While not exactly what the article is referencing, I can say anecdotally that it’s much easier to keep my vitamin D levels above the 30ng/mL threshold (arguably one should shoot for higher, but that’s a reasonable cutoff between low and normal) after losing about ~40 lbs. When my weight was in the low 200s, even with 50k IU per week, my levels were just barely about 30ng/mL in the summer of 2021. Summer of last year I tested a bit higher, but with zero supplementation required.
High dose vitamin D increases death rate in randomized trial:
60 000 IU once a month was used in the study. Which would be 2000 IU a day (!).
I don’t have full access to the paper. But I think the blood levels would probably be similar for daily dosing vs. once a month for vitamin D.
Ouch, been taking Vit D sparingly here and there in high doses and now maybe i should just stop. That death increase is HUGE, not just significant lol.
Vitamin D deficiency is terrible, but mega-dosing is also not good. It’s hard to tell how much to take and it really depends on the person. This study was done on a mostly elderly Asian population which tends to be much skinnier/thinner and therefore more affected by vitamin D3 supplementation due to low body weight on average.
Pre-Diabetics should take 4,000 IU daily. 50% of the population has a vitamin D deficiency. Vitamin D3 is metabolized poorly in overweight individuals. 4,000 IU helps prevent serious outcomes of COVID. 60,000 IU monthly leads to a higher risk of death. If you spend a lot of time in the sun, you need less.
1,000 IU? 2,000 IU? 4,000 IU? 5,000 IU daily? I think we can all agree that more than 5,000 IU daily is a bad idea and 1,000 IU is a good minimum.
Honestly, vitamin D is one personalized/confusing supplement where one size does not fit all. I alternate between 1,000 IU and 5,000 IU. I think I need to be in the 1,000-2,000 IU daily range from here on out as I am deficient.
Me at 50K/week D3 and 120lbs:
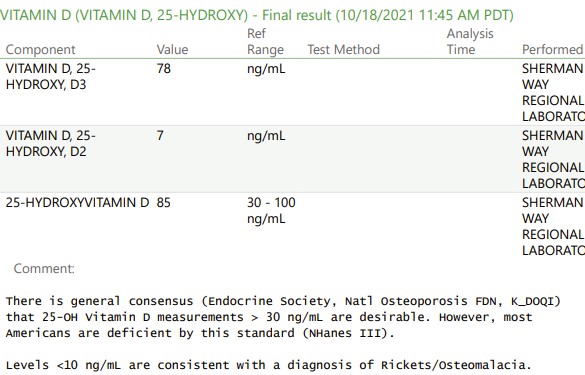
It was in the 20-30 range before supplementation.
And then I see the Stanfield thing and apparently Kaiser is trying to kill me.
I did some n=1 experimentation with large doses of cholecalciferol (d3) taking 24,000 and 12,000 doses. I found it disrupted my sleep for a day or three as my liver processed it into 25 hydroxy vitamin d (25ohd). I concluded that it was mildly toxic as cholecalciferol. I take a maintenance dose of 3000 d3, but that is insufficient to keep me at high normal. When i want to increase my serum levels i take 25ohd. I like to keep serum levels along the top end of the normal range. I concluded i could metabolise 3000iu per day, but 6,000 was too much. Those figures may now have shifted, but i continue to aim to keep my serum levels at high normal.
I think I am going to read the full paper soon, but I am going to make sure I get 1000 IU a day, which was more convenient than 2000 IU for me. I heard about 1000 IU from Brad, which was according to endocrine society guidelines.
Do you have a source for that? Last time I checked there was no good evidence for covid/vitamin d.
If it’s a recent paper, seems no good:
I suggest reading;
“How Not To Die With True High-Dose Vitamin D Therapy: Coimbra’s Protocol and the Secrets of Safe High-Dose Vitamin D3 and Vitamin K2 Supplementation”
By Tiago Henriques
In my view the book is worth reading/ purchasing{yes, I have purchased a copy earlier part of last year]. This is the English translation from the original, which is in Portuguese.
I do take very large amounts of D³ 40,000IU plus{80,000IU highest dose I have taken] daily for several weeks/months at a time, then a break. And my blood levels do not go much above 50.
If I had a PDF copy available I would post.
 for Multiple Sclerosis")
Yes, there was a study I linked to on this site about how vitamin D3 prevented COVID. It was a study done on 400 healthcare hospital workers in Mexico. The findings were significant.
6.4% vs 24%
It wasn’t done on 400, but 321, and more than 30% dropped out during the study. So it ended up being around 100 in each group, and we don’t know what happened to the 50 in each group.
Also the randomization failed, with 6.2% having diabetes in the placebo group, but 1.9% in the vitamin d group. And 23% were nurses in the placebo group, while it was 16.2% in the vitamin D group.
So it is a weak study.
Its convincing enough for me when combined with the other available information for me to strive to overcome my vitamin D deficiency.
To me the issue is mechanism. Vitamin d operates primarily through 1,25 di hydroxy vitamin d. This when bound to VDR enables more of the genome to function (mainly expeession but also transrepression)
Generally therefore more proteins will br produced with higher vitamin d levels.
I hypothesise that the reason mammals have a part of the genome that responds to vary energy demands by the annual cycle is because food is more available when there is more sunlight.
So we have functions that only operate when there is plenty of energy. One assumes that the genes are evolutionarily beneficial. It may be that cycling these has merit, but generally i would like this part of my genome to function.
Hence i aim for the upper level of normal.
Very interesting hypothesis! I had never thought of it in that way. It would fit with evolutionary theory if true.
@A_User Just out of curiosity, what are the best trials or studies you have found that have led you to change your supplement stack or habits?
I am always looking for high quality advice and information.
Interesting data. A few thoughts -
Using a dose of 2000IU per day, the very large (~25,000 participants) VITAL study that was discussed in the OP’s article found a small (HR .99) but not statistically significant decrease in all-cause mortality. There was a statistically significant reduction in cancer mortality when they did analyses that excluded cancer deaths in the first or second year of the trial, as that would likely be too early for any benefit to show up and those cancers may have already been established or “simmering” before the trial started.
Based on that, you may be thinking “well, it must have been the large bolus dosing of 60k IU per month that was problematic.” Another very large trial in Australia called D-Health used that same dose and found a small increase in all-cause mortality (HR 1.04), though it was nothing close to the 1.29 HR in the study that tweet is discussing, and it did not reach the level of statistical significance. This study did find an increase in cancer mortality (HR 1.15), but that also did not reach statistical significance. Even though neither was statistically significant, this does point to the possibility that at a given monthly dose of Vitamin D, it’s better to split it up into daily doses rather than taking it all at once.
Although weekly or monthly doses have been found just as effective as daily doses at correcting Vitamin D deficiencies, a larger dose is metabolized quite differently, which could produce different biological effects. There could also be differences based on one’s ethnicity and genetic background, as this trial that found such a large increase in death rates drew its subjects mostly from Indian and Asian populations.
My takeaway from all the Vitamin D research I’ve looked at over the years - the benefits and risks of supplementing likely vary depending on your baseline characteristics (BMI, baseline vitamin D levels, existing illnesses, maybe even your ethnicity) and what outcome you’re actually looking at (bone health, auto-immune disorders, depression, all-cause mortality, cancer occurrence/CVD events and cancer/CVD mortality, etc). This could also be another example of a biomarker that shows big impacts when you look at one’s “natural baseline” level, but changing that level with medications or supplements might have much less significant effects. The classic one that I’m thinking of is HDL cholesterol, where there is evidence that having higher baseline levels lowers CVD risk, but when they studied medications designed to raised HDL, they found either no benefits, or an increase in risk that was so significant that they had to stop the trial.
Selected articles of interest:
My personal experience is that unmetabolised cholecalciferol messes up my sleep. What other harm it does i dont know, but if it were to reduce melatonin production that would have knock on effects
So, best to take it in the morning? That would make sense. Thanks.
I have gone for taking it in the morning for exactly that reason. It is always worth thinking how the body processes molecules. Vitamin D particularly has a storage form (25OHD) and one or two active forms. (1,25 and 24,25 Di Hydroxy Vitamin D).