If you suspect hepatic glucose production elevation, then the only agent which addresses hepatic gluconeogenesis is pioglitazone. Metformin does not.
All that with 25mg/day of Empagliflozin which makes me pee glucose like crazy (Checked with urine strips).
Yes, there are studies showing that empagliflozin use increases neoglucogenesis in a compensatory manner, so it’s not shocking that if hepaticneogenesis is your issue, empagliflozin doesn’t have much effect. I’m in the same boat, which is why I’m exploring low dose pioglitazone (7.5mg/day), perhaps sometime next year.
Thanks for sharing your data! I think it’s premature to conclude that your rapa-induced hyperglycemia is not due to insulin resistance on the basis that your OGTTs are normal or even improved on rapa is premature. First, you’re on empagliflozin, which blunts your OGTT regardless. And second, excess hepatic glucose output is a normal result of hepatic insulin resistance: that’s why metformin works. So a reasonable reading is that rapa may be causing you hepatic but not muscular insulin resistance.
Btw. here’s the study establishing that pioglitazone inhibits hepatic gluconeogenesis, while metformin does not (I’ve posted this study before). The study is in DMT2, but no reason to suspect that it’s any different in pre-diabetic or normal glucose individuals.
Comparison of the Effects of Pioglitazone and Metformin on Hepatic and Extra-Hepatic Insulin Action in People With Type 2 Diabetes
“[…]pioglitazone enhanced (P < 0.01) insulin-induced suppression of both glucose production (6.0 ± 1.0 vs. 0.2 ± 1.6 μmol · kg−1 · min−1) and gluconeogenesis (n = 11; 4.5 ± 0.9 vs. 0.8 ± 1.2 μmol · kg−1 · min−1). Metformin did not alter either suppression of glucose production (5.8 ± 1.0 vs. 5.0 ± 0.8 μmol · kg−1 · min−1) or gluconeogenesis (n = 9; 3.7 ± 0.8 vs. 2.6 ± 0.7 μmol · kg−1 · min−1).”
Meanwhile here’s a study showing that empagliflozin causes compensatory increase in gluconeogenesis:
Inhibition of Sodium-Glucose Cotransporter-2 during Serum Deprivation Increases Hepatic Gluconeogenesis via the AMPK/AKT/FOXO Signaling Pathway
“These data show that SGLT2 mediates glucose uptake in hepatocytes and that SGLT2 inhibition during serum deprivation increases gluconeogenesis via the AMPK/AKT/FOXO1 signaling pathway.”
Low dose pioglitazone (7.5mg/day) is as about as effective at lowering A1C and FBG as full dose or high dose, but with fewer side effects:
The Low-Dose (7.5 mg/day) Pioglitazone Therapy
“The low-dose pioglitazone therapy may show the same degree of improvements in glucose and lipid metabolism, fatty liver, insulin resistance, and adiponectin as the standard- and high-dose pioglitazone therapy. Furthermore, the low-dose pioglitazone therapy may also show less adverse effects on weight gain, edema and heart failure as compared with the standard- and high-dose pioglitazone therapy.”
I think you cannot say this without measuring at least insulin levels during OGTT. Your insulin levels might be in a prediabetic range postprandial indicating insulin resistance with rapamaycin.
Some might say even dynamic insulin level measurement is not sufficient and it requieres hyperinsulinemic euglycemic clamp to measure insulin sensivitiy or resistance. It has been shown by Defonzo that e.g. healthy kids have normal glucose repsonse in OGTT, but are insulin resistant.
I take a high dose (higher than you) of Rapamycin, but quite infrequently. I posted the results from one here:
What I see happening from a single dose is
a) A development of hepatic insulin resistance
b) An over compensation by producing more insulin.
c) The fading of insulin resistance
d) An overswing where glucose goes low
e) back to normal.
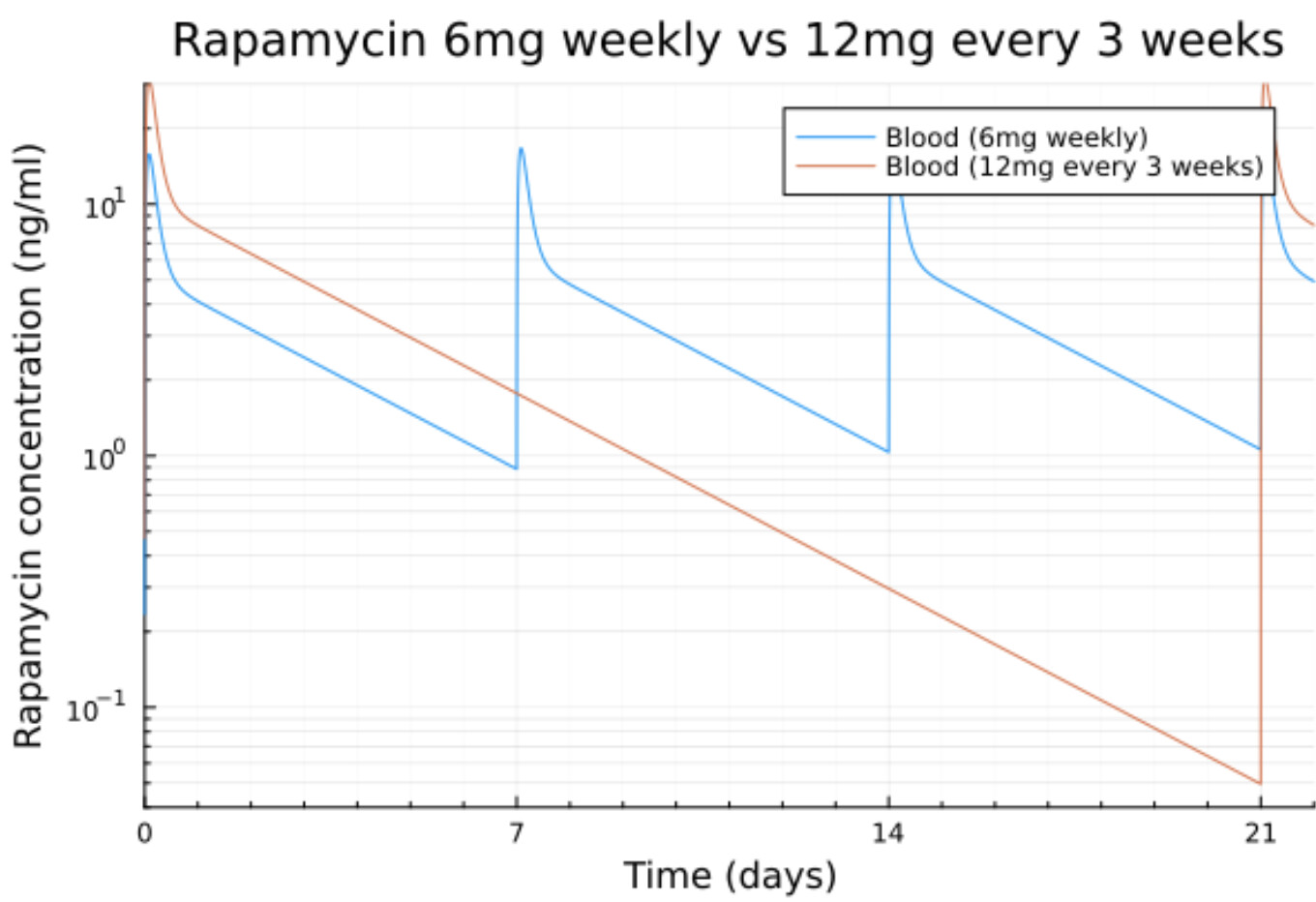
With 12mg fortnightly your trough is still going to have some mTOR inhibition which I think is the mechanism for the hepatic insulin resistance. I don’t think I would want to take that much that frequently.
With my large, but intermittent dosing I get back to normal.
Metformin never worked for me. I tried it several times in the past with various doses without any change in glucose. I’m currently re-trying it to see it it could work in addition to the SGLT2i and the GLP1-RA but no change either.
Also the OGTT shows that I can clear 75g of glucose in less than 2h so, whatever amount of insulin used for that, it was enough. My issue is that, even fasted, I’m at 120mg/dl with rapamycin vs less than 100 with rapamycin.
If we look at the daily CGM plots we see that with rapamycin, the fasted baseline is around 120 and that the postprandial spikes after the 2 meals went back down to that baseline (below it even).
Basically the glucose regulation works but with a fasted baseline of 120 instead of less than 100.
With my latest blood rapamycin measurements I get a trough at 0.3 ng/ml after 2 weeks and 0.05ng/ml after 3 weeks when things start to normalize again.
Also at 12mg the max at equilibrium is around 8 ng/ml so maybe it’s too high and cause mTOR2 inhibition as we know that this can be caused by staying too long at some level but also with a level too high.
A very interesting post. Thank you.
I have steroid-induced DM. 10 years of 15-50 mg of prednisone. I take pioglitazone, empagliflozin and acarbose (with carbs). Lean (11%fat on Dexa), aerobically fit (6+ h per week plus weights), and also carb restricted. Gluconeogenisis is a huge factor here, and even fasting/exercise had zero effect before the meds, and improved but still present after.
8 mg rapamycin q 2 weeks had similar effects. Only detected via random blood pricks.
I ended up buying a CGM (off rapa) and did two 75 g GTT’s. One before daily prednisone (nearly normal), and one during peak steroid effect (not normal!).
I will stay the course for now, but once the neurosis-inducing effects of the CGM have worn off, I’ll repeat those trials on rapa.
Again, gratitude for your post.
I used CHBT to calculate AUC and predicted insulin requirements in my two OGTT’s see post below for why I did them). Big increase in both.
Again, grateful for your post.
This is purely speculative on my part, but I suspect that the body interprets rapamycin as a “stressor”, with HRV, HR, impacts and (in those not adrenally suppressed), a cortisol response.
I wonder if it is cortisol, not MTORC2 that is driving this short term response.
Looks like it’s a direct effect of Rapamycin suppressing mTORC1 and not a side effect (or mTOTC2 inhibition) as I thought.
Here is a detailed explanation from ChatGPT 4.5:
Then I got it to explain Why is rapamycin-induced glucose elevation termed as hepatic insulin resistance?
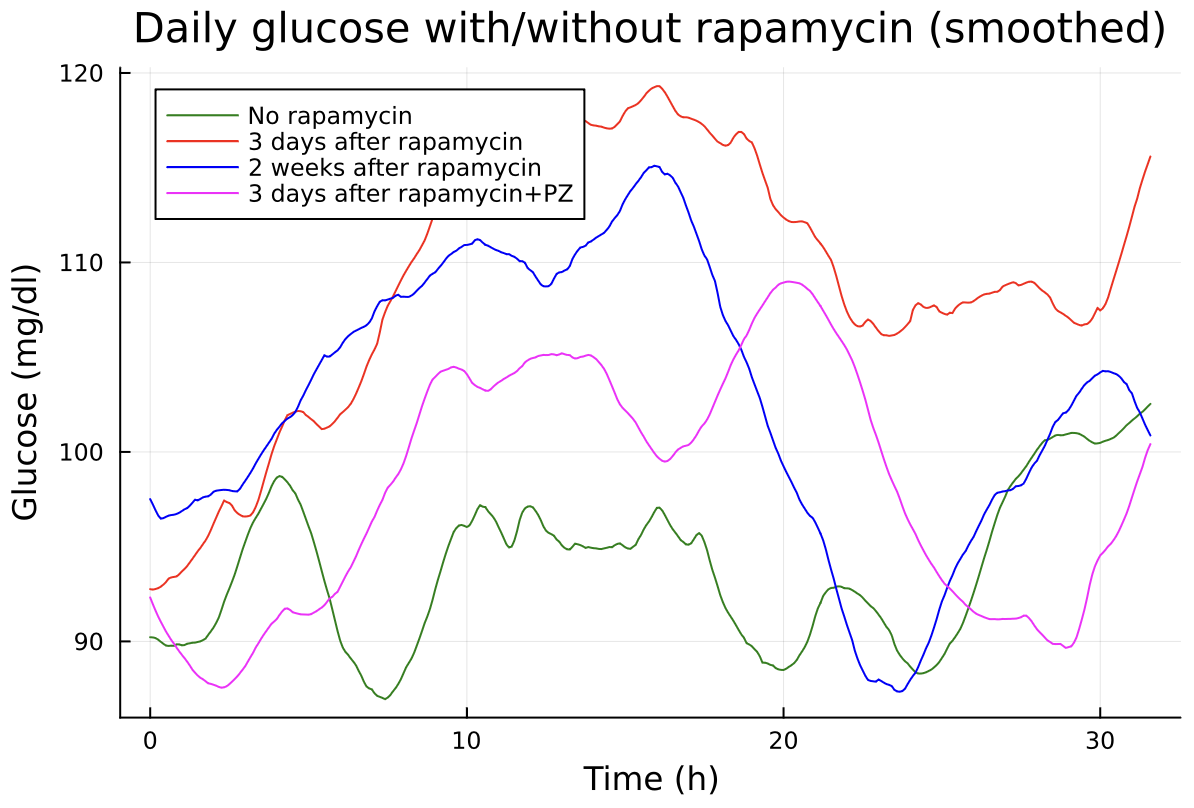
Update: Started to take Pioglitazone 7.5mg/day (PZ)
Looks like that’s finally something that works for me. If you look at the magenta curve (3 days after rapamycin+PZ) it’s not too bad especially compared to the red line (3 days after rapamycin) or even 2 weeks after rapamycin without PZ.
BTW it’s the tri-therapy pushed by Ralf DeFronzo: Pioglitazone + GLP1-RA (Tirzepatide) + SGLT2i (Empgliflozin). It’s even a quadri-therapy when I take acarbose with meals.
That’s depressing. I guess I should congratulate, but I’m rather enervated by these graphs. A freakin’ quadri-therapy and that’s all it gets you. I would’ve hoped for absolutely stellar results. What chance do I stand, when I’ll be limited to only a dual-therapy - I am on SGLT2i (empagliflozin) and am contemplating pioglitazone, that will make it TWO, possibly, possibly incorporate acarbose. I have no current plans for GLP-1RA. I really was hoping for more from the addition of pioglitazone. I suppose I will suspend judgment until you have a reading of A1c. If pioglitazone brings A1c to some civilized level, I would take that as a cautious win.
Right now that green curve looks reasonable, although it starts trending up later toward 26+ hours, where it crosses the magenta line (plus toward the beginning, same situation). I would’ve wanted pio to look like the best parts of green and magenta curves
I think it might work if like me the issue is with excessive hepatic glucose production. In that case PZ is more useful than a GLP1-RA.
That said the idea behind the try-therapy is that the GLP1-RA will block the possible weight gain from PZ. So far I my weight has not changed either way.
Me too but the magenta is 3 days after rapamycin (12mg). I will post how it will be 3 weeks after rapa. Hopefully it will be good as there is not much I can add to that.
You might interested to see the pioglitazone thread where I posted a study showing the combination of telmisartan and pioglitazone resulted in no weight gain from pio and no impingement on the insulin sensitizing of pio from telmi. There are more studies there that I posted, which seem to indicate that telmisartan and pioglitazone are a good combination. Of course, if you have no need/use for BP lowering, then it’s irrelevant. However, I have an ever so slight tendency to BP excursions into the 130/80 territory, and I think a judicious addition of telmi might be indicated for me - this would avoid the need to use a GLP1-RA.
And yes, my issue seems to be excessive liver gluconeogenesis, which results in elevated dawn effect, as well as elevated BG readings right after exercise. There are no real excursions in response to meals. This issue has been bedeviling me for over 10 years now, where I hover in the pre-diabetic 5.7-5.9 range no matter what I do. So far, I have not noticed any effect from rapamycin, oddly enough.