involves a deliberate rotation of varied viscous fibers, multi-type resistant starches, and structural polyphenols to fill distinct ecological niches within the gut. To achieve this, consumers must actively screen out commercial pitfalls, such as post-fermentation sugar additions in commercial kefirs and kombuchas or the glycemic structural modifications found in finely processed instant oats. Whole, minimally processed, cost-effective foods provide a clinically superior safety and efficacy profile compared to synthetic alternatives.
II. Insight Bullets
- Prunes as Osmotic Laxatives: Prunes contain sorbitol, a sugar alcohol that draws water into the intestinal lumen via an osmotic gradient, softing stool and improving evacuation mechanics.
- Clinical Superiority of Prunes over Psyllium: Randomized crossover trial data show that 100g of prunes daily provides superior improvements in complete spontaneous bowel movements and stool consistency compared to psyllium husk (Attaluri et al., 2011).
- Caloric Trade-offs of Dried Fruit: A standard 80–100g therapeutic dose of prunes yields approximately 200 kcal, necessitating its use as a replacement for existing snacks rather than an additive to prevent positive energy balance.
- Contraindications in IBS-D: Due to their water-pulling osmotic properties, sorbitol-dense foods like prunes accelerate transit times and are clinically contraindicated for individuals presenting with diarrhea-predominant irritable bowel syndrome (IBS-D).
- Fermented Foods Drive Microbiome Diversity: Controlled feeding trials demonstrate that consistent intake of fermented foods dramatically expands gut microbiome alpha diversity and suppresses 19 distinct serum inflammatory markers, including interleukin-6 (Wastyk et al., 2021).
- Kefir Efficacy Profiles vs. Yogurt: Kefir exhibits a more diverse, complex consortium of lactic acid bacteria and yeasts than standard yogurt, providing superior probiotic delivery, higher antioxidant density, and improved glycemic control in diabetic cohorts (Ostadrahimi et al., 2015).
- Commercial Post-Fermentation Sugar Pitfalls: Many commercially distributed fermented milks and kombuchas introduce substantial amounts of sucrose or high-fructose corn syrup post-fermentation to mask tartness, which counteracts metabolic benefits.
- The Symbiotic Requirement of Prebiotics: Exogenous probiotics delivered via fermented foods will fail to colonize or exert sustained biological activity unless accompanied by adequate prebiotic substrates to fuel their metabolic survival.
- Viscous Fiber and Gelling Mechanics: Soluble viscous fibers (such as beta-glucans) interact with water to establish a highly structured gel matrix inside the gut, which delays gastric emptying, improves satiety, and downregulates systemic cholesterol levels (Whitehead et al., 2014).
- Whole Oats vs. Processing Alterations: Whole rolled or steel-cut oats retain their complex carbohydrate architecture and lower HbA1c and fasting insulin in metabolic disorders, whereas finely chopped instant oats frequently introduce glycemic spikes and added sugars (Hou et al., 2016).
- Polyphenol-Microbiome Symbiosis in Berries: Berries provide concentrated doses of structural polyphenols that escape small intestinal digestion to selectively enrich Bifidobacterium and Lactobacillus strains in the colon.
- The Payback System of Short-Chain Fatty Acids: Microbial fermentation of viscous fiber yields short-chain fatty acids (primarily butyrate), which directly fuel colonocyte metabolism, enhance tight junction barrier function, and upregulate insulin sensitivity.
- Resistant Starch Heterogeneity: Resistant starches bypass standard enzymatic cleavage in the small intestine; different structural types (e.g., Type 1 in lentils vs. Type 2 in green bananas) induce distinct physiological and microbial shifts.
- Lentils as Metabolic Enhancers: Pulses deliver cost-effective resistant starch and fiber combinations that consistently drive down clinical markers of insulin resistance, systemic inflammation, and circulating LDL-C.
- The Ramp-Up Adaptability Curve: The gastrointestinal tract requires a progressive step-wise escalation of prebiotic fibers; sudden transitions from low to high fiber precipitate severe bloating, mimicking a true food allergy or structural intolerance.
- Nutritional Viability of Ultra-Processed Alternatives: Structural processing is not uniformly toxic; high-fiber alternatives like lentil pasta or BPA-free/salt-free canned pulses preserve the core prebiotic metrics while lowering lifestyle friction.
- Walnut-Driven Microbiome Up-Regulation: Consuming 1.5 ounces (~43g) of walnuts daily significantly alters intestinal beta-diversity, augmenting the abundance of Ruminococcaceae and Bifidobacteria while dropping serum cholesterol (Holscher et al., 2018).
- Kiwifruit for Gastrointestinal Motility: Clinical trial data reveal that consuming two gold or green kiwifruits daily achieves therapeutic improvements in bowel movement frequency and decreases straining equivalent to psyllium husk without causing adverse flatulence (Gearry et al., 2023).
- Kombucha Hype Filtering: While kombucha serves as a viable, low-calorie alternative to sugary sodas, internet claims asserting it can cure cancer or reverse chronic systemic diseases are completely unbacked by human clinical data.
- Microbiome Resilience Requires Diversity: True gastrointestinal health is a function of ecological diversity driven by a multi-component diet rather than isolated, hyper-dosed “superfoods” or proprietary capsule formulations.
IV. Actionable Protocol (Prioritized)
High Confidence Tier (Backed by Level A/B Evidence)
- Constipation Mitigation via Whole Foods: To treat mild-to-moderate functional constipation or sluggish motility, ingest either two whole green/gold kiwifruits daily or 50–100g of prunes daily. These food-based protocols are clinically verified to match or exceed the efficacy of 7.5–11g of psyllium husk (Attaluri et al., 2011; Gearry et al., 2023).
- Microbiome Alpha Diversity Expansion: Consume 3 to 6 servings daily of low-sodium, zero-sugar-added fermented foods, prioritizing traditional dairy or plant-based kefir and unsweetened plain yogurt. This protocol is validated to systematically scale up microbial diversity lines while downregulating 19 circulating inflammatory biomarkers (Wastyk et al., 2021).
- Lipid and Glycemic Modulation via Viscous Beta-Glucans: Incorporate 3g or more of oat beta-glucan daily, derived strictly from whole rolled or steel-cut oats (approximately 60–80g dry weight). This intake levels down total cholesterol, reduces LDL-C by an average of 0.30 mmol/L, and improves HbA1c and fasting insulin sensitivity parameters (Whitehead et al., 2014; Hou et al., 2016).
- Targeted SCFA Up-Regulation via Lipids: Ingest 1.5 ounces (~43g) of whole raw walnuts daily. This dosage alters intestinal beta-diversity, selectively enriches butyrate-producing Ruminococcaceae, and decreases atherogenic secondary bile acids like deoxycholic acid (Holscher et al., 2018).
Experimental Tier (Backed by Level C/D Evidence with High Safety Margins)
- Mixed Polyphenol Integration: Incorporate 1 cup of diverse, unheated frozen berries (blueberries, blackberries, raspberries) daily into morning feeding windows. This provides a concentrated matrix of structural polyphenols that escape small bowel assimilation to enrich Bifidobacterium and Lactobacillus populations.
- Multi-Type Resistant Starch Rotation: Integrate 1/2 cup of prepared whole pulses (lentils, chickpeas, or black beans) or 100% lentil-derived pasta daily. Rotate these sources to capture distinct resistant starch categories (Type 1 through Type 4), which optimize diverse microbial fermentation cascades along the length of the colon.
Red Flag Zone (Claims Debunked or Lacking Safety Data)
- Commercial Unstandardized Probiotics & Cleanses (Safety Data Absent / Clinically Unverified): Avoid high-cost over-the-counter probiotic pills, gut cleanses, or detox regimens. These formulations lack a supportive food-derived prebiotic matrix and display volatile, highly unpredictable colonization dynamics compared to real fermented foods.
- High-Sugar Commercial Fermented Vehicles (High Translational Gap): Reject commercial kefirs, yogurts, and kombuchas that list added sugars post-fermentation. The introduction of refined sucrose or high-fructose corn syrup offsets the systemic metabolic benefits of the underlying probiotic strains.
- Rapid-Onset High-Fiber Loading (High Safety/Tolerability Risk): Never transition abruptly from a low-fiber Western diet to high-dose prebiotic protocols. Sudden intake escalations induce severe flatulence, abdominal distension, and microbial distress. Scale up fiber and pulse intake gradually (e.g., by 1–2 tablespoons per week) to give the gut ecosystem time to adapt.
4 Likes
Dr. Vinay Prasad takes a critical look at fiber. He’s not impressed.
Episode 3 - Fiber - How much do you ‘Need’? (via Vinay Prasad MD MPH)

I. Executive Summary
Dietary fiber is widely promoted as a core component of longevity medicine, yet the epidemiological foundations supporting specific target metrics (such as 30–35 grams per day) are fundamentally compromised by healthy-user bias and systematic misinterpretation of genetic data. This analysis deconstructs a pivotal 2025 National Health and Nutrition Examination Survey (NHANES) and Mendelian Randomization (MR) study published in the journal Stroke (Lai et al., 2025), demonstrating how observational cohorts suffer from unmitigated residual confounding. Individuals consuming high-fiber diets inherently present with lower body mass index (BMI), lower baseline rates of hypertension, higher educational attainment, increased marital stability, and reduced smoking rates. These variables reflect broad health-seeking behaviors rather than isolated fiber mechanics.
Furthermore, while the study’s MR analysis—designed to use genetic variants as instrumental variables to establish causality—returned almost universally null findings across multiple stroke subtypes (including ischemic, lacunar, large artery, and cardioembolic stroke), the authors highlighted a solitary, nominally significant association with small vessel stroke (OR 0.8326, p=0.0309) in their abstract. This represents a clear instance of abstract spin that overstates protective effects and obscures the true null nature of the aggregate genetic data.
Clinically, fiber forms are highly heterogeneous. Viscous, gel-forming soluble fibers such as psyllium husk demonstrate robust Level A/B evidence in randomized controlled trials (RCTs) for improving surrogate biomarkers, including fasting blood glucose and low-density lipoprotein cholesterol (LDL-C). Conversely, non-gel-forming or insoluble fibers like wheat bran, wheat dextrin, and inulin lack these specific metabolic advantages. Crucially, no prospective RCT directly links high fiber intake to extended maximum lifespan or reduced all-cause mortality in healthy cohorts.
Therefore, fiber functions purely as an intervention to prevent premature or untimely death (such as mid-life cardiovascular events) rather than a true longevity-extension therapeutic that shifts the upper limits of human survival. The primary knowledge gap resides not in prospective epidemiology, which remains saturated, but in behavioral adherence data exploring how healthy subjects tolerate and maintain high-fiber regimens over multi-year intervals.
II. Insight Bullets
- Epidemiological Consensus vs. Data Rigor: Longevity texts and nutritional guidelines universally mandate high fiber intake, yet the empirical data underlying specific volume metrics remain highly vulnerable to methodological limitations.
- Fiber Heterogeneity: Fiber cannot be treated as a single uniform macronutrient; its biological action depends entirely on physicochemical traits such as solubility, viscosity, and fermentation rate.
- Mechanistic Efficacy of Gel-Forming Fiber: Psyllium husk forms a viscous gel in the gut that delays gastric emptying and slows macronutrient absorption, providing distinct metabolic advantages.
- Surrogate Marker Modification: Level A meta-analyses confirm that psyllium significantly reduces fasting blood glucose, HbA1c, and LDL-C, with benefits scaling proportionally to the patient’s baseline metabolic dysfunction (McRorie et al., 2015).
- Inefficacy of Non-Viscous Variants: Insoluble or non-viscous fibers, such as wheat bran, wheat dextrin, and inulin, fail to replicate the glycemic or lipid-lowering efficacy seen with gel-forming soluble options in RCTs.
- The Food vs. Supplement Black Box: There is a profound lack of head-to-head clinical data evaluating whether isolated fiber supplements deliver identical physiological outcomes to fiber consumed within intact, plant-based food matrices.
- Healthy-User Bias in Cohorts: Observational data from food frequency questionnaires (such as NHANES) are deeply confounded by the baseline characteristics of individuals who choose to eat high-fiber diets.
- Confounder Clustering: High-fiber consumers display lower BMIs, lower baseline hypertension, higher education levels, higher rates of marriage/cohabitation, and lower smoking rates, rendering isolated causal attribution nearly impossible.
- Residual Confounding Inevitability: Statistical adjustments in cohort studies are crude and can only account for measured variables, ensuring that persistent unmeasured healthy-user bias artificially inflates fiber’s apparent benefits.
- Extrapolation Errors in Spline Modeling: Epidemiological models plotting continuous risk reductions up to extreme fiber intakes (such as 50–100g/day) rely on highly volatile, sparse data from very few subjects, overstating prospective safety and efficacy.
- Mendelian Randomization Disconnect: Mendelian Randomization (MR) utilizes single nucleotide polymorphisms (SNPs) as instrumental variables to bypass environmental confounding, yet its application to dietary habits remains highly speculative.
- The Stroke Paper Flaw: A 2025 study in Stroke utilized MR to find a causal path between fiber and stroke, but the actual genomic data showed stone-cold null results across almost all major stroke classifications (Lai et al., 2025).
- Abstract Spin and Selective Reporting: Despite broad null results in the MR table (p-values ranging from 0.08 to 0.96), the authors extracted a solitary positive signal for small vessel stroke to declare a causal relationship in the abstract.
- Error Propagation: The distortion of data within journal abstracts creates a cascade of misinformation that transfers directly into consumer health books, media reports, and public health policy without verification of the fine print.
- The “Untimely Death” vs. “Longevity” Distinction: Fiber should be categorized strictly as an intervention to prevent untimely death from premature cardiovascular pathology, not as an intervention that modulates core biological aging pathways to extend maximum lifespan.
- Absence of Hard Hardpoint Data: No long-term randomized controlled trials exist demonstrating that supplemental fiber improves all-cause mortality or hard longevity metrics in healthy populations.
- The Adherence Knowledge Gap: There is an absolute paucity of clinical data tracking long-term adherence rates, tolerance, and gastrointestinal side effects (such as bloating and gas) of high-dose fiber protocols in healthy cohorts.
- Misallocation of Research Funding: Continued funding of passive observational dietary surveys is a waste of federal resources; funds should be redirected toward randomized behavioral trials assessing long-term dietary adherence frameworks.
IV. Actionable Protocol (Prioritized)
High Confidence Tier (Level A/B Evidence)
- Targeted Psyllium Supplementation: To optimize lipid profiles and short-term glycemic control, administer a median dose of approximately 10.2 grams per day of soluble, viscous, gel-forming psyllium husk fiber directly before major meals (Jovanovski et al., 2018). This is clinically proven to lower LDL-C, non-HDL-C, and ApoB, with the magnitude of benefit scaling to the degree of baseline insulin resistance or dyslipidemia.
- Intact Whole-Food Integration: Prioritize obtaining baseline fiber from whole plant matrices (such as cruciferous vegetables, nuts, and legumes) rather than isolated texturized additives. Whole foods slow macronutrient absorption, modulate postprandial glucose spikes, and promote satiety via stretch-receptor activation in the stomach.
Experimental Tier (Level C/D Evidence)
- Microbiome Modulation via Fermentable Prebiotics: The use of inulin, wheat dextrin, or synthetic prebiotic fibers to selectively upregulate short-chain fatty acid (SCFA) production (such as acetate and butyrate) remains experimental. While safety margins are high, clear translation into hard cardiovascular or metabolic endpoints in healthy humans is unproven.
- Aggressive Titration for Weight Management: Gradually increasing fiber intake from the standard American baseline of 14 grams per day up to the professional target of 30–35 grams per day may serve as a mechanical adjuvant for weight loss due to induced satiety. However, long-term human adherence data are absent.
Red Flag Zone (Claims Debunked or Lacking Safety Data)
- Non-Viscous Fiber Substitutions: Avoid substituting wheat bran, wheat dextrin, or inulin with the expectation of achieving direct acute improvements in fasting blood glucose or LDL-C clearance. RCT data demonstrate that non-gel-forming fibers lack these physical absorption-delaying capabilities.
- Autonomous Stroke Prevention Claims: Do not rely on high-fiber diets as an autonomous or primary therapeutic vector to lower stroke risk. Assertions of an aggressive, direct causal reduction in overall stroke incidence are contradicted by the null findings of objective genetic Mendelian Randomization data.
- Lifespan Extension Speculation: Treat claims that fiber supplementation directly modulates intrinsic mammalian biological aging rates or extends maximum lifespan as unverified. Hard clinical data linking fiber ingestion to maximum lifespan extension are completely absent.
1 Like
He’s fun to listen to. I like his attitude. I’ve been fiber maxing and taking miyarisan. Good thing I’m a farmer because the gas is ridiculous. I thought the benefit would be immunity. Never even thought about stroke. I don’t want a stroke, I’ve seen it done and it’s not pretty.
2 Likes