Without reading the paper I don’t think CS is at the core of the issue. The quoted text is not clear on whether it is the quantity of CS or the activity of CS that they are looking at. The activity will be linked with pyruvate influx.
Mechanical Forces Guide Axon Growth through the Nigrostriatal Pathway in an Organotypic Model
https://advanced.onlinelibrary.wiley.com/doi/10.1002/advs.202500400
“Reconstructing the nigrostriatal pathway is one of the major challenges in cell replacement therapies for Parkinson’s disease due to the lack of enabling technologies capable of guiding the reinnervation of dopaminergic precursors transplanted into the substantia nigra toward the striatum. This paper examines nano-pulling, as a technology to enable the remote manipulation of axonal growth.”
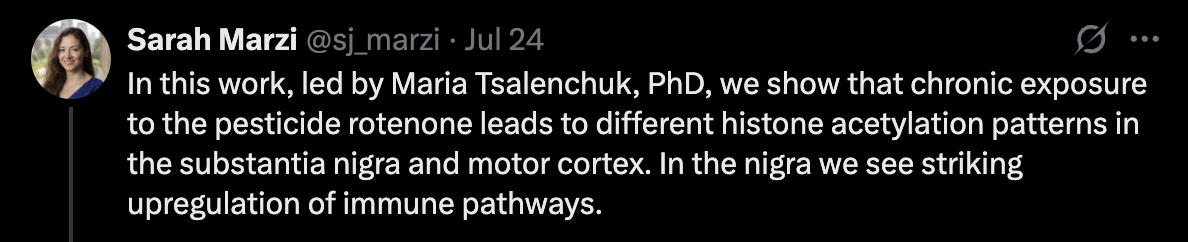
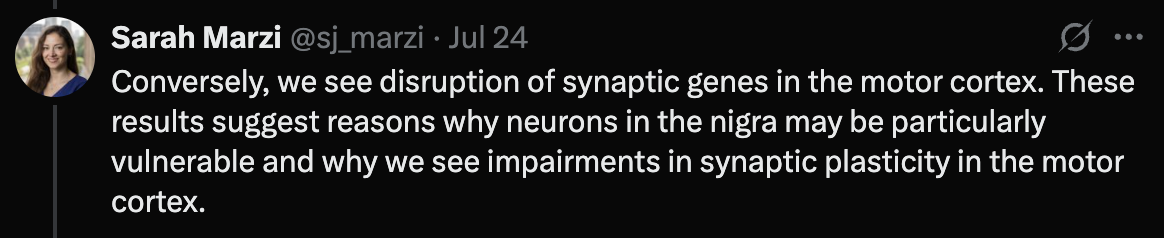
Pesticide exposure is increasingly recognized as a potential environmental factor in idiopathic Parkinson’s disease, though the molecular mechanisms remain unclear. This study explores how pesticide exposure alters gene regulation in key brain regions using the rotenone rat model. We performed H3K27ac ChIP-sequencing to profile active regulatory elements in the substantia nigra and motor cortex. Despite uniform complex I inhibition across regions, we observed region-specific epigenomic changes associated with rotenone exposure. RNA-sequencing confirmed transcriptomic alterations. We identified a strong, rotenone-induced immune response in the substantia nigra, including increased activity in the C1q complement pathway, suggesting immune involvement driven by regulatory mechanisms. In contrast, the cortex showed dysregulation of synaptic function at the gene regulatory level. Our results highlight a role for gene regulatory mechanisms potentially mediating the effects of pesticide exposure, driving region-specific functional responses in the brain that may contribute to the pathology and selective vulnerability that characterise Parkinson’s disease.
Pesticide exposure in rats changes epigenetic signatures in different brain regions (poke @John_Hemming).
1 Like
It hits the higher energy neurons first
UA and PD:
2 Likes
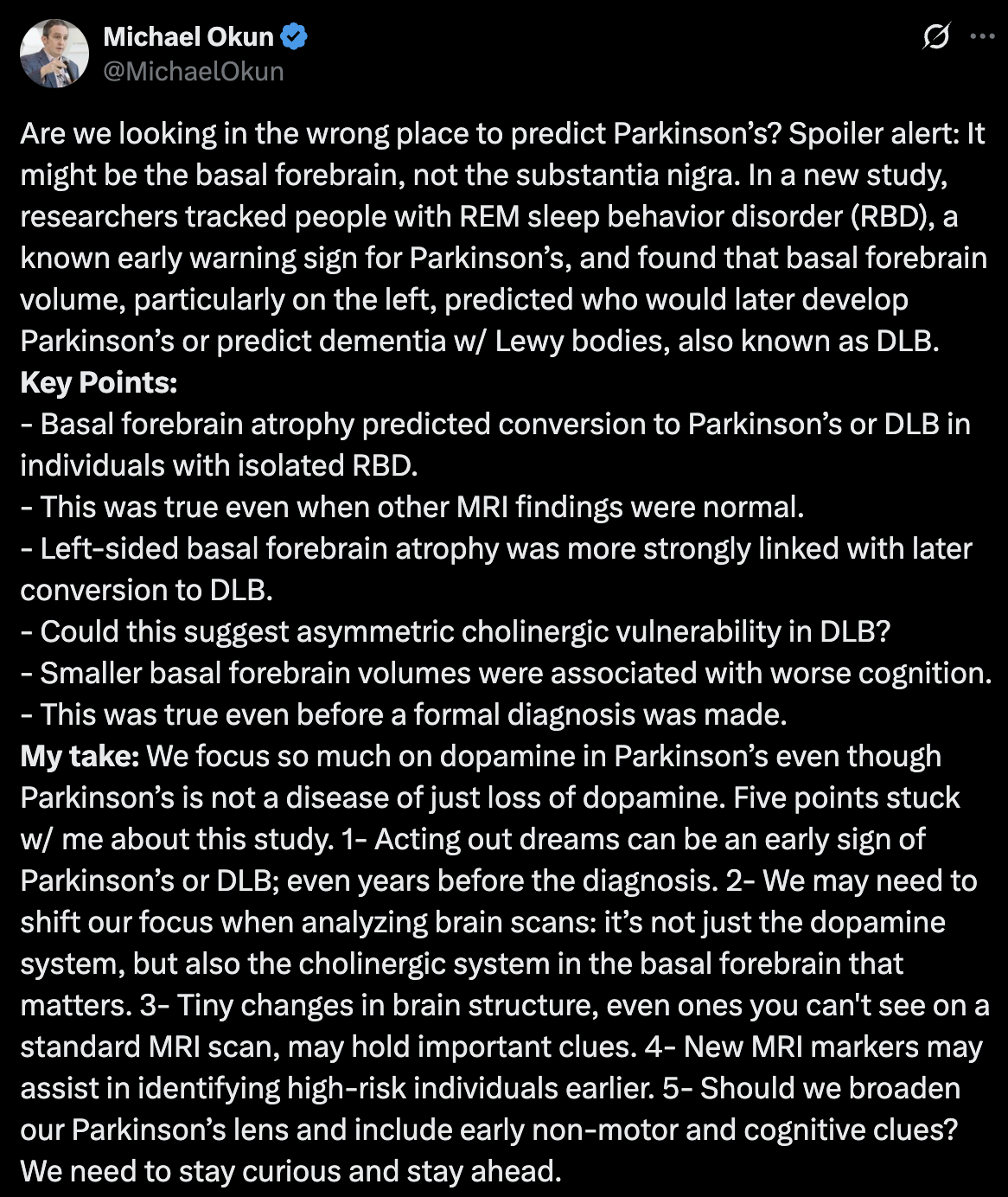
Basal Forebrain Volume Predicts Disease Conversion in Prodromal Synucleinopathy 2025
Thanks for sharing @John_Hemming
If rapa increases caudate and hippocampus volume, could it increase basal forebrain volume as well? Rapamycin as a preventive intervention for Alzheimer’s disease in APOE4 carriers: targeting brain metabolic and vascular restoration - #12 by adssx
5 Likes
One more datapoint in favor of our future Nobel prize @John_Hemming: Mitochondrial dysfunction-mediated metabolic remodeling of TCA cycle promotes Parkinson’s disease through inhibition of H3K4me3 demethylation 2025
(that being said, unfortunately it’s a group of weak Chinese universities + one Italian researcher)
Parkinson’s disease (PD), a neurodegenerative disorder caused by complex factors, is usually associated to mitochondrial dysfunctions but the links between such disorder and PD remain object of research. Here, we report that impaired mitochondrial quality control (MQC) system is a molecular basis of the mitochondrial dysfunction in PD and that tricarboxylic acid cycle (TCA cycle) disorder is the main feature of such mitochondrial dysfunction. Multi-omics analysis revealed that MDH2, OGDHL and IDH3G enzymes are bottlenecks in the enzymatic reactions of the TCA cycle in PD. Mechanistically, the abnormal α-KG/fumarate ratio caused by the TCA cycle bottleneck inhibits histone H3K4me3 demethylation and further enhances the expression of alpha-synuclein (SNCA), which may promote PD at an early stage. On these bases, we proposed a number of PD therapeutic strategies targeting mitochondria and histone methylation modifications, which proved to be effective in in vitro or in vivo models, especially citrate supplementation, in restoring normal TCA cycle enzymatic reactions. Taken together, our work highlights the non-negligible regulatory role of “mitochondrial-nuclear” communication in PD and provides important insights for the development of PD therapeutic strategies.
Citrate exhibits neuroprotective effects by correcting the abnormal α-KG/Fumarate ratio in PD
Based on the above results, we sought to find a natural supplement to correct the abnormal TCA cycle in PD. Given the extraordinary potential of citrate supplementation in improving cognitive ability, we constructed a subacute PD mouse model using MPTP and supplemented citrate through drinking water (Fig. 6A), which maximally simulated the dietary intake of natural supplements under physiological conditions [21]. Although continuous intraperitoneal injection of MPTP during model construction affected the food intake of mice, and this effect was reflected in changes in mouse body weight, the weight difference became no longer significant in the later stages of the model construction (Fig. 6B, C). During the establishment of the model, the water intake of mice was not affected, which ensured the stability of citrate supplementation (Fig. 6D). As expected, dietary citrate supplementation did not show systemic toxicity, while significantly increasing serum and midbrain citrate levels, confirming the safety and effectiveness of the citrate supplementation model, especially that citrate can cross the blood-brain barrier (BBB) and enter the midbrain (Fig. 6E, F). To evaluate the effect of citrate on motor dysfunction in the subacute PD model, we tested the motor ability and coordination ability of the model mice by behavioral tests. Compared with MPTP-treated mice, citrate supplementation reduced the time mice spent on the pole and increased the grasping time of mice on the inverted grid (Fig. 6G, H), indicating that citrate supplementation alleviated motor impairment in PD mice. Importantly, citrate supplementation restored the impaired tyrosine hydroxylase (TH; DaN marker) protein expression in the SN of PD mice and reduced MPTP-induced SNCA accumulation in the midbrain (Fig. 6I–K).
Currently, about the TCA cycle, supplementation of multiple metabolites including isocitrate [36] and α-KG [37] has been reported to show neuroprotective effects in PD. Based on the metabolic bottleneck of the TCA cycle reported here, we propose citrate as a potential metabolite for the treatment of PD. Actually, citrate can cross the BBB and shows good prospects in improving memory and treating Alzheimer’s disease [38,39,40]. At the same time, citrate, as α-KG precursor, acts as a metabolic supplement to help increase α-KG levels. More importantly, citrate can also act as a metabolic activator to enhance the activity of MDH2 in a high malate environment, promoting the conversion of fumarate metabolite malate to oxaloacetate [41], which reduces the accumulation of its substrate fumarate. Taken together, the multiple effects of citrate help reduce the α-KG/Fumarate ratio and correct abnormal TCA cycle flux, making it a very promising natural candidate for the treatment of PD. Previous reports have highlighted SNCA accumulation as an upstream event that triggers mitochondrial damage [42]. Here, our work emphasizes mitochondrial damage as an early factor in the pathogenesis of PD, and SNCA accumulation as a downstream molecular event that is finely regulated by α-KG/Fumarate ratio and H3K4me3 levels. These works reflect the complex crosstalk in the pathogenesis of PD and provide a more comprehensive perspective for the development of therapeutic strategies.
Briefly, mice (8 weeks old) received 12 days of daily drinking water containing citrate (Sigma; 1% w/v) and intraperitoneal injection (i. p.) of MPTP (MedChemExpress, HY-15608; 30 mg/kg body weight) or vehicle treatment for 8th to 12th days; the behavioral teste and sampling were performed three days after the last injection. Citrate was dissolved in drinking water, with pH adjusted to 7.3–7.4 by addition of sodium hydroxide.
They used the same dose as the paper Dietary citrate supplementation enhances longevity, metabolic health, and memory performance through promoting ketogenesis, which, according to ChatGPT, is equivalent to 8–10 g/day for a 70-kg human.
5 Likes
Thanks for this.
I take about 20g a day. I was this morning 82.2 kg.
Searching the paper there appears to be no mention of acetyl-CoA although there is a mention of acetylation. Hence I don’t think they have the mechanism right.
Still my citrate mix has now been mixed and is sitting in the factory to go to Amazon. I just need to sort out process.
5 Likes
Chinese preprint: Regulation of mitochondrial dynamics and function by MT1 melatonin receptor in Parkinson’s disease 2025
Here, we found the expressions of PINK1, and Parkin were decreased with MT1 deficits in vitro but not in vitro. The discrepancies between in vitro and in vivo models are probably because of the complex physiological conditions in the central nervous system, such as the interactions and signaling among neurons and glial cells. This effect is not similar to melatonin, which reported to be neuroprotective in PD by mitophagy augment [56]. Mitophagy is a selective autophagic removal process of damaged mitochondria. Since exacerbated LC3II/LC3I and P62 accumulation were observed in MT1 depleted PD mice, it is reasonable to speculate the autophagy of aggregates was also inhibited. Although we didn’t observe the TH loss in striatum and motor abnormality by MT1 knockout, the alteration of LC3II/LC3I ratio and P62 accumulation were found. This indicates the absence of MT1 may increase the susceptibility of PD occurrence through autophagy inhibition but is not the key etiological factor.
So melatonin “not the key etiological factor” @John_Hemming?
That’s the absence of a receptor not melatonin itself.
“Here, we found the expressions of PINK1, and Parkin were decreased with MT1 deficits in vitro but not in vitro.”
For the sake of clarity, this should be corrected, which is ‘in vivo’?
1 Like
Looking at the original PDF it is a typo in the original PDF.
Dr. Greger is at it again, never missing an opportunity to promote WFPB.
The Role Meat May Play in Triggering Parkinson’s Disease (Dr. Greger)

1 Like
I liked this one more:
Are pawpaws safe to eat? Pawpaw fruits, like soursop, guanabana, sweetsop, sugar apple, cherimoya, and custard-apple, contain neurotoxins that may cause a neurodegenerative disease.

And the vegan version of Chris Masterjohn responds:

2 Likes
Mitochondrial damage triggers the concerted degradation of negative regulators of neuronal autophagy 2025
Here, we demonstrate that in response to mitochondrial damage in neurons, MTMR5, MTMR2 and Rubicon undergo concerted degradation in a graded manner, independent of Pink1/Parkin activity. Upon mitochondrial stress, we find that Rubicon is ubiquitinated and targeted to the proteasome for degradation; MTMR2 and MTMR5 are also ubiquitinated in response to mitochondrial stress, but their degradation involves both the proteasome and calcium-dependent proteolysis. We term the selective degradation of these proteins in response to mitochondrial damage as the Mitophagic Stress Response (MitoSR), and hypothesize that this response accelerates mitophagic flux by degrading the negative regulators of autophagy. Consistent with recent findings that MTMR5/MTMR2 negatively regulate autophagosome biogenesis48, we find that loss of this myotubularin complex enhances mitochondrial engulfment in response to oxidative damage in neurons. In contrast, under basal conditions, Rubicon is recruited to neuronal lysosomes via RAB7, blocking lysosomal function and thereby inhibiting autophagosome maturation. We find that targeted depletion of these negative regulators significantly increases mitochondrial turnover in neurons under both basal conditions and upon induction of mild oxidative stress. Thus, we propose that therapeutic interventions directly targeting negative regulators of autophagy may promote clearance of damaged mitochondria in patients suffering from neurodegenerative diseases such as PD and ALS, where mitophagy is compromised.
1 Like
In the end if the mitochondria are not functioning well enough the cell cannot produce the proteins for autophagy.
3 Likes
There’s an ongoing trial of MK7 in PD but I’m afraid we might never get the results. Meanwhile, mechanistic studies look good: Menaquinone-7 - an interesting molecule to power up the mitochondria - #80 by adssx
1 Like
Mendelian randomization preprint from McGill University: Investigating the genetic relationship between vitamin B12 deficiency and Parkinson’s disease 2025
Our analysis showed no associations between common variants of genes crucial in B12 metabolism and PD. Pathway PRS identified nominal association between B12-related genes and PD (OR = 1.061, 95% CI: 1.004–1.121, p = 0.038), which did not survive Bonferroni correction. In the rare variants analysis, we identified a significant association between variants with high CADD scores in the CUBN gene (P=6.07E-05; Pfdr=0.005) in the AMP-PD cohort, driven by the benign variant p.G3114S (OR=3.3; p=3.56E-05); however, this was not validated in the meta-analysis. We did not identify a potentially causal relationship between vitamin B12 levels and the risk, age-at-onset, or progression of PD. Additionally, no genetic correlation was observed between vitamin B12 and PD risk or age-at-onset GWASs.
Confirmed by two previous MR studies:
As for PD, the IVW method suggested that the Zinc (Zn) levels was significantly associated with PD (OR = 1.107, 95% CI 1.013–1.211; p = 0.025), which is consistent with results from the weighted median analyses. Moreover, the results remained consistent and robust in the sensitivity analysis. However, there were no significant associations of catalase, glutathione peroxidases, superoxide dismutase, vitamin A, vitamin C, vitamin E, vitamin B12, folate, copper, or iron with PD. As for OS, our reverse MR analysis also did not support a causal effect of liability to PD on OS.
In addition, we did not observe any evidence that the circulating levels of vitamin B6, vitamin B12 and folate acid affected the risk of PD or age at onset of PD. Our findings implied that lowering homocysteine levels through vitamin B6, vitamin B12 or folate acid supplementation may not be clinically helpful in preventing PD or delaying the age at PD onset.
On the other hand, this abstract found: Higher Serum Vitamin B6 and B12 Levels Associated with Parkinson’s Disease Incidence (P2-5.003) 2025
“2,757 participants (mean age 59.7[SD, 12.4], 45.8% men) followed on average for 19.4[SD, 6.1] years were included. With surveillance beginning 5 years after entry, there were 40 incident PD cases. The highest tertiles of serum B12 (HR 2.27 [95% CI 1.04, 4.95], p=0.040) and B6 (HR 2.96 [1.24, 7.07], p=0.015) levels were associated with incident PD, but not vitamin intake. Higher serum vitamin levels were not associated with incident dementia or Alzheimer’s disease. Higher dietary intake of vitamins was not associated with incident PD.”
So B12 supplementation is irrelevant in PD? (poke @DrFraser)
4 Likes
The way this is presented, one would think that pre-existing B12 levels being high were a risk for PD, but if you happen to be taking some supplements, that didn’t worsen things - which mechanistically is interesting and a bit counter-intuitive. However, supplementation isn’t always the same thing as lifestyle or other genetics resulting in a higher level.
I very much appreciate the laser focus on PD … and overall, I think exercise, including things with a lot of balance and aerobic activity (pickleball for us elders), some weight training, 40 hz devices and GLP-1s are among the the things to highly consider (I know there are more).
But in conjunction with this, if one has a Homocysteine of 35 … I’d still treat it - but for other reasons, just not in the delusion that this will impact PD.
Neurodegeneration will remain a tough nut to crack.
4 Likes
I wonder if SS 31 / Elamipretide would help with this?
I keep getting delayed in my experiment with this peptide, been quite busy the past couple of weeks
https://www.sciencedirect.com/science/article/pii/S0753332225002501
Contemporary insights into elamipretide’s mitochondrial mechanism of action and therapeutic effects
Highlights
• Mitochondria electron transport system (ETS) produces essential cellular energy. • ETS is located on cardiolipin (CL)-rich cristae of inner mitochondrial (MITO) membrane. • In disease, elamipretide binds to CL, improving MITO structure, function and dynamics. • In animals, elamipretide improves MITO function in cardiac and skeletal myopathies. • In humans, elamipretide improves symptoms of Barth syndrome myopathy
1 Like