The mTOR pathway is central to maintaining cellular growth, autophagy, and metabolic balance in neurons—processes vital for brain health. In AD, dysregulated mTOR signaling is linked to impaired autophagy and the accumulation of toxic proteins, including Aβ plaques and hyperphosphorylated Tau, which drive neurodegeneration. Additionally, excessive mTOR activation is associated with heightened oxidative stress, mitochondrial dysfunction, and neuroinflammation, all of which exacerbate cognitive decline in AD (Davoody et al., 2024).
Beyond its role as an mTOR inhibitor, rapamycin exerts diverse effects on immune modulation and cellular homeostasis through both mTOR-dependent and independent pathways. It modulates immune responses by influencing T-cell activation and differentiation, promoting immune tolerance through enhanced regulatory mechanisms. Furthermore, rapamycin induces autophagy, a critical cellular process for degrading and recycling damaged proteins and organelles. By activating autophagy, rapamycin may reduce Tau pathology and Aβ accumulation—key drivers of AD progression. This autophagic activation underpins rapamycin’s neuroprotective properties, offering the potential for alleviating AD pathology by clearing neurotoxic aggregates (Davoody et al., 2024).
I improvements like that I almost wish I was an APOE4 mouse (technically E4FAD), instead of an APOE4 human!
I’m a beginner when it comes to reading scientific publications. I wasn’t able to see the description of the experiments (how many mice, groups, etc) that produced this data. I must have missed something because,I don’t understand what value this publication provides. It writes about things that are well known: e.g. the APOE4 allele increases Alzheimer risk. And then it quotes data from other publications.
Yeah when I’m back on Rapa (around July / August at this rate) I’ll do 1 mg / day for a time, maybe a few months, and see what happens. I’m almost sure it won’t be optimal to keep up that dose forever and periodic breaks will be needed, and maybe a switch to ultra high dose low frequency like @John_Hemming’s. But what I am curious about is HOW sirolimus was able to exert this effect at this dose, seeing as it doesn’t cross the BBB unless at a much higher and prolonged concentration. Though the evidence for the latter statement always seemed too spotty and hypothetical. There’s also the increased BBB permeability of apoE4 carriers like myself so that probably works in favor of drug penetration.
In regard to the dosing, safety is a factor - but you’ll likely have some immunosuppression and adverse effects if you take 1 mg/day. We’d need to see levels. I’d say most people can get away with this for 1 month, but on a safety basis, I’d be very reluctant to dose this way longer term.
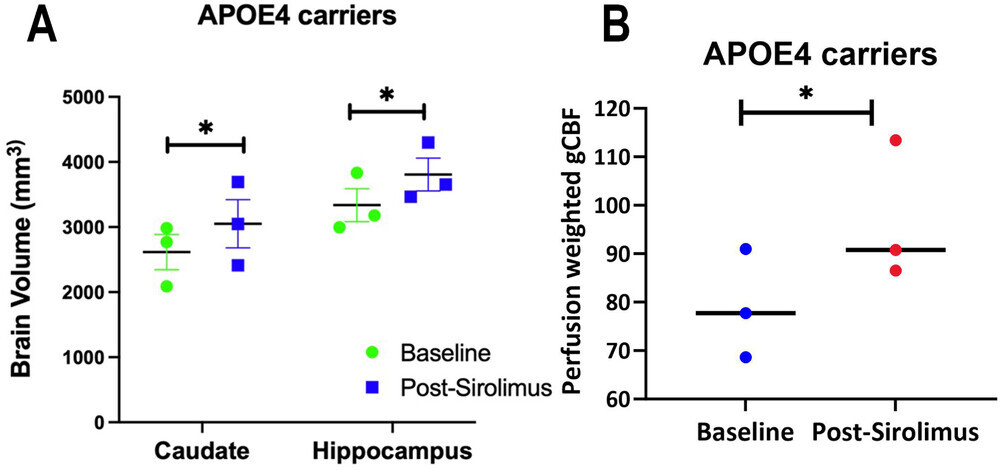
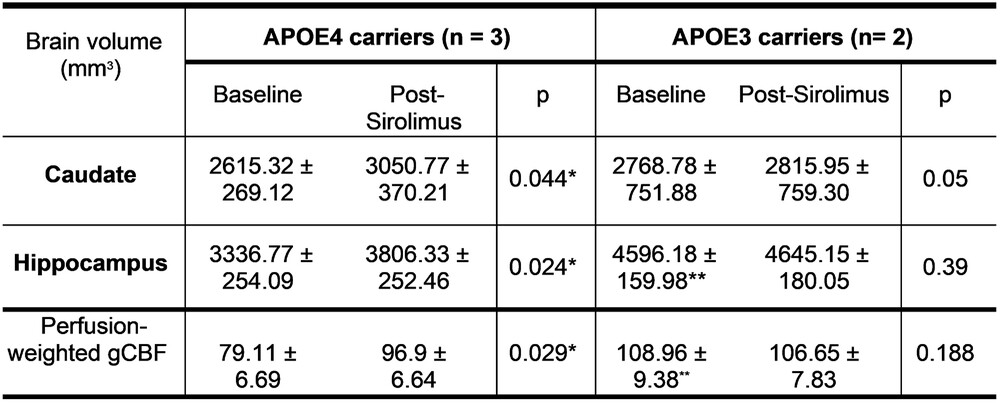
Low dose Sirolimus (1 mg/day) was given for 4 weeks to three middle-aged, cognitively normal APOE4 carriers (F:M = 2:1) and two female APOE3 individuals (45-65 yrs; MOCA > 27).
APOE4 carriers had significantly increased Caudate and Hippocampal volumes (Fig. 1A) and gCBF (Fig. 1B) after 4 weeks of Sirolimus treatment.
No side effects were observed, and no changes in blood glucose and HbAc1 levels were found in all the participants.
Tiny study (n=5), not randomized, not placebo controlled.
It would have been great to measure after one month without rapamycin to see whether the biomarkers return to baseline or stay high. If they stay constant, then one could just do 4 weeks of 1 mg/day once a year to protect their brain. Or a single yearly large dose (@John_Hemming’s strategy?).
Anyway, I wasn’t convinced by rapa’s neuroprotective potential but there’s a growing body of evidence…
Also: is there a risk with low-dose rapa (1 mg/day vs 5 or 6 mg/week)? See:
Caveat: the CARPE_DIEM phase 1 trial of rapa 1 mg/day in AD found worse cognition scores after 8 weeks and 0 rapa in the CSF: ClinicalTrials.gov They’re still following up with phase 2 (NCT04629495), n=40, results in 2026.
The ERAP trial in AD (NCT06022068) is supposed to have just completed. “7 mg taken once per week during 26 weeks.” So we should expect results soon? I’ve just emailed the researcher. In their protocol, they wrote:
Notably, the data on side effects is based on the use of rapamycin following organ transplantation, where the drug is commonly used together with other immunosuppressants. In the ERAP trial, we plan to deviate from the standard dosing of rapamycin in two ways. Typically, when used as an immunosuppressant, rapamycin is administered orally at a daily dose of 2 mg or above [43]. We will instead administer an overall lower dose but in an intermittent fashion; a weekly oral dose of 7 mg. This change is aimed at reducing the risk of adverse events. The rationale behind this is that positive effects of rapamycin are hypothesized to be caused by inhibition of the mTOR1 complex, while many of the side effects are hypothesized to be due to inhibition of the mTOR2 complex. While mTOR1 is sensitive to acute dosing treatment, mTOR2 requires sustained exposure of the drug to be effectively inhibited [45].
The extent to which rapamycin crosses the blood-brain barrier (BBB) in humans has not been thoroughly investigated. Rapamycin is a large molecule (molecular weight 914.2) and a substrate, albeit with low affinity, for the efflux pump P-glycoprotein [46]. Compounds with these properties are often considered unlikely to pass from intestine to blood and bind to an intracellular target [47]. It is however known, from long clinical use, that oral treatment with rapamycin in humans leads to intracellular mTOR inhibition. The molecule’s ability to pass through cell membranes , likely facilitated by its high lipophilicity (logP estimated to be 4.3), supports its passage across the BBB despite its size .
After oral administration, detectable levels of rapamycin have been found in the brains of rodents [49, 50], and a large number of studies show clear effects in the central nervous system of animals [7]. Support for cerebral target engagement (i.e. mTOR inhibition) in humans comes from the use of rapamycin as a first-line treatment for the cerebral manifestations of TSC [51]. TSC is a genetic disorder that activates the mTOR pathway, leading to the growth of benign tumors in various organs, including the brain. Inhibition of mTOR with rapamycin analogues is the only approved pharmacological treatment of the disease, and the only feasible mechanism of action is mTOR inhibition in cells behind the BBB.
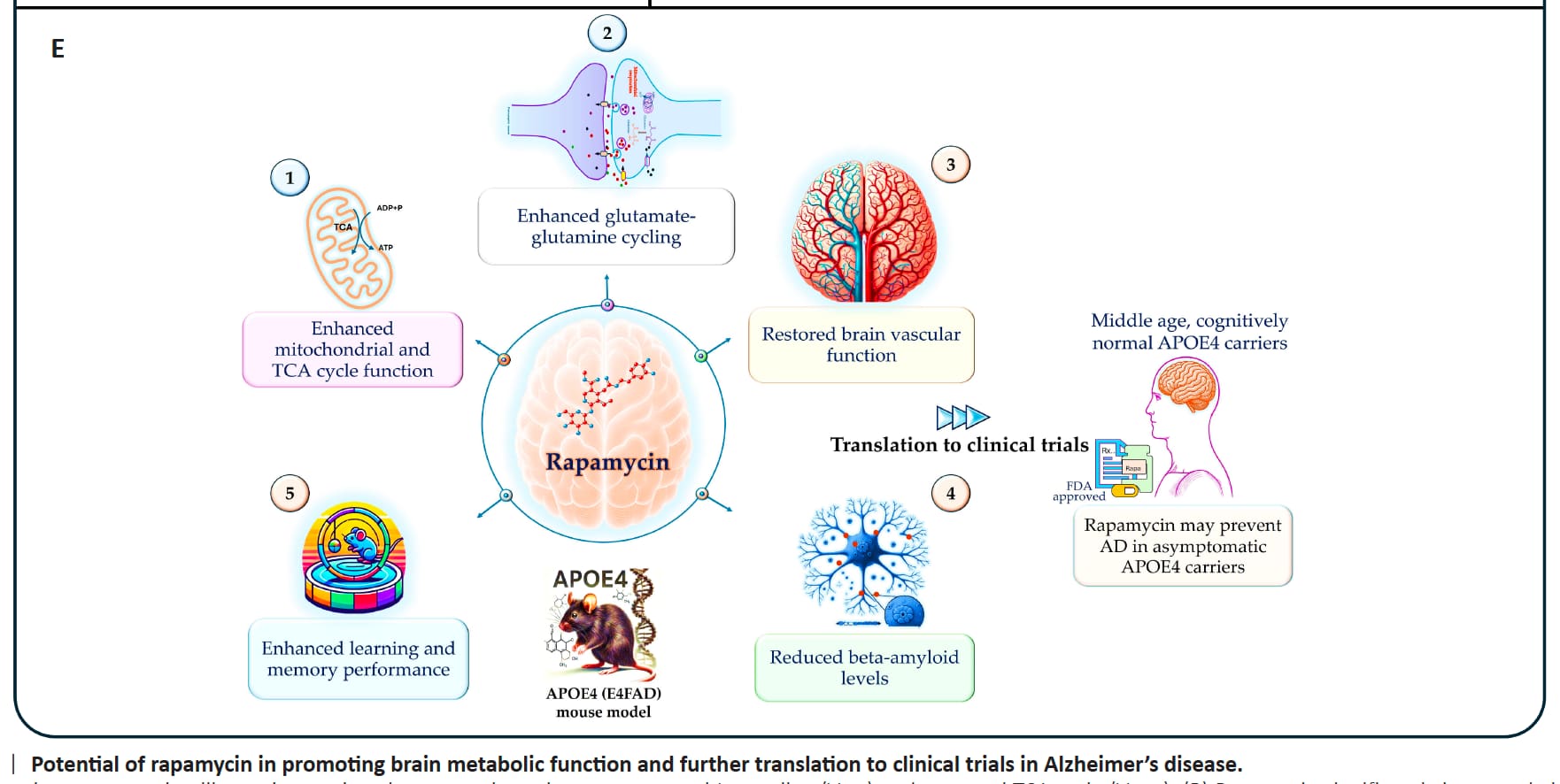
They also give three possible mechanisms of action of rapa: autophagy (mTOR inhibition), vasculoprotection (“Rapamycin has been shown to improve cerebral perfusion and BBB integrity in rodent models of AD, supporting the notion of the mTOR pathway as a potential target for brain vasculoprotection in AD”) and immunomodulation.
So hopefully, we’ll get an answer very soon (this year) about the effectiveness of 7 mg/week in AD. And next year about 1 mg/day.
Rapamycin causes a reduction in WBC via inhibition of mTORC1. This is arguably a side effect from the main mechanism. The reduction in WBC results in more infections which is one of the things that people don’t like.
Similarly Rapamycin causes hepatic insulin resistance via inhibition of mTORC1.
It will also reduce the production of stem cells.
I have not myself looked that much at mTORC2, but I think people should be aware that a lot of the negative effects of rapamycin come directly from its main mechanism of action and all that can be done is to adjust dosing strategies to obtain the greatest benefit for the least sensible harm.
As Matt pointed out on the podcast, it is such a pity that we cannot solve this once and for all. Probably need a cohort of one off one month of daily rapamycin, another with weekly dosing targeted to blood levels, and placebo with individuals all ApoE4/E4. The costs would be probably 3 MRIs including cerebral blood flow, Initial, 2 months, 12 months. In this fashion we’d see if cyclic was effective (and doing this for the whole 12 months), or whether a one time month of daily rapamycin has effects and sticking power (I’d propose the group on longer cyclic therapy will have further improvements on their 1 year scan as compared to the their 2 month scan, whereas I’d bet the group that did the 1 month then stopped will have some regression). Then we’d need the placebo to see the natural rate of progression of disease with no treatment.
These things are very complicated to arrange, but I’d bet that it wouldn’t be that hard to find 300 people willing to self fund their labs, 3 MRI’s who have ApoE4/E4.
I wonder if an organization like the Buck Institute would pursue this?