On September 23rd I took 1 packet of biocon and 2 packets of zydus with GFJ and a bit of pomegranate. The Grapefruit was half eaten a while before the rapamycin and half with the rapamycin.
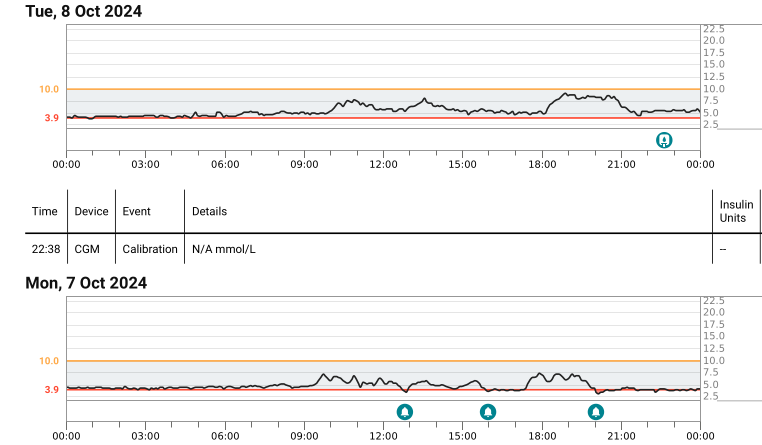
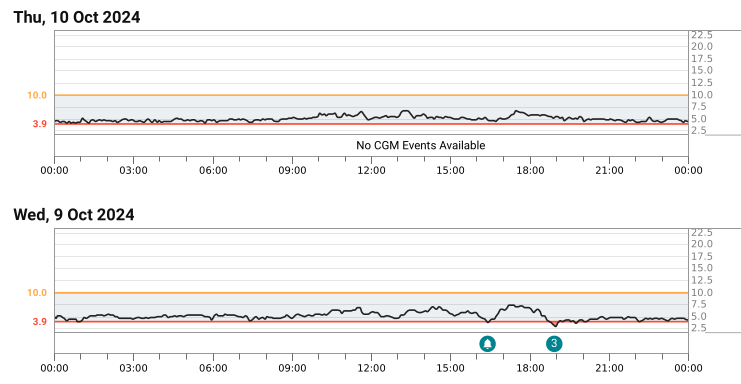
This time I had been wearing a CGM (One+) for a few days before taking the rapamycin. It fell off and I got another, I then used a third on schedule, but it stopped uploading on Sunday and that got fixed part way through Tuesday.
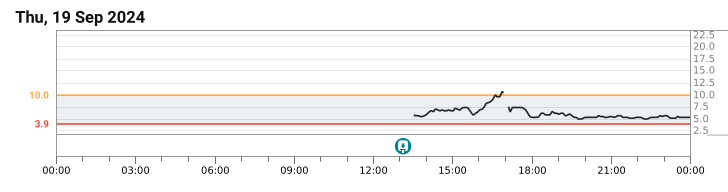
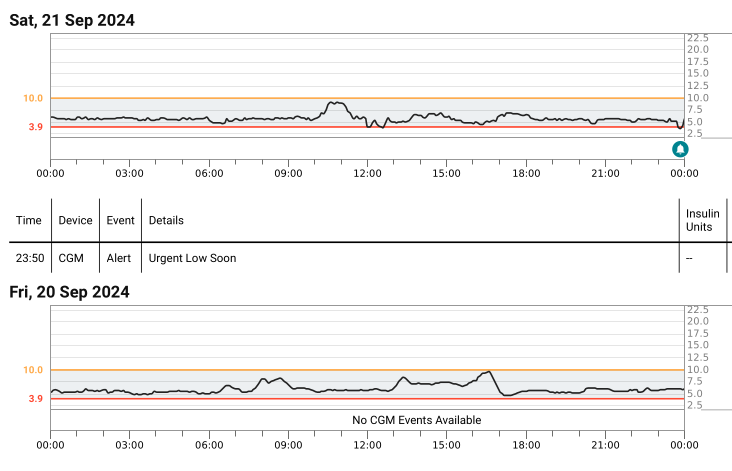
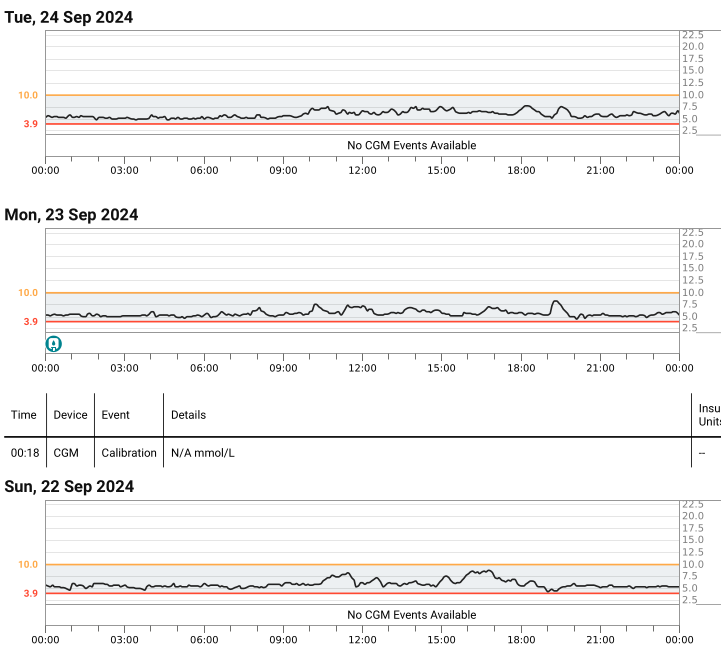
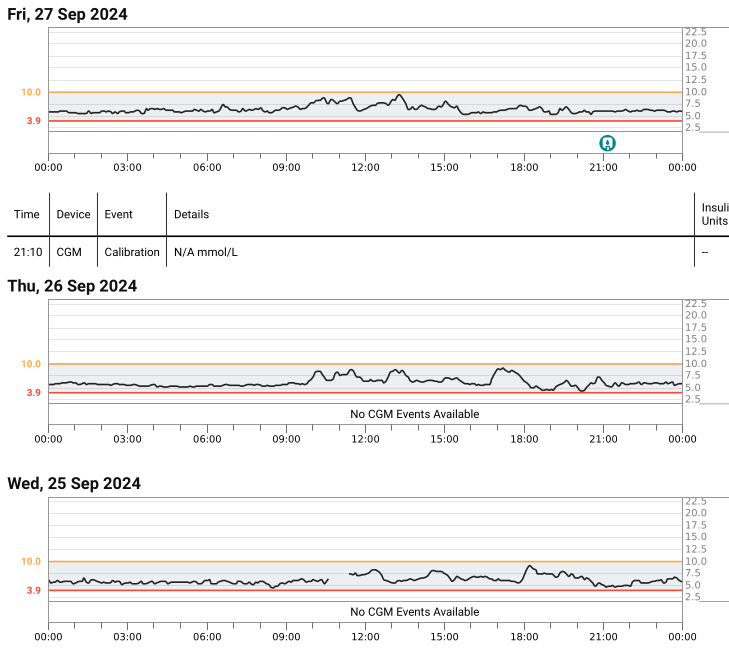
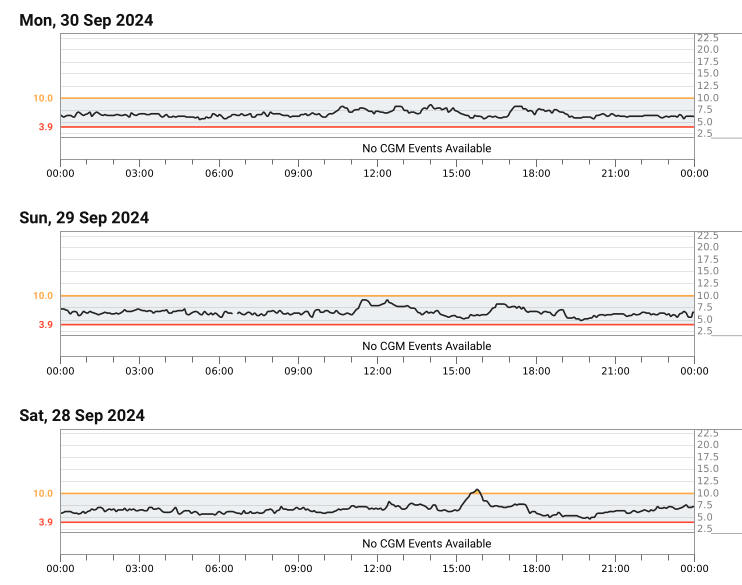
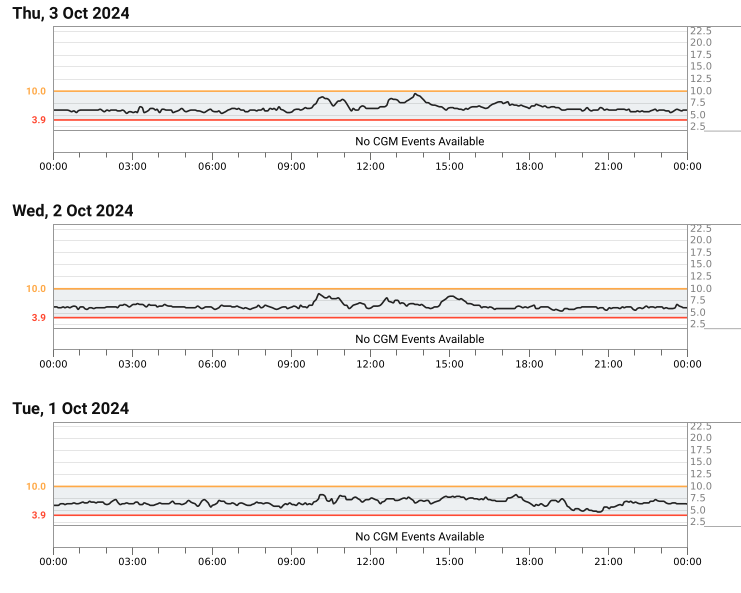
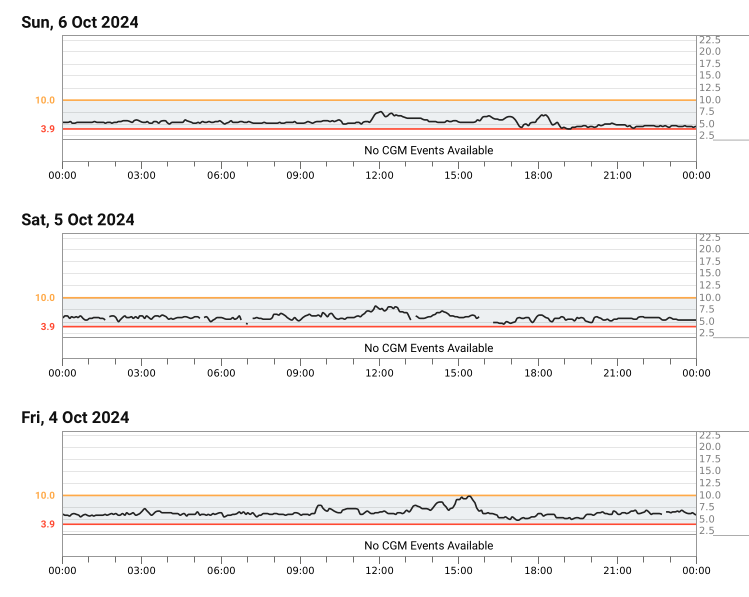
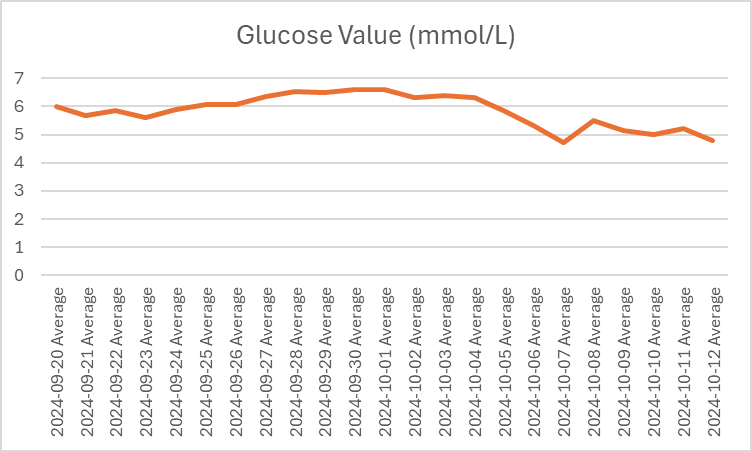
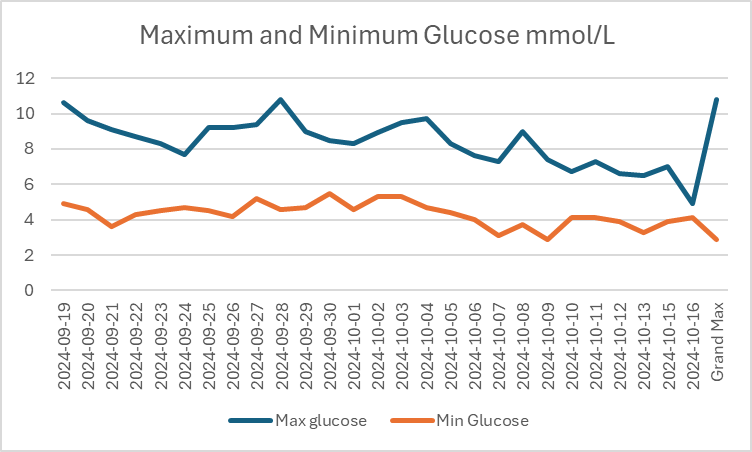
It will take some work to produce useful reports from this, but I have already done an average glucose chart. I have excluded the days with part data as they will not have useful averages. The results are skewed a bit by alcohol consumption. Alcohol takes down the average glucose. The results, however, still show a useful pattern of Rapamycin initially driving up the average glucose figure. Interestingly it appears that it is the baseline that moves up moreso than the peaks.
The body adjusts to produce more insulin, but the rapamycin fades and so at a point when the rapamycin has no immediate effect the blood glucose average goes lower.
This is vulnerable to errors in sensors. I did not calibrate them as that itself could add an additional error as the fingerstick might not be right. I will tidy up the charts and upload them later, but here is the average daily glucose.
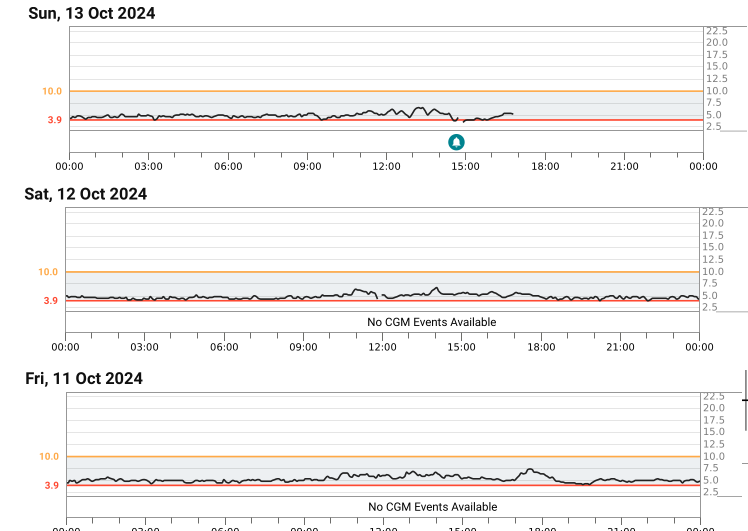
My last full day has average glucose of 4.778745645 which is about HbA1c of 4.6%. That was Saturday 12th October and I didn’t drink that day although it was affected by me drinking on the Friday which has an effect into the early morning.
")