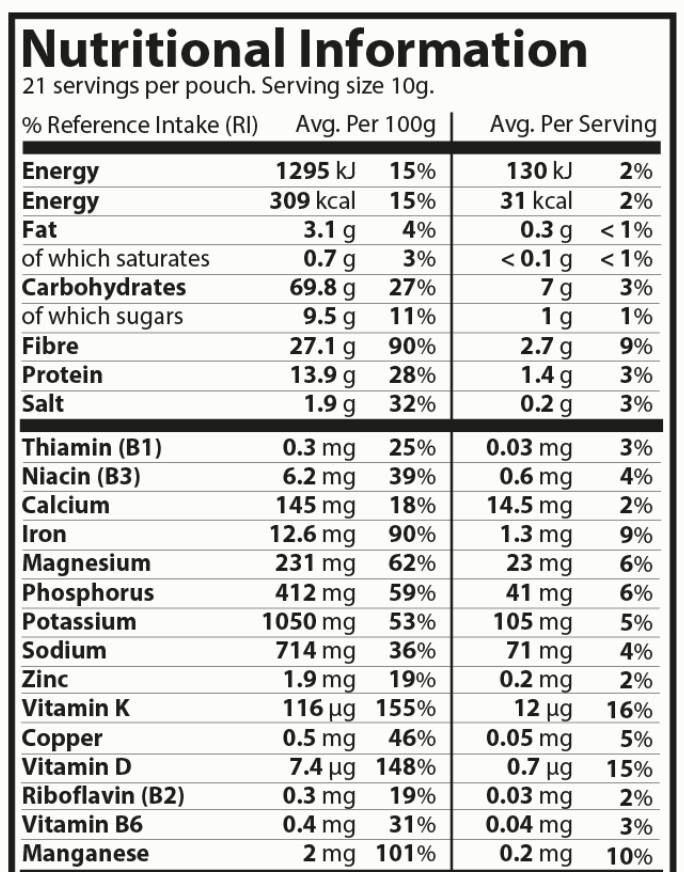
The synbiotic arm were given 170 ml kefir and 10 g of a prebiotic mix (supplied by Chucking Goat Ltd), consumed as a smoothie daily for 6 weeks.
Note that the composition below is for 100g but the serving size is 10g so it provides only 2.71g of fiber for 6.98g of carbs and 0.95g of sugar.
Not really impressive. I’m taking fiber and EPA and kefir (>250ml of my home made fresh kefir).
Butyrate: The Microbiome’s Anti-Aging “Kill Switch” for Senescent Cell
I was never able to find a BHB supplement that I liked. So I have chosen to take C8 (caprylic acid) in my morning coffee Actually use a combo of C8 and C10 for immediate and sustained benefits. It actually tastes good in my coffee. I use the powdered form, and it tastes a lot like adding a creamer to my coffee.
Of course: “ketone esters provided the largest BHB ketone boost per serving.”
Summary of Differences
Feature
C8 Supplementation
Direct BHB Supplementation
Action
Precursor; body produces BHB from C8
Direct source of BHB
Speed
Slower to raise BHB levels (peak around 60-120 min)
Rapid BHB surge (peak around 30-60 min)
Effect Duration
More sustained elevation
Quicker return to baseline
Goal
Supports long-term fat adaptation and endogenous ketone production
Provides immediate exog
Mostly at my age I look for supplements that have benefits for the brain:
C8 (caprylic acid) supplementation primarily benefits the brain by providing an alternative and rapid fuel source in the form of ketones and through direct neuroprotective effects, including enhanced mitochondrial function and potential anti-inflammatory action.
Key Brain Benefits
Alternative Energy Source: The brain primarily uses glucose for energy. However, in certain conditions like Alzheimer’s disease or with aging, the brain may develop insulin resistance and lose the ability to use glucose efficiently, creating an “energy gap”. C8 is quickly metabolized into ketone bodies (specifically BHB) in the liver, which can readily cross the blood-brain barrier and provide an alternative, highly efficient fuel source to brain cells, thereby bridging this energy gap.
Improved Cognitive Function: Studies have shown that C8 supplementation can enhance mental clarity, focus, memory, and overall cognitive performance, both in healthy young adults and in elderly individuals with mild cognitive impairment (MCI) or Alzheimer’s disease (AD).
Neuroprotective Effects: C8 and its metabolites may offer neuroprotection by:
Increasing Neuronal GABA Synthesis: C8 can increase the supply of glutamine to astrocytes, which is then used to synthesize the neurotransmitter GABA in neurons, potentially contributing to anti-seizure effects.
Modulating Inflammation: Low-level intake of caprylic acid may help reduce neuroinflammation and protect against neural degeneration.
Enhancing Mitochondrial Function: Some research suggests C8 can directly stimulate mitochondrial respiration (energy production) in brain cells.
Support for Neurological Conditions: The ketogenic effects of C8 have been used in the dietary management of drug-resistant epilepsy since the 1920s, helping to reduce seizure frequency. Research also suggests potential benefits in ameliorating other neurodegenerative disorders such as Parkinson’s disease and TBI by restoring energy metabolism.
Summary
C8 supplementation offers significant brain benefits by providing a rapid, alternative fuel and directly supporting neural health and function. These effects can lead to enhanced mental performance and may also help mitigate cognitive decline in individuals with conditions that impair brain glucose metabolism. Ref
OK, there were problems with this study. Here is some more from an analysis of the paper (see below) but it would seem that the idea of a complex of prebiotic fibers, and specific goat-milk kefir (27 strains) (how do you make this???), might have some value. Below I’ve done a search for other probiotic mixtures that might be similar to the one used in the study, but that are sold commercially in the USA.
4. Novelty
Magnitude of Effect: We already knew fermented foods were good (Wastyk et al., 2021). What is new is the effect size (d>1.0 for multiple markers) compared to the standard of care (Omega-3). Omega-3s failed to move the needle on IL-6 or SIRT2 in this comparison.
Specific Synbiotic Formulation: This wasn’t just “yogurt.” It was a specific goat-milk kefir (27 strains) paired with a complex 18-fiber prebiotic mix (arabinoxylan, beta-glucans, etc.). This supports the “precision prebiotic” hypothesis—you need the right fuel for the right bugs.
5. Critical Limitations
The Age Confound (Major): The study compares a younger Synbiotic cohort (18+) against an older Omega-3/Inulin cohort (60+). While the authors adjusted for age statistically, this is a dangerous comparison. Older adults have established immunosenescence and higher baseline inflammation. It is possible Omega-3s work better in younger people, or that the Synbiotic effect is exaggerated because younger systems are more plastic.
Non-Blinded: Participants knew they were drinking a smoothie. The placebo effect on subjective well-being is irrelevant for serum markers, but lifestyle confounding (e.g., “I’m drinking this healthy smoothie, maybe I shouldn’t eat pizza”) is a risk.
Short Duration: 6 weeks is sufficient for cytokine changes but insufficient to prove long-term remodeling of the immune system or colonization of the gut microbiome.
Low Dosage of Omega-3: The Omega-3 group received only 500mg/day (165mg EPA / 110mg DHA). This is a clinically low dose. Most therapeutic longevity protocols recommend 2g-4g daily. Comparing a “nuclear” synbiotic intervention to a “homeopathic” dose of Omega-3 is a straw-man comparison [Confidence: High].
Prebiotic Fiber Mixtures
Market search identified that no single pre-mixed powder contains all 18 specific isolated fibers, as many are structural subclasses of one another (e.g., Arabinan and Galactan are often substructures of Pectin or Arabinogalactan; Xyloglucan is a hemicellulose).
However, Designs for Health PaleoFiber and Vibrant Health Green Vibrance contain the highest density of these specific compounds due to their use of complex whole-plant and gum sources.
Top Ranked: Highest Ingredient Match
1. PaleoFiber (Powder)
Match Count:12/18 (Direct & Source-Derived)
Why it wins: This formula is designed as a “complex fiber” blend. It uses 12 distinct plant sources that naturally cover the structural hemicelluloses (Arabinoxylan, Xylan, Mannan) which are rarely found as isolated ingredients.
Ingredient Mapping:
Arabinogalactan: Native to Acacia Gum (primary ingredient).
Arabinoxylan:Psyllium Husk is ~70% highly branched arabinoxylan.
Cellulose:Bamboo Fiber is almost pure cellulose.
Guar Gum: Explicitly included (Hydrolyzed Guar).
Inulin:Chicory Root Inulin.
Mannan:Glucomannan (Konjac root) and Guar (Galactomannan).
Pectin:Apple Pectin.
Arabinan / Galactan: Abundant side-chains in Apple Pectin and Acacia.
Xylan: Major component of Bamboo Fiber.
Hemicellulose: Comprised of the Psyllium, Bamboo, and Flax fibers.
Note: They also offer “PaleoFiber RS” which swaps some fibers for Resistant Starch (Green Banana) but loses the diversity of the 12-fiber blend.
2. Green Vibrance
Match Count:11/18
Why it ranks high: While primarily a “Greens” powder, its fiber profile is chemically complex. It explicitly adds Larch Arabinogalactan, FOS, and Apple Pectin to a base of cereal grasses (Wheat/Oat/Barley) which are the industry’s primary sources of Arabinoxylan, Beta-Glucan, and Xylan.
Why it ranks high: It is one of the few products to explicitly isolate and list Xylooligosaccharide (XOS) and multiple forms of Beta-Glucan. It is a “precision” prebiotic rather than a “whole food” blend.
Ingredient Mapping:
XOS: Xylooligosaccharide (rarely found in blends).
Arabinogalactan: Explicitly listed.
Beta-Glucan: (1,3/1,6 from Yeast) AND (1,3/1,4 from Oat).
I’ve been on my “high-butyrate” diet for the past few months, and it seems to be working. This week’s blood test that included HS-CRP was at 0.3mg/L, so about as low as it goes (given the error bars of this test).
My butyrate program:
10 grams of inulin in my coffee right now (recently ran out of SunFiber)
NOW Foods Supplement, 8 Billion Acidophilus & Bifidus, 1 per day, 68 mg,
Curcumin Phytosome 500 mg (Meriva) - Sustained Release per day,
Natural Factors Oil of Oregano, Carvacrol 144mg per day
and occasionally (couple times a week) fermented tea (Japanese/chinese).
Tim, could you share the brands your are using? I’ve been dealing with acid reflux recently and would like to see if I see similar relief as you’ve described.
I am just parroting what we already know from various AIs. But what happened to Akkermansia?
“Metabolic Health: Ameliorating insulin sensitivity and lowering plasma total cholesterol.
Weight Management: Reductions in body weight, fat mass, and hip circumference have been observed in clinical studies.
Gut Barrier Integrity: Strengthening the mucus layer and preventing “leaky gut” by improving the gut’s physical barrier.”
FWIW: I have taken probiotics on and off over the years and did not notice any subjective change. Lately I have been putting my probiotics in enteric-coated capsules before taking them. The difference is dramatic. I notice a big change: normalization of my poop
I especially notice a normalization of my stomach and lower digestive tract.
Currently I am taking Lactobacillus brevis, but when I finish the bottle, I will go back to Akkermansia, which I have tried before with no subjective result. But at the time I was taking Akkermansia, I wasn’t putting it in enteric-coated capsules.
“Gut microbiome homeostasis is fundamental to brain health (cognitive function and synaptic plasticity) (Salami, 2021), preventing neuroinflammation and protecting against neurodegenerative disorders in the elderly by maintaining microglial cells in a healthy mature state”
“Diversity & Stability: A healthy gut typically has a high variety of different species that are resilient enough to bounce back after temporary disruptions like a round of antibiotics or a change in diet.”
I use tributyrin to reduce inflammation, not for acid reflux. To treat acid reflux combined with acidosis, I used to take 650-mg tablets of sodium bicarb for years. Recently, however, the sodium got to be too much and I switched to capsules of ginger. I take one 500-mg capsule three times a day with food. This works. It also obliterates inflammation.
Enteric caps are elusive to find . AI said it might be because true enteric implies “medical” as opposed to simple supplements. Sometimes on Amazon XPRS has enteric and also Leadlife. I tested both in vinegar and both brands preformed well. Enteric (Acid-Resistant) Clear Empty Gelatin Capsules — 1000 ct (Sizes 00-1)
This has some interesting content on the topic and product as well:
There seems to be many different products on the market containing Tributyrin with various other ingredients. I wonder if it would be more beneficial to alternate various products.
The Heart-Healthy Starch Paradox: When “Good” Carbs Fuel a Risky Cardiovascular Metabolite
Resistant starch is widely celebrated in biotech, healthcare, and longevity circles for its ability to blunt insulin spikes and feed the colonic microbiome. However, a meticulously controlled dietary trial challenges this universally positive narrative, revealing that high intake of resistant starch can significantly elevate trimethylamine-N-oxide (TMAO), a gut-derived metabolite tightly linked to cardiovascular disease risk.
Conducted by researchers across several US institutions, including the Children’s Hospital Oakland Research Institute and Lawrence Berkeley National Laboratory, this trial investigated how diets varying in resistant starch and total carbohydrate content affect postprandial glucose and TMAO levels. The research was published in the British Journal of Nutrition. The impact score of this journal is 3.0, evaluated against a typical high-end range of 0–15 for top nutrition science journals, therefore this is a Medium impact journal.
In a rigorously controlled cross-over trial, 52 healthy men and women were assigned to lower-carbohydrate (39-40% of energy) or higher-carbohydrate (51-53% of energy) dietary arms. Within these arms, participants consumed 2-week diets that were either high or low in resistant starch, separated by a 2-week washout. The findings present a striking metabolic trade-off. As expected, the high-resistant-starch meals successfully reduced postprandial insulin and glucose responses, demonstrating clear utility for meal-to-meal glycemic control. However, in the lower-carbohydrate context, the high-resistant-starch diet unexpectedly increased fasting plasma levels of TMAO and its precursors, including carnitine and betaine. When overall carbohydrate intake was high, TMAO levels were uniformly elevated regardless of starch digestibility, suggesting that baseline carbohydrate load dictates microbial fermentation pathways. Crucially, the short-term resistant starch intervention failed to improve fasting lipids, lipoproteins, or baseline insulin sensitivity.
This study complicates the established consensus on resistant starch. It suggests that while swapping digestible carbohydrates for resistant starch improves immediate glycemic markers, it simultaneously shifts colonic microbial fermentation in a way that ramps up pro-atherogenic TMAO production. For longevity specialists prioritizing actionable insights, this highlights a critical biological reality: single-variable nutritional interventions often produce competing multi-system trade-offs, pitting cardiovascular and metabolic pathways against one another.
Design: Participants acted as their own controls across 2-week high-resistant-starch and low-resistant-starch periods, nested within higher-carbohydrate or lower-carbohydrate arms.
Mechanistic Deep Dive
Gut Microbiome & TMAO Production: TMAO generation requires gut microbes to convert dietary precursors (like choline and carnitine) into trimethylamine, which the liver oxidizes into TMAO via flavin monooxygenases. High resistant starch intake fundamentally alters the colonic microbial community. The resulting shift appears to enhance the microbiome’s capacity to synthesize trimethylamine, even without increasing the dietary intake of carnitine or choline.
Metabolic vs. Cardiovascular Trade-offs: The data highlight a divergence in organ-specific health priorities. The high-resistant-starch intervention improved metabolic readouts by blunting incremental area under the curve (IAUC) for 0.5-hour glucose and 1-hour insulin responses. Yet, it concurrently increased plasma TMAO. Elevated TMAO is mechanistically linked in the literature to macrophage foam cell formation, vulnerable plaque development, and platelet hyperactivity.
Carbohydrate Dependency: The TMAO-raising effect of resistant starch was only significant when overall carbohydrate intake was restricted to 39-40% of total energy. Above 50% carbohydrate intake, TMAO generation was maximized independently of resistant starch content, suggesting a threshold effect for carbohydrate-driven microbial fermentation.
Novelty
Prior to this, resistant starch was almost exclusively viewed as cardioprotective due to short-chain fatty acid (SCFA) generation. This paper is among the first to empirically demonstrate that high resistant starch actually increases circulating TMAO levels [Confidence: High].
It introduces a previously unrecognized macronutrient interaction, proving that total dietary carbohydrate load dictates the microbiome’s TMAO-producing response to resistant starch [Confidence: High].
Critical Limitations
Short Duration: The 2-week intervention periods are biologically brief. It is entirely unknown if the gut microbiome or hepatic flavin monooxygenase 3 (FMO3) adapts to resistant starch over months, which could theoretically normalize TMAO levels [Confidence: Medium].
Translational Uncertainty: The study measures TMAO solely as a proxy biomarker. We lack hard endpoint data verifying whether this diet-induced TMAO spike actually accelerates atherosclerosis, or if the concurrent insulin-sensitizing benefits outcompete the cardiovascular risk in vivo [Confidence: High].
Food Processing Confounders: Starch retrogradation during the mandatory freezing and reheating of study meals may have altered starch digestibility, potentially muting the true metabolic divergence between the high- and low-resistant-starch diets [Confidence: Medium].
Missing Data: The paper lacks longitudinal tracking of endothelial function (e.g., flow-mediated dilation) or inflammatory cytokines to contextualize the physiological impact of the TMAO elevation.