Yes, discussed here and there. (Let’s keep this thread about everolimus)
3 Likes
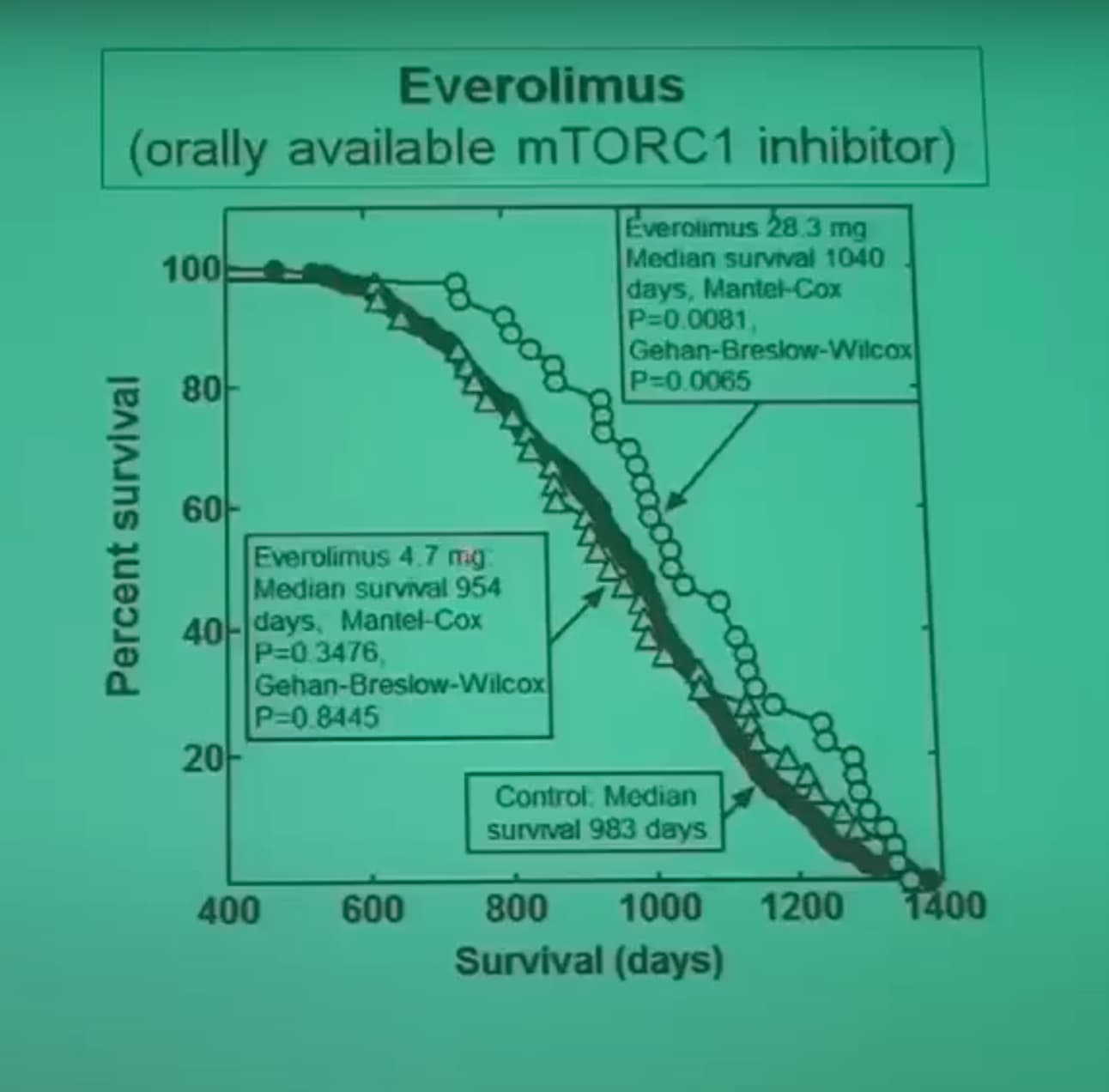
Median survival:
- Control: 983 days
- Everolimus 4.7 mg: 954 days (-3%, p=0.35)
- Everolimus 28.3 mg: 1040 (+6%, p=0.01)
How do these doses convert to human doses?
Comparison to sirolimus (DrugAge):
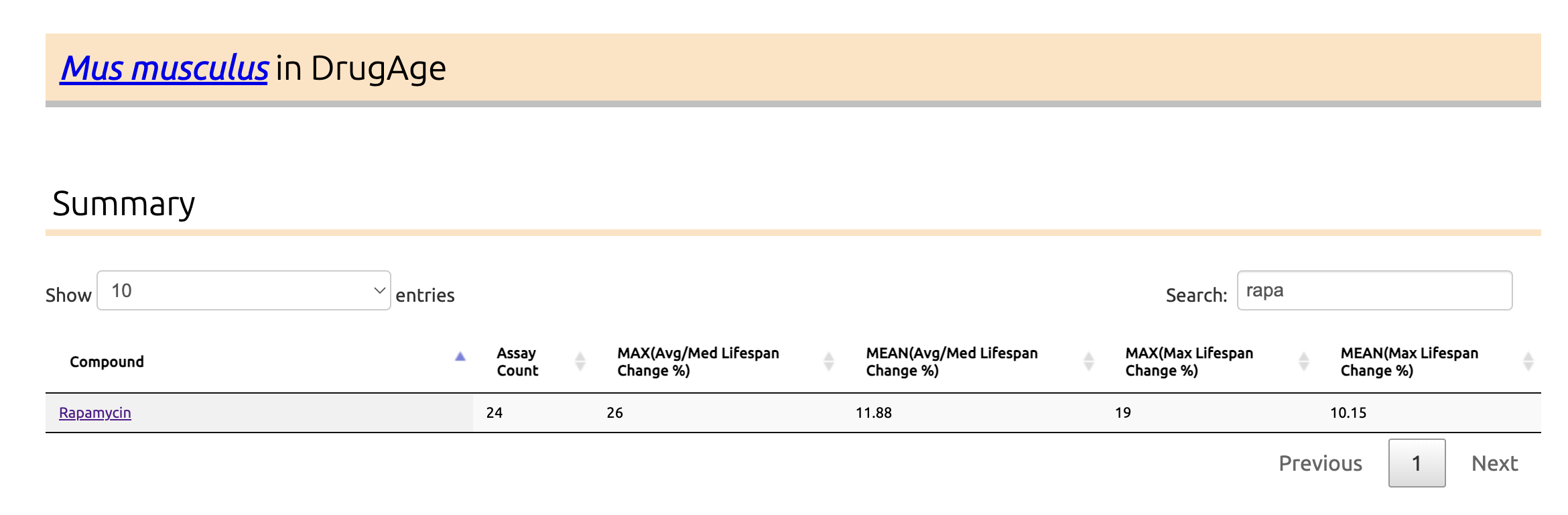
So clearly inferior?
3 Likes
Looks like a really high dose if that is per mouse rather than per kilogram of mouse.
I don’t think you can read much into this.
I would assume that beyond the issue of short life and dosing the effect of inhibiting mTOR is much the same.
I am personally sticking with Rapamycin because it does what I want it to do, but at the moment I don’t want to take it until I have resolved the issue with my low WBC. I think I have resolved the issue, but I don’t have test results to prove this.
3 Likes
Wow! That’s a pathetically small effect! I had never gotten a clear shot of the numbers. I had assumed that the effects of rapa and everolimus would be quite similar; this is effectively a null result ![]() .
.
Good question. It seems unlikely it means mg/kg mouse (why would they start with double the rapa dose and then go to 10x of it?), but the other alternatives also seem unlikely (28.3 mg per mouse (definitely not), or 28.3 mg/kg food).
I’d have to say so!
3 Likes
OK so from a lifespan point of view, everolimus seems useless (vs sirolimus).
The question of the potentially better BBB crossing remains. However, sirolimus seems beneficial according to this trial: Rapamycin as a preventive intervention for Alzheimer’s disease in APOE4 carriers: targeting brain metabolic and vascular restoration
1 Like
I am not myself sure that everolimus would be necessarily worse than sirolimus. My reason for concentrating on Rapamycin is that we have more knowledge about its potential risks and hence if I take a high dose I am more likely to be aware of any negative consequences and how to handle them.
Also there is only so much experimentation that can be done. My experiments take multiple weeks at times and I really cannot slot in an alternative to rapamycin that has much the same mechanism.
I am also not persuaded of the argument that rapamycin does not cross the BBB. It probably crosses at a lower rate.
I don’t think that any one molecule (citrate, rapamycin, menaquinone-7, melatonin) is the solution to repairing the mitochondrial dna. I think a combination in a cyclical manner is going to produce the optimal results.
2 Likes
To revive this thread, wanted to check if there is any new evidence to say that Everolimus is a viable option for longevity gains. Am seeing more comments about its usage in some biohacking circles due to shorter half life and lower AE profile, but the last discussion on this thread seems to indicate it is a dud for longevity.
1 Like
I wouldn’t say it’s a dud at all. I would disagree with @adssx on his assessment above.
I still expect the effect is likely very similar to rapamycin. The key unresolved issue is the exact dosing requirement to get similar results. That one datapoint that was posted a few posts back is only one study. Everolimus has rarely been studied for longevity… because it’s so similar to rapamycin (so most scientists expect it to have very similar lifespan enhancing results).
I have a good stash of Everolimus because of this. Given that it comes in 10mg tablets, it’s a little easier to order larger quantities from India or other locales.
But I tend to default to rapamycin use because it’s the compound that has the most research behind it, and is easy to get, and I started on it 6 years ago. And, I wouldn’t say I’m so confident in the everlimus effectiveness that I’d give up Rapamycin for it. There is no obvious reason to move to Everolimus really, at this point. Rapamycin is well validated, inexpensive and easy to get. Everolimus probably works equally well at some dosing, but why risk it?
2 Likes
Various doses of sirolimus extended lifespan. Various doses of everolimus did not. And no one seems to study everolimus anymore. So clearly everolimus is shit (until proven otherwise!).
2 Likes
Its shorter half life may actually be an issue. What we don’t know is how long mTOR needs to be inhibited in order to kick things off. It could be something like a few hours. I am sticking with SIro.
1 Like
chatGPT says:
Here’s a compact set of tables for the key everolimus / lifespan or survival experiments by species.
1. C. elegans (worms)
| Species / strain | Health context | Study (year) | Everolimus regimen | Lifespan effect | Notes |
|---|---|---|---|---|---|
| C. elegans N2 (wild-type) | Normal aging | Demirel et al., 2024, Russian J. Nematology (russjnematology.com) | 0.01–10 nM in agar throughout life | Mean lifespan ↑ ~40–53% across 0.01–5 nM; slightly less at 10 nM | Very large extension; non-monotonic dose–response; also tested rapamycin & temsirolimus. |
| C. elegans lin-35 mutant | Tumour-suppressor mutant (Rb ortholog) | Demirel et al., 2024 (russjnematology.com) | Same doses as above | Mean lifespan ↑ ~2–31% depending on dose | Effect smaller and more variable than in N2; still generally positive. |
| C. elegans N2 | Normal aging | Zhang et al., 2024, J Gerontol A (PubMed) | Liposome-delivered everolimus at several doses during adulthood | Pooled data: ~+6.8% mean lifespan, not statistically significant (p ≈ 0.075) | In same study, rapamycin & temsirolimus showed clearer, significant lifespan extension; everolimus weaker. |
2. Drosophila melanogaster (flies)
| Species / strain | Health context | Study (year) | Everolimus regimen | Lifespan / survival effect | Notes |
|---|---|---|---|---|---|
| Male D. melanogaster | Normal aging | Spindler et al., 2012, PLoS ONE (PMC) | Food containing 3 mM everolimus (library screen) | Male lifespan ↑ ~17% | Identified everolimus as a positive hit in a kinase-inhibitor screen; baseline lifespan short (screen conditions). |
| Male D. melanogaster (reviewed) | Normal aging | dos Santos et al., 2024 review on pharmacology of aging in flies (PMC) | Various (summarising prior work) | Confirms everolimus extends fly lifespan in at least some conditions | Review categorises everolimus among clinically used drugs that extend fly lifespan; detailed dose data from Spindler. |
3. Mice – survival / “lifespan” in disease models
(There is still no classic “healthy mouse lifespan” everolimus study analogous to Harrison 2009 for rapamycin.)
| Model / genotype | Health context | Study (year) | Everolimus regimen | Survival / lifespan effect | Notes |
|---|---|---|---|---|---|
| EGFR-mutant transgenic mice (lung tumours) | Oncogene-driven lung cancer | Yasugi et al., 2014 (PubMed) | Everolimus (RAD001) given chronically after tumour induction | Median survival: 31.2 → 58.0 weeks (~+86%, p < 0.001) | Strong prolongation of survival; pS6 down, angiogenesis suppressed; little evidence of apoptosis/autophagy change. |
| TgMISIIR-TAg ovarian cancer mice | Transgenic ovarian carcinoma | Mabuchi et al., 2007, Cancer Res (PubMed) | RAD001 treatment in transgenic females | Markedly delayed tumour onset; tumour burden ↓ ~84%; improved tumour-free survival | Ascites & peritoneal dissemination in 21% of treated vs 74% controls; survival benefit via delayed aggressive disease. |
| Eµ-Myc transgenic mice | B-cell lymphoma / leukemia model | Wall et al., 2013, Cancer Discov (PMC) | Everolimus as prevention and therapy | Strongly prolonged overall survival; in one cohort median survival 73 days (placebo) vs not reached (everolimus) | Everolimus clears premalignant B cells, restores normal B-cell differentiation, induces p53-linked senescence; robust delay of lymphoma onset. |
| Lmna H222P/H222P mice | Cardiomyopathy (cardiolaminopathy) | Wu et al., 2024, Circ: Heart Failure (PubMed) | Everolimus started after onset of heart failure | Median survival ↑ 9% vs placebo (p ≈ 0.035) | Also improved cardiac structure/function; reactivated autophagy; modest glucose intolerance as side effect. |
| Ovarian cancer xenografts & related models | Advanced ovarian cancer | Mabuchi et al. plus later summaries (e.g. Guo 2016; Blagosklonny 2023 review) (PubMed) | Everolimus alone or with other therapy | Delayed tumour onset, reduced tumour burden and intra-abdominal spread; prolonged survival in several models | Used more as an anti-cancer drug; survival benefits are disease-specific, not general aging models. |
4. Humans – aging-related endpoints (no lifespan data)
| Population | Health context | Study (year) | Everolimus regimen | “Lifespan-adjacent” outcome | Notes |
|---|---|---|---|---|---|
| Adults ≥65 yrs (healthy) | Immunosenescence | Mannick et al., 2014, Sci. Transl. Med. (PubMed) | RAD001 0.5 mg/day or 5 mg/week for 6 weeks vs placebo | ~20% improvement in influenza vaccine response; ↓ PD-1⁺ T-cells; no lifespan follow-up | First “aging” oriented RAD001 trial in humans; short-term immune functional data only. |
| Adults ≥65 yrs (ongoing / planned trials) | Aging biomarkers, function | Mannick et al., various; summarized in 2021 & 2024 reviews (PMC) | Low-dose everolimus alone or in combination with other mTOR inhibitors | Endpoints: immune, inflammatory, functional; no mortality endpoints | Designed to explore safety, dosing and biomarker changes rather than hard survival. |
| Patients with cancers, TSC, etc. | Disease treatment | Multiple RCTs across indications (neuroendocrine tumours, renal cell cancer, TSC, etc.) (MD Anderson Cancer Center) | Therapeutic doses (e.g. 5–10 mg/day) | Improved progression-free survival / disease outcomes in specific diseases | These are oncology / transplant trials; they don’t speak to “normal aging lifespan” in otherwise healthy humans. |
Quick overall read
- Invertebrates: Clear evidence that everolimus can extend lifespan, with effect sizes ranging from non-significant ~7% up to ~50% depending on strain, dosing, and protocol.(russjnematology.com)
- Mice: Strong survival extension in multiple disease-prone models (cancers, cardiomyopathy), but no clean “healthy mouse lifespan” study yet.(PubMed)
- Humans: Only short-term functional improvements (especially immune function in older adults); no direct lifespan/healthspan endpoints yet.(PubMed)
If you’d like, I can next add a second table comparing everolimus vs rapamycin vs temsirolimus in the same experiments (e.g. Demirel & Zhang, worm and fly data) to get a clearer sense of relative potency.
2 Likes
These are cancer models: irrelevant.
Longevity studies for everolimus are here:
3 Likes
I took rapamycin for over 2 years and didn’t see any results. I saw a recent study that said it only worked for 75% of people, so I just switched to everolimus, because it is supposed to cross the blood/brain barrier better. It is much more expensive and harder to get, but my doctor found it from Mark Cuban’s pharmacy for about $60 for 30. It was $2,500 from Walgreens! Today was day 6. I’m also taking Lithium and b vitamins but eliminated most of the other supplements I had been taking in case they interfered with the everolimus. I will add them back one at a time eventually. I don’t know if I will live longer, but I really need to feel better–I have adrenal POTS among other things.
5 Likes
Thank you for your report. Keep us posted on any benefits (or not) of your new regiment. Best of luck!
3 Likes
In the 2014 trials where everolimus increased immune function they found 5mg weekly worked but 20mg did not if I remember correctly. From everything I read so far a dosing conversion factor of around 1.3-1.5x seems to be ideal to account for everolimus’ higher bioavailability.
So 5mg everolimus should be similar to 7-8mg rapamycin but everolimus will always achieve a lower trough by the end of the week but some rapamycin will still remain at day 7 so its hard to find a true equivalent dose
2 Likes
That doesn’t mean it isn’t working. A huge problem with interventions that slow down aging is that it takes so long to know if they are working. If you used some intervention that actually worked and slows down aging by say 5%, you wouldn’t notice anything in 2 years. You would have to wait 10 years and have a twin that acts as a control that doesn’t take it to maybe notice results in 10 years. We unfortunately don’t have markers of biological age that are good enough to detect whether something is slowing down aging or not in humans.
4 Likes
I will give my standard reply: “If it ain’t broke, you can’t fix it!” So, everolimus would be the same in that regard.
Is there something specific you expected from sirolimus?
I have been taking it for 4+ years at higher-than-average weekly doses, and it has solved a multitude of old-age problems. (I am ~85 years old).
I agree that everolimus may be a better option for life extensions, but the jury is still out. I am not sure what benefits everolimus crossing the BBB would have, as my subjective view is that my brain is still fine.
I posed a rather lengthy query to paid versions of ChatGPT 5 and Gemini, basically asking to compare everolimus with sirolimus for life extension based on what is known. Dosage equivalents, blah blah blah.
The response was very lengthy, so I will just post a few relevant highlights. You can see the query and full responses in the links below. I prefer Gemini’s response.
Assessment: Is Everolimus a Superior Alternative for Life Extension?
- Strength of lifespan evidence
- Sirolimus (rapamycin) is, so far, the only drug consistently shown to extend lifespan in multiple mammalian studies (mice), across sexes, strains, and ages at treatment onset, with median lifespan increases often in the ~9–26% range and accompanying healthspan benefits. ScienceDirect+2OUP Academic+2
- Everolimus has robust anti-tumor and survival data in cancer-prone mice (e.g., Eμ-Myc lymphoma, APC^Min/+ models), but no published wild-type mouse lifespan program comparable to the rapamycin literature. Survival extension is usually framed as “delay of tumor progression” rather than “general lifespan extension.” AACR Journals+2ScienceDirect+2
- Current high-level reviews of mTOR inhibitors and aging repeatedly emphasize rapamycin as the agent with strong, reproducible mammalian longevity data, while positioning everolimus (and other rapalogs) as promising but under-tested in this specific context. lamminglab.medicine.wisc.edu+1
Everolimus (RAD001) has the best human immune-aging data: in older adults, low-dose regimens such as 0.5 mg/day or 5 mg once weekly for 6 weeks improved influenza vaccine responses (~20% better geometric mean titers) and reduced some infection endpoints, with acceptable short-term safety.
Similar “healthy-elderly immunosenescence” studies with sirolimus itself are fewer; most human sirolimus data come from transplant and rare disease populations, where doses and co-medications are very different from longevity practice.
However, transplant data broadly suggest that when adjusted to equivalent exposure, rapamycin and everolimus have very similar patterns of adverse effects (stomatitis, dyslipidemia, cytopenias, and infection risk), with modest differences between studies.
Some preclinical work suggests rapalogs (everolimus, temsirolimus) may produce less mTORC2-driven metabolic toxicity at certain schedules, but other data (and transplant experience) show broadly similar metabolic side-effect profiles when dosed to comparable efficacy. PubMed+2Nature+2
Blood–brain barrier and brain aging
- Both sirolimus and everolimus are lipophilic macrolides that do cross the blood–brain barrier, but CSF levels can be low and brain penetration is considered limited and heterogeneous. Nature+2Nature+2
- Everolimus is widely used in tuberous sclerosis and brain tumors, with evidence of central mTOR pathway inhibition, while rapamycin itself also has preclinical data showing CNS mTOR modulation. Cancer Care Ontario+2MDPI+2
- At the low weekly doses used for longevity (e.g., 5–8 mg sirolimus or ~5 mg everolimus), relative CNS exposure and functional impact are unknown, and no head-to-head cognitive-aging or neurodegeneration trials exist.
Overall judgment for someone on 6–8 mg once-weekly sirolimus
-
Evidence hierarchy:
- Sirolimus: strong mammalian lifespan data + substantial mechanistic and clinical experience.
Absorption and Bioavailability
Both drugs are substrates for the P-glycoprotein (P-gp) efflux pump and the Cytochrome P450 3A4 (CYP3A4) enzyme system in the intestinal enterocytes, which historically results in low and variable oral bioavailability.7 However, the structural modifications of Everolimus confer specific advantages.
Dosage Equivalence Scenarios
| Strategy | Sirolimus Dose | Everolimus Equivalent | Rationale |
|---|---|---|---|
| Direct Weight Match | 1 mg | 1 mg | Everolimus yields higher Peak, lower AUC. |
| Transplant (Trough) | 1 mg (Daily) | 1.5–2.0 mg (Daily) | Compensates for rapid clearance to keep immunity low. |
| Longevity (Pulse) | 6 mg (Weekly) | 8–10 mg (Weekly) | Ensures maximal autophagy trigger (Cmax) while utilizing rapid half-life for recovery. |
Is Everolimus a “Better” Option?
Affirmative, with qualifications regarding cost and evidence density. From a pharmacological perspective, Everolimus is the superior agent for “pulsed” dosing regimens. The primary criticism of weekly Sirolimus is its 62-hour half-life, which makes it a “dirty” pulse; significant drug remains in the system for the entire week, leading to potential chronic mTORC2 inhibition and metabolic derailment. Everolimus (28-hour half-life) allows for a kinetically “clean” pulse. It achieves a high Cmax to trigger autophagy and clears completely within 4–5 days, providing a physiological recovery window that Sirolimus cannot offer.
9.2 The Neuroprotective Verdict
For individuals prioritizing cognitive health, Everolimus is theoretically superior. Unlike Sirolimus, which may inhibit mitochondrial function in the brain, Everolimus has been shown to distribute into neuronal mitochondria and stimulate bioenergetics. Coupled with its ability to reduce neuroinflammation more effectively than Rapamycin in seizure models , it represents the more targeted choice for neuro-preservation.
My own take is that everolimus is probably superior for older people in that it seems to provide better anti-cancer protection and help for the aging brain.
Thanks to your post, I have been rethinking this and plan to give evrolimus a shot.
Both Zydus and Biocon of India produce everolimus, and it is available at reasonable prices from India, albeit more expensive than sirolimus.
As I said, the responses from both Gemini and ChatGPT 5 are several pages long.
You may read the complete reports from both. Here are the links:
Gemini: https://tinyurl.com/3w5ebkcb
ChatGPT5: https://tinyurl.com/37w36bd2
3 Likes
The idea I have been toying around with is doing a slightly smaller sirolimus than my usual weekly dose plus a compensatory everolimus (dose equivalent to bring you back to a full usual dose) as a kind of chaser. The idea would be to have roughly the same mTOR inhibition, but a small amount of everolimus crossing the BBB.
I haven’t done it yet, as I’m having major surgery soon and then will be off rapa for three months or so to make sure bone fusion is successful.
You may be interested in asking your favorite AI for feedback, though when I did so some time ago, AI (Gemini) was negative without actual data, the usual conservative response. Fact is there is very little actual data on combining the two. One idea in order to avoid possible complications would be to take them away from each other - the sirolimus dose and then the small everolimus a day or two days later to avoid interference in case that matters. Since everolimus has a shorter half life it shouldn’t accumulate and the trough preserved.
Just some ideas, obviously very speculative. Proceed at your own risk, do your research, not medical advice etc. YMMV.
2 Likes
It’s not like Everolimus crosses the BBB well. I’m not convinced there is biological significance between the two. I’m also suspect of comparing different studies because the dosages are not always equivalent, T1/2 are different and route of administration is often different. I think everolimus has been studied more because the companies want to make that claim. Both Sirolimus and everolimus cross the BBB a little. Several of the newer catalytic mtor inhibitors that block the ATP binding site (of both MTORC1 and MTORC2) cross the BBB quite well.
2 Likes