Tim, could you share the brands your are using? I’ve been dealing with acid reflux recently and would like to see if I see similar relief as you’ve described.
1 Like
John, could you elaborate on citrate and acid reflux? Is there any research or protocol you can point to?
2 Likes
I am just parroting what we already know from various AIs. But what happened to Akkermansia?
“Metabolic Health: Ameliorating insulin sensitivity and lowering plasma total cholesterol.
Weight Management: Reductions in body weight, fat mass, and hip circumference have been observed in clinical studies.
Gut Barrier Integrity: Strengthening the mucus layer and preventing “leaky gut” by improving the gut’s physical barrier.”
FWIW: I have taken probiotics on and off over the years and did not notice any subjective change. Lately I have been putting my probiotics in enteric-coated capsules before taking them. The difference is dramatic. I notice a big change: normalization of my poop
I especially notice a normalization of my stomach and lower digestive tract.
Currently I am taking Lactobacillus brevis, but when I finish the bottle, I will go back to Akkermansia, which I have tried before with no subjective result. But at the time I was taking Akkermansia, I wasn’t putting it in enteric-coated capsules.
“Gut microbiome homeostasis is fundamental to brain health (cognitive function and synaptic plasticity) (Salami, 2021), preventing neuroinflammation and protecting against neurodegenerative disorders in the elderly by maintaining microglial cells in a healthy mature state”
“Diversity & Stability: A healthy gut typically has a high variety of different species that are resilient enough to bounce back after temporary disruptions like a round of antibiotics or a change in diet.”
3 Likes
Where do you order enteric-coated capsules?
I searched before (a couple of years back) with no success.
1 Like
I use tributyrin to reduce inflammation, not for acid reflux. To treat acid reflux combined with acidosis, I used to take 650-mg tablets of sodium bicarb for years. Recently, however, the sodium got to be too much and I switched to capsules of ginger. I take one 500-mg capsule three times a day with food. This works. It also obliterates inflammation.
3 Likes
Yes, John Hemming, you often post about citrate. What do you get out of it and what is a good starting dose?
1 Like
Enteric caps are elusive to find . AI said it might be because true enteric implies “medical” as opposed to simple supplements. Sometimes on Amazon XPRS has enteric and also Leadlife. I tested both in vinegar and both brands preformed well. Enteric (Acid-Resistant) Clear Empty Gelatin Capsules — 1000 ct (Sizes 00-1)
2 Likes
This has some interesting content on the topic and product as well:
There seems to be many different products on the market containing Tributyrin with various other ingredients. I wonder if it would be more beneficial to alternate various products.
2 Likes
Here’s a paper about how resistant starch is linked to increased TMAO in plasma:
2 Likes
The Heart-Healthy Starch Paradox: When “Good” Carbs Fuel a Risky Cardiovascular Metabolite
Resistant starch is widely celebrated in biotech, healthcare, and longevity circles for its ability to blunt insulin spikes and feed the colonic microbiome. However, a meticulously controlled dietary trial challenges this universally positive narrative, revealing that high intake of resistant starch can significantly elevate trimethylamine-N-oxide (TMAO), a gut-derived metabolite tightly linked to cardiovascular disease risk.
Conducted by researchers across several US institutions, including the Children’s Hospital Oakland Research Institute and Lawrence Berkeley National Laboratory, this trial investigated how diets varying in resistant starch and total carbohydrate content affect postprandial glucose and TMAO levels. The research was published in the British Journal of Nutrition. The impact score of this journal is 3.0, evaluated against a typical high-end range of 0–15 for top nutrition science journals, therefore this is a Medium impact journal.
In a rigorously controlled cross-over trial, 52 healthy men and women were assigned to lower-carbohydrate (39-40% of energy) or higher-carbohydrate (51-53% of energy) dietary arms. Within these arms, participants consumed 2-week diets that were either high or low in resistant starch, separated by a 2-week washout. The findings present a striking metabolic trade-off. As expected, the high-resistant-starch meals successfully reduced postprandial insulin and glucose responses, demonstrating clear utility for meal-to-meal glycemic control. However, in the lower-carbohydrate context, the high-resistant-starch diet unexpectedly increased fasting plasma levels of TMAO and its precursors, including carnitine and betaine. When overall carbohydrate intake was high, TMAO levels were uniformly elevated regardless of starch digestibility, suggesting that baseline carbohydrate load dictates microbial fermentation pathways. Crucially, the short-term resistant starch intervention failed to improve fasting lipids, lipoproteins, or baseline insulin sensitivity.
This study complicates the established consensus on resistant starch. It suggests that while swapping digestible carbohydrates for resistant starch improves immediate glycemic markers, it simultaneously shifts colonic microbial fermentation in a way that ramps up pro-atherogenic TMAO production. For longevity specialists prioritizing actionable insights, this highlights a critical biological reality: single-variable nutritional interventions often produce competing multi-system trade-offs, pitting cardiovascular and metabolic pathways against one another.
Technical Biohacker Analysis
Study Design Specifications
- Type: Randomized, cross-over dietary intervention clinical trial.
- Subjects: Human adults; N=52 (32 women, 20 men).
- Design: Participants acted as their own controls across 2-week high-resistant-starch and low-resistant-starch periods, nested within higher-carbohydrate or lower-carbohydrate arms.
Mechanistic Deep Dive
- Gut Microbiome & TMAO Production: TMAO generation requires gut microbes to convert dietary precursors (like choline and carnitine) into trimethylamine, which the liver oxidizes into TMAO via flavin monooxygenases. High resistant starch intake fundamentally alters the colonic microbial community. The resulting shift appears to enhance the microbiome’s capacity to synthesize trimethylamine, even without increasing the dietary intake of carnitine or choline.
- Metabolic vs. Cardiovascular Trade-offs: The data highlight a divergence in organ-specific health priorities. The high-resistant-starch intervention improved metabolic readouts by blunting incremental area under the curve (IAUC) for 0.5-hour glucose and 1-hour insulin responses. Yet, it concurrently increased plasma TMAO. Elevated TMAO is mechanistically linked in the literature to macrophage foam cell formation, vulnerable plaque development, and platelet hyperactivity.
- Carbohydrate Dependency: The TMAO-raising effect of resistant starch was only significant when overall carbohydrate intake was restricted to 39-40% of total energy. Above 50% carbohydrate intake, TMAO generation was maximized independently of resistant starch content, suggesting a threshold effect for carbohydrate-driven microbial fermentation.
Novelty
- Prior to this, resistant starch was almost exclusively viewed as cardioprotective due to short-chain fatty acid (SCFA) generation. This paper is among the first to empirically demonstrate that high resistant starch actually increases circulating TMAO levels [Confidence: High].
- It introduces a previously unrecognized macronutrient interaction, proving that total dietary carbohydrate load dictates the microbiome’s TMAO-producing response to resistant starch [Confidence: High].
Critical Limitations
- Short Duration: The 2-week intervention periods are biologically brief. It is entirely unknown if the gut microbiome or hepatic flavin monooxygenase 3 (FMO3) adapts to resistant starch over months, which could theoretically normalize TMAO levels [Confidence: Medium].
- Translational Uncertainty: The study measures TMAO solely as a proxy biomarker. We lack hard endpoint data verifying whether this diet-induced TMAO spike actually accelerates atherosclerosis, or if the concurrent insulin-sensitizing benefits outcompete the cardiovascular risk in vivo [Confidence: High].
- Food Processing Confounders: Starch retrogradation during the mandatory freezing and reheating of study meals may have altered starch digestibility, potentially muting the true metabolic divergence between the high- and low-resistant-starch diets [Confidence: Medium].
- Missing Data: The paper lacks longitudinal tracking of endothelial function (e.g., flow-mediated dilation) or inflammatory cytokines to contextualize the physiological impact of the TMAO elevation.
2 Likes
This is an interesting development (the TMAO issue). UltaLabs does have a TMAO blood test:
LInk to the test: TMAO Test | Ulta Lab Tests
The Strategic FAQ
1. Does the insulin-sensitizing effect (lowered postprandial AUC) outweigh the cardiovascular risk of elevated TMAO in a non-diabetic individual? Answer: Highly doubtful. For a metabolically healthy longevity biohacker with an already optimized HbA1c and fasting insulin, the marginal benefit of blunting a meal-time glucose spike is vastly outweighed by the chronic endothelial stress and macrophage foam-cell formation driven by elevated TMAO.
2. If total carbohydrate intake was high (over 50% of energy), TMAO was elevated regardless of the RS dose. Does this mean the TMAO pathway is simply maximized by any large fermentable carbohydrate load? Answer: Yes. The data strongly suggests a threshold effect. High-carbohydrate diets appear to saturate the colonic fermentation capacity for TMA production, elevating TMAO to a ceiling where the addition or subtraction of RS makes no statistical difference.
3. This trial utilized high-amylose maize (Type 2 RS). Would Type 3 RS (retrograded starch, like cooked-and-cooled potatoes) produce the exact same TMAO spike? Answer: This remains unknown based on current data. Different types of RS have distinct physical structures and enrich entirely different bacterial consortia (e.g., Type 2 often enriches Bifidobacterium, while Type 3 might favor Ruminococcus). TMA production is highly taxa-dependent, so the TMAO spike might be specific to Type 2 RS.
4. The intervention was only 14 days long. Is the TMAO elevation a transient shock response of the microbiome, or does it persist chronically? Answer: This is a critical knowledge gap. The microbiome is highly plastic. While the initial shift forces a TMAO spike, we lack the longitudinal data required to know if the microbiome eventually reaches a new homeostasis that downregulates TMA production over a 6-to-12-month timeline.
5. Why did fasting lipids (LDL, ApoB) fail to improve despite the massive 48–66g/day RS dose, contradicting some older literature? Answer: The 2-week duration is likely insufficient to alter hepatic lipid packaging and clearance mechanisms. Furthermore, older studies often used RS sources that were co-packaged with soluble viscous fibers, which have well-documented lipid-lowering effects that pure RS lacks.
6. Could concurrent administration of a targeted prebiotic or probiotic rescue the TMAO spike by outcompeting TMA-producing taxa? Answer: Theoretically, yes. If you precisely engineer the gut microbiome by introducing non-TMA-producing butyrate generators, you could competitively suppress the specific clades (like Lachnospiraceae and Clostridiales) that were correlated with the TMAO spike in this trial.
7. Since TMAO increased on the low-carbohydrate/high-RS diet, is this driven by the starch itself, or by a shift in the microbial taxa that metabolize baseline dietary choline and carnitine? Answer: It is driven entirely by a microbial shift. The data explicitly shows that dietary intake of TMAO precursors (choline/carnitine) did not increase during the high-RS intervention. Instead, RS expanded specific TMA-producing bacterial taxa in the colon, ramping up the conversion of baseline dietary precursors into TMA.
8. How does the mandatory freezing and reheating of study meals affect the RS quantification and actual delivered dose? Answer: Heating in excess water gelatinizes starch, making it highly digestible, while cooling causes retrogradation (creating Type 3 RS). The freeze-thaw-reheat cycle likely altered the precise 16-fold difference in RS content between the high and low diets, introducing a significant methodological variable that could have muted the true metabolic divergence.
9. Is hepatic Flavin Monooxygenase 3 (FMO3) upregulated by the low-carbohydrate/high-RS dietary pattern, or is the TMAO spike purely due to gut-level overproduction? Answer: The study only measured plasma TMAO, not hepatic FMO3 expression. However, given the rapid timeline and the clear correlation with specific microbial shifts, the bottleneck is almost certainly an overabundance of gut-derived TMA flooding the liver, rather than an upregulation of hepatic FMO3 itself.
10. Did the high-RS group experience weight loss that could mathematically confound the glycemic improvements? Answer: No. Weight changes across the 2-week cross-over periods were clinically insignificant. The authors explicitly stated that adjusting the data for body weight changes did not statistically alter the glycemic, lipid, or TMAO responses.
TMAO and Cardiovascular Risk: Scholarly Debate and Knowledge Gaps
Elevated circulating TMAO (generally >6.2 μM) is strongly correlated with an increased risk of major adverse cardiovascular events (MACE), atherosclerosis, and all-cause mortality. However, a significant scholarly debate persists regarding whether TMAO is a causative agent of vascular damage or merely a biomarker of gut dysbiosis and metabolic dysfunction.
- The Causality Debate: While early murine models suggested TMAO directly promotes atherogenesis by altering cholesterol transport and macrophage activity, recent ex vivo analyses (e.g., Frontiers in Physiology, 2025) demonstrate that high TMAO concentrations do not acutely increase cardiac cell death. This supports the hypothesis that TMAO is a bystander—a readout of an unhealthy gut microbiome rather than the primary driver of cardiovascular pathology.
- The “Fish Paradox”: A critical knowledge gap remains regarding seafood. Fish is a primary dietary source of pre-formed TMAO and its precursors, yet regular fish consumption is robustly associated with cardioprotection and longevity.
- Required Data: To resolve these uncertainties, large-scale Mendelian randomization studies and localized metabolic tracking of the microbiome in human subjects are required to differentiate between the protective effects of specific diets and the isolated pathogenic potential of TMAO.
Actionable Insights for Longevity
TMAO is generated via a specific metabolic pathway: gut microbiota metabolize dietary precursors (primarily L-carnitine and choline) into trimethylamine (TMA). TMA enters the portal circulation and is oxidized in the liver by the enzyme flavin monooxygenase 3 (FMO3) into TMAO. Intervening in this pathway provides several targets for lifespan extension.
1. Dietary Precursor Restriction The most practical intervention is limiting the substrate required for TMA production. L-carnitine and choline are highly concentrated in red meat, egg yolks, and full-fat dairy. Transitioning to a Mediterranean diet has been clinically shown to significantly reduce circulating TMAO levels within four weeks. Furthermore, long-term plant-based diets alter the microbial taxonomy to such a degree that vegans produce negligible TMAO even when acutely challenged with a carnitine load.
2. Modulation via Phytochemical Compounds Specific polyphenols have demonstrated the ability to favorably alter the gut microbiome and reduce TMA synthesis. Compounds such as resveratrol, quercetin, and apigenin are currently being investigated for their capacity to inhibit the microbial enzymes responsible for cleaving TMA from its precursors.
3. FMO3 Enzyme Downregulation While choline is an essential nutrient and cannot be entirely eliminated, the hepatic conversion of TMA to TMAO can be targeted. Evidence suggests that high consumption of certain cruciferous vegetables—specifically Brussels sprouts—can naturally downregulate FMO3 activity in the liver, creating a metabolic bottleneck that lowers systemic TMAO concentrations without necessitating the complete avoidance of choline.
6 Likes
Berberine has a big effect on TMAO, you need a gram a day I think. My free AI:
Does Berberine use have any effect on TMAO production?
Berberine use
significantly reduces the production of TMAO (trimethylamine N-oxide). Research indicates that berberine acts as a “microbiota remodeler,” specifically targeting the gut-liver axis to inhibit the biosynthesis of this harmful metabolite.
[image]ScienceDirect.com +3
Mechanism of Action
Berberine reduces TMAO levels through several key biological pathways:
- Gut Microbiota Remodeling: It significantly alters gut bacterial composition, notably by reducing the Firmicutes/Bacteroidetes ratio. It decreases the abundance of TMA-producing bacteria such as Lachnospiraceae and Ruminococcus while increasing beneficial genera like Lactobacillus and Akkermansia.
- Enzyme Inhibition (CutC/D): Berberine and its metabolite, dihydroberberine, directly bind to and inhibit the activity of choline-trimethylamine lyase (CutC/D), the primary bacterial enzyme that converts dietary choline into TMA (the precursor to TMAO).
- Hepatic Modulation: In animal models, berberine has been shown to downregulate the expression of flavin-containing monooxygenase 3 (FMO3) in the liver, the host enzyme responsible for oxidizing TMA into TMAO.
[image]Nature +5
Clinical Evidence
- Atherosclerosis Patients: In a 4-month clinical study, patients taking 0.5g of berberine twice daily showed a 35% reduction in plasma TMAO and a 37% reduction in plasma TMA.
- Hypertension Patients: A study of hypertensive patients found that 0.4g taken three times daily reduced plasma TMAO levels by 16.7% over three months, which correlated with improved vascular function and lower blood pressure.
- Thrombosis Risk: By lowering TMAO, berberine has been found to decrease platelet hyperactivity and reduce the potential risk of arterial thrombosis.
[image]National Institutes of Health (.gov) +4
8 Likes
Fiber Is the New Protein
The Longevity Data Is Not Subtle
When The Lancet published its landmark 2019 meta-analysis of 185 prospective studies and 58 clinical trials, the findings were about as close to a nutritional mic drop as we get in evidence-based medicine.
Higher fiber intake was associated with a 15 to 30 percent reduction in all-cause mortality and cardiovascular mortality. Lower rates of coronary heart disease, stroke, type 2 diabetes, and colorectal cancer.
7 Likes
Is gas from Acarbose or all them?
2 Likes
The gas increased after I started using the Thorne Fiber Blend supplement. It has lessened since I have started taking the Acarbose separately (not at the same time). I am going to try the Green banana fiber after the Thorne runs out.
1 Like
I tried Green banana powder before - I tolerated it very well. Will buy again, but Acarbose didn’t work for me. My fasting BG is 90, but it spikes high after meals then goes fast back to the basic reading, but still keeps my HA1c at 5.9 - 6 no matter what I try. I’m not on Metformin or Berberine. Will try again (and again) to modify how I eat, and help me God ![]()
5 Likes
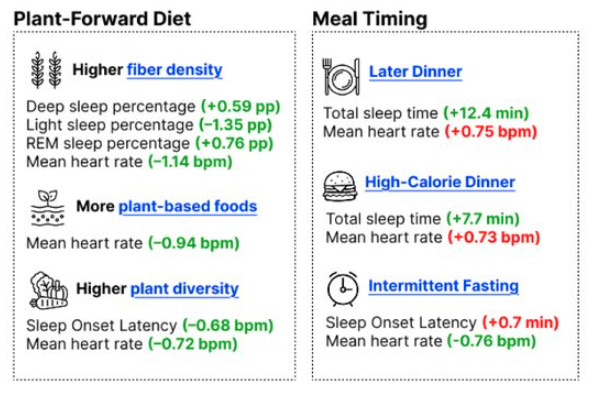
People who eat a lot of fibre spend more time in deep sleep
The most comprehensive study to date has revealed what we need to eat throughout the day to sleep well that night
Eating more fibre may help you sleep more deeply, while consuming a wider variety of fruit, vegetables and nuts could help you nod off faster. That’s according to the most comprehensive look yet at how what we eat throughout the day affects our sleep that night.
“Increasing fibre and plant variety is already recommended for overall health, carries low risk for most people and may offer sleep benefits as an additional upside,” says Hagai Rossman at the Weizmann Institute of Science in Israel.
Prior studies have linked eating fibre-rich, plant-based foods to better sleep, but these mostly relied on people recalling their diet in surveys, sometimes weeks or months later. In addition, when sleep has been objectively measured, it has typically been via movement trackers that cannot distinguish between its deeper and lighter phases, which is important for gauging sleep quality.
Now, Rossman and his colleagues have gained the clearest picture to date by analysing sleep and dietary data collected from more than 3500 adults, aged 53, on average. “Previous studies haven’t looked at so many dietary and sleep factors,” says Marie-Pierre St-Onge at Columbia University in New York City.
Over two consecutive days, each participant logged what they ate in a mobile app, either during its consumption or shortly afterwards. At night, they wore a device that has been approved by the US Food and Drug Administration to measure sleep. This is comprised of sensors worn on the chest, a wrist and a finger that track snoring, blood oxygen levels, and heart and breathing rates.
…
It is unclear exactly why fibre has these effects, but studies suggest that gut microbes can ferment it into short-chain fatty acids, such as butyrate, that reduce inflammation and alter gut-to-brain signalling in a way that promotes deep sleep, says Rossman.
The researchers also found that those with an above-average fibre intake had a slightly lower heart rate during the night than those who consumed less. A low nocturnal heart rate suggests that a person has entered a state of deep rest and repair, which puts less strain on the heart. “A 1 beat-per-minute difference [as observed between the high- and low-fibre groups] might not be that important for one night, but if that difference is sustained over decades or a lifetime, that could make an important difference [for cardiovascular health],” says St-Onge.
Read the full story: People who eat a lot of fibre spend more time in deep sleep (New Scientist)
Related Research Paper: medRxiv DOI: 10.64898/2026.02.17.26346471
6 Likes
Fascintaing stuff that just validates the gut brain axis and the power of longest information superhighway there exists in our bodies. Its called Vagus nerve.
Butyrate → vagal activation → higher HRV → more stable:
Respiratory sinus arrhythmia
Baroreflex sensitivity
Reduced nocturnal sympathetic spikes
This decreases:
Micro-arousals
Sleep fragmentation
C) Reduces Neuroinflammation
Butyrate is an HDAC inhibitor.
In CNS:
Lowers microglial activation
Reduces inflammatory tone in hypothalamus
Improves circadian gene expression (CLOCK/BMAL1 modulation)
Inflammation disrupts SWS — reducing it improves depth.
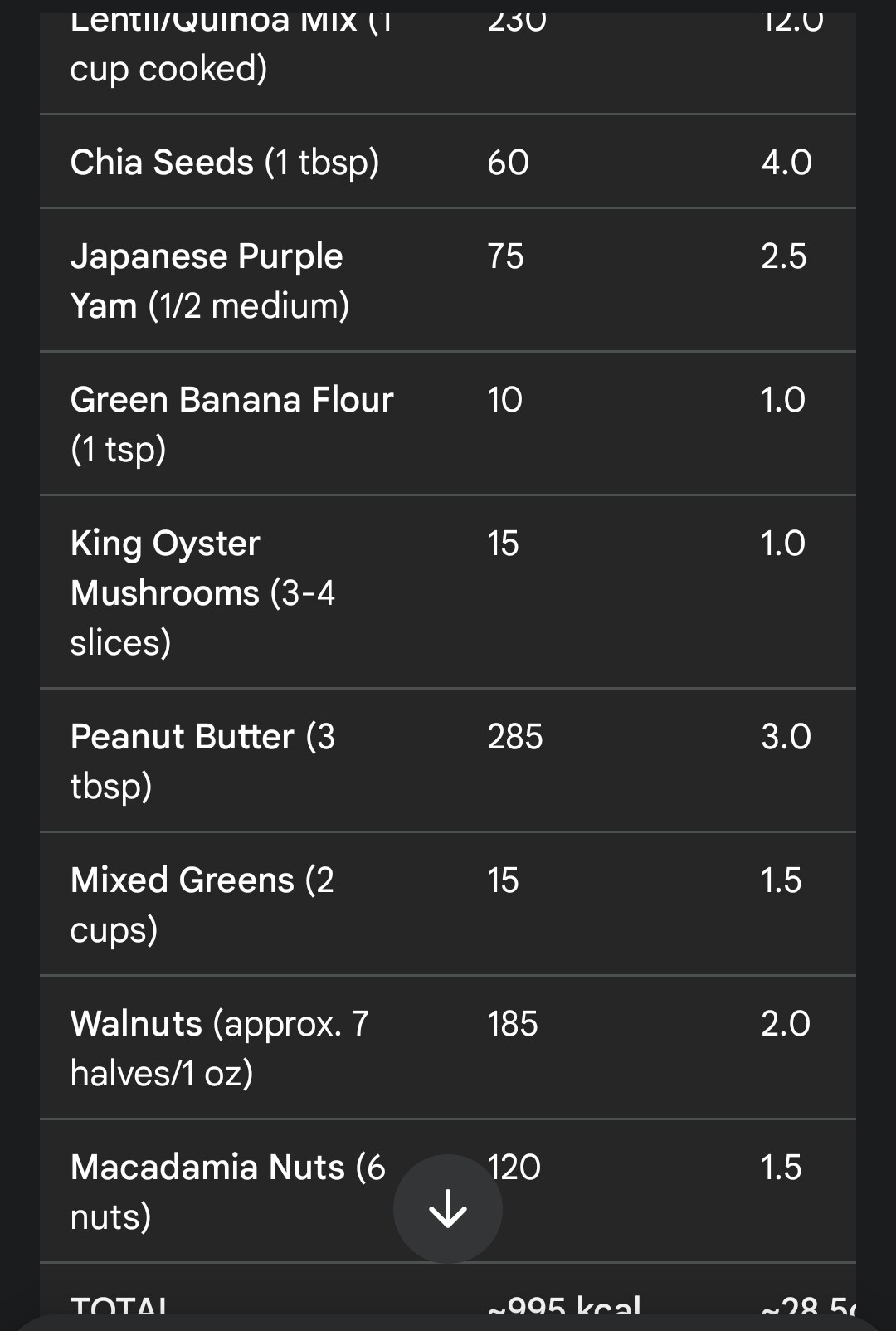
Had 29 gm worth of fiber rich supper this evening. Will see how the HR trends and the deep sleep tonight.
7 Likes
Simulations of your gut may predict which probiotics will stick
Tests of “digital gut” simulations hint at personalized probiotics but not a cure‑all yet
Figuring out which bacteria or other nutrients your gut needs may one day be as simple as running detailed computer simulations.
From pills to yogurts to sodas, probiotics are being repackaged and marketed to us more and more, with the promise of boosting our “gut health.” But while commercially available probiotics work for some people, this one-size-fits-all approach hasn’t reliably benefited consumers. Instead, new simulations can predict whether a specific bacterial strain will successfully take up residence in a person’s gut, researchers report February 19 in PLOS Biology.
2 Likes