Dr. Ross Pelton on Tuesday, June 21, 2022. PEARL Webinar is one of the few experts addressing the issue of rising lipid levels. (I was directed to the webinar by"Agetron )
He suggests that if your cholesterol levels rise, your dose is too high and you should back off.
Symptoms of an overdose: anemia, low iron, elevated cholesterol and triglycerides levels.
Dosing and side effects at 25:50.
Since I have been dosing at rather high levels and my cholesterol has been much higher than my normal levels I think I will back off. Fortunately, I have blood tests taken over the years and just before taking rapamycin.
I didn’t actually recognize this as an adverse side effect when adjusting my dosage to the highest levels without adverse side effects.
This was a great webinar and covers several other anti-aging topics besides rapamycin.
This is a human imposed restriction…how does this “too high limit” prevent our ultimate goal, lifespan extension in humans? The innate laws of physics, biology, science, in this case, longevity extension, do not care about external limits. Clearly, if standard playbook dosing protocol causes a reduction in mortality via side effects, this obviously defeats the purpose.
This is a massive unknown gap in translation…the elephant in the room.
No, I am in the higher systemic and higher in the brain whilst minimizing side effects via hacking delivery method (s). Maybe there’s another paradigm for rapamycin to optimize human longevity?
I’m an engineer/inventor/citizen-scientist, I am intensely curious at re-appplying myself to leverage biological science (not my training) for optimal health benefit. But a realist by nature; the facts, known and UNKNOWN, help ground my thinking.
But I agree with you, optimists do live longer. So here’s to rapamycin, the magic bullet!
I believe that he’s a pharmacist and may have a different perspective. I haven’t listened to the podcast but if he’s generalizing like that and not taking into account the details, then I can’t agree.
First off, the Mendelian randomized study that I posted showed no significant risk for CAD from lipids if elevated after the age of 70.
What does he define as an elevation? To what extent and which lipid subgroup?
A drop in iron may be beneficial. How low is he talking about?
He may be correct but is there Any human study to support this advice?
For Rapamycin, even Dr B says in a few of his papers that if lipids rise, take a statin. Dr B also says glucose should not rise but if it does, it’s benevolent, but he demurs and says just take metformin.
This is standard lipids (and glucose) playbook…extended to a rapamcyin side effect, conventional cardiovascular disease management. And we’ve already thrashed this subject for some time as to it’s need/efficacy.
Your questioning the need for a statin is still valid, but you also come from a “different perspective” and bias.
We do not know if Rapamycin alters the normal CVD dynamics. Two cardiologists might possibly disagree…one who goes by AMA playbook vs one who looks at the entire risk profile, including say CAC.
By different perspective, I merely mean that it’s not unusual for doctors and pharmacists to view certain things differently. Not that one is necessarily right. In fact, I’m usually wrong.
Agreed, but I think your true inquiry is whether the perspective is grounded in some “rapamcyin” specific attribute or knowledge, or just standard lipids playbook of which you are completely versed.
I will venture to say it’s the latter…standard lipids playbook because we truly do not know.
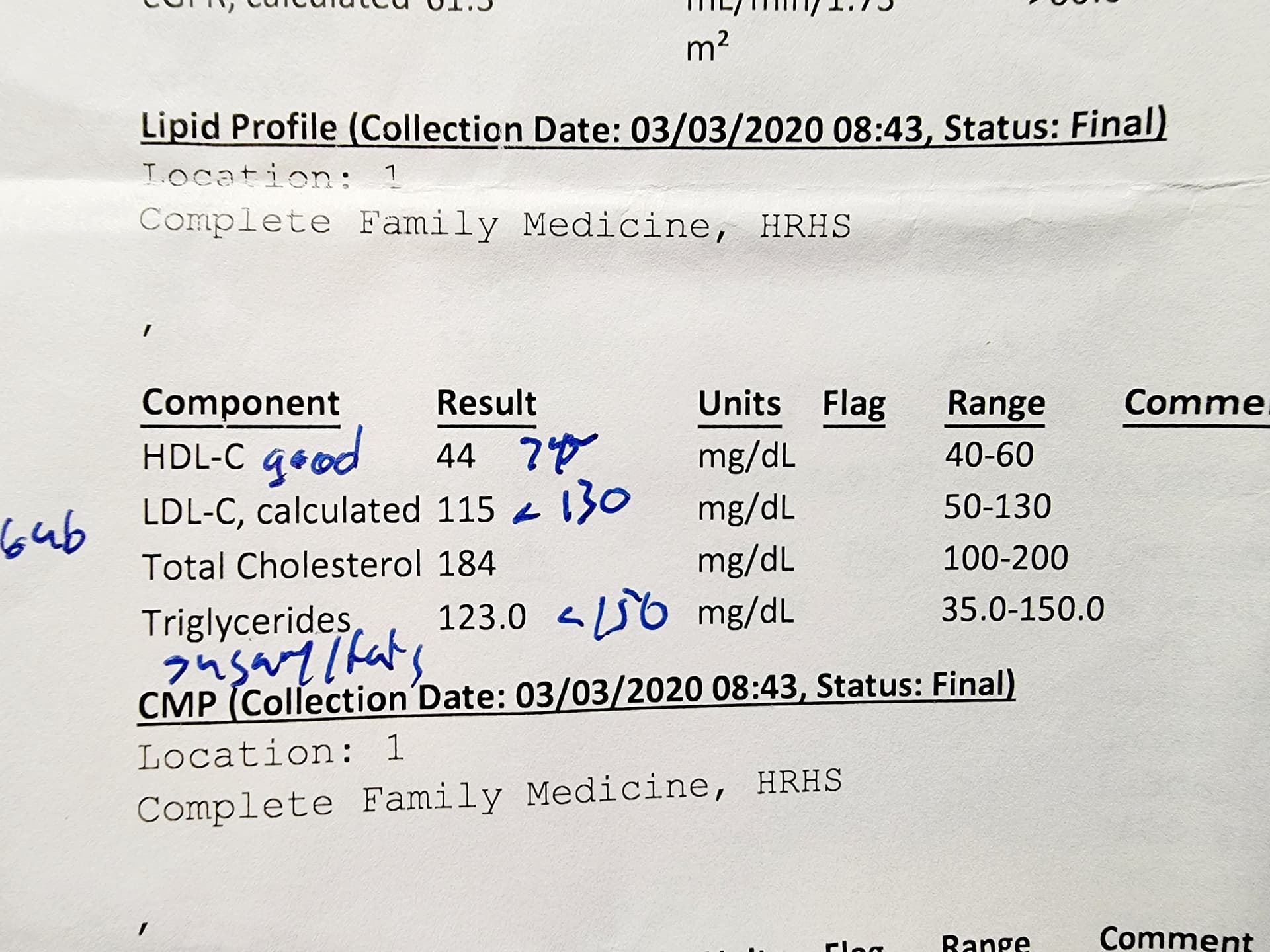
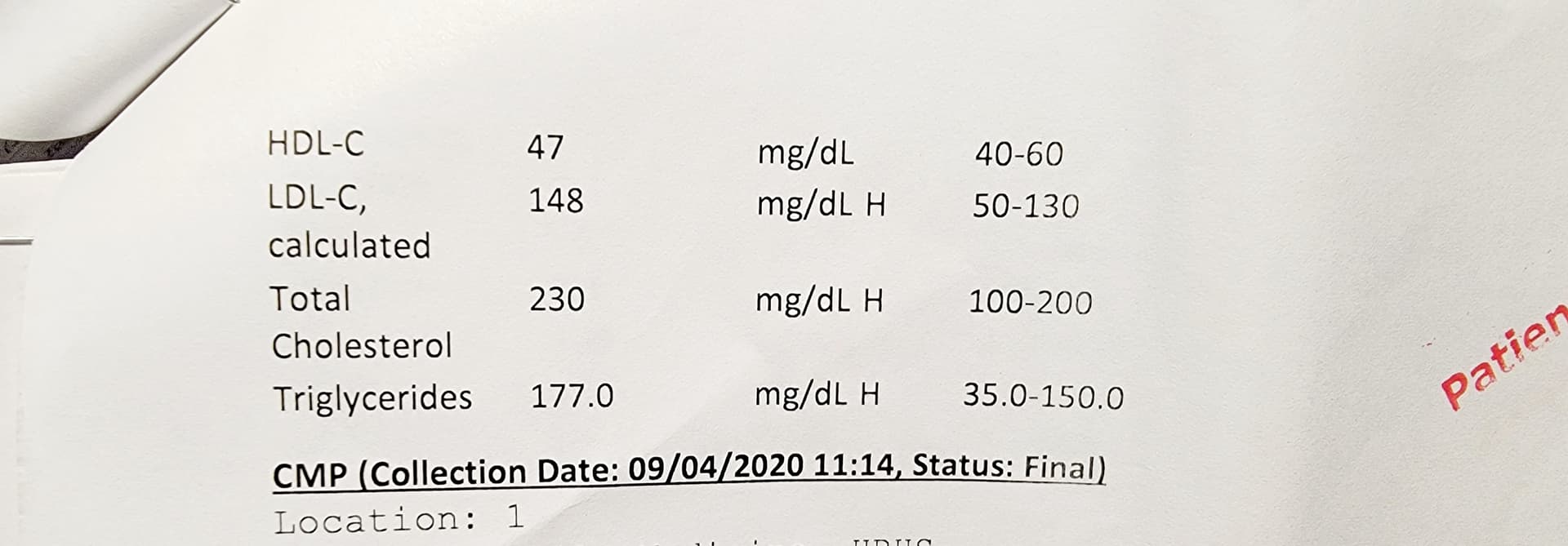
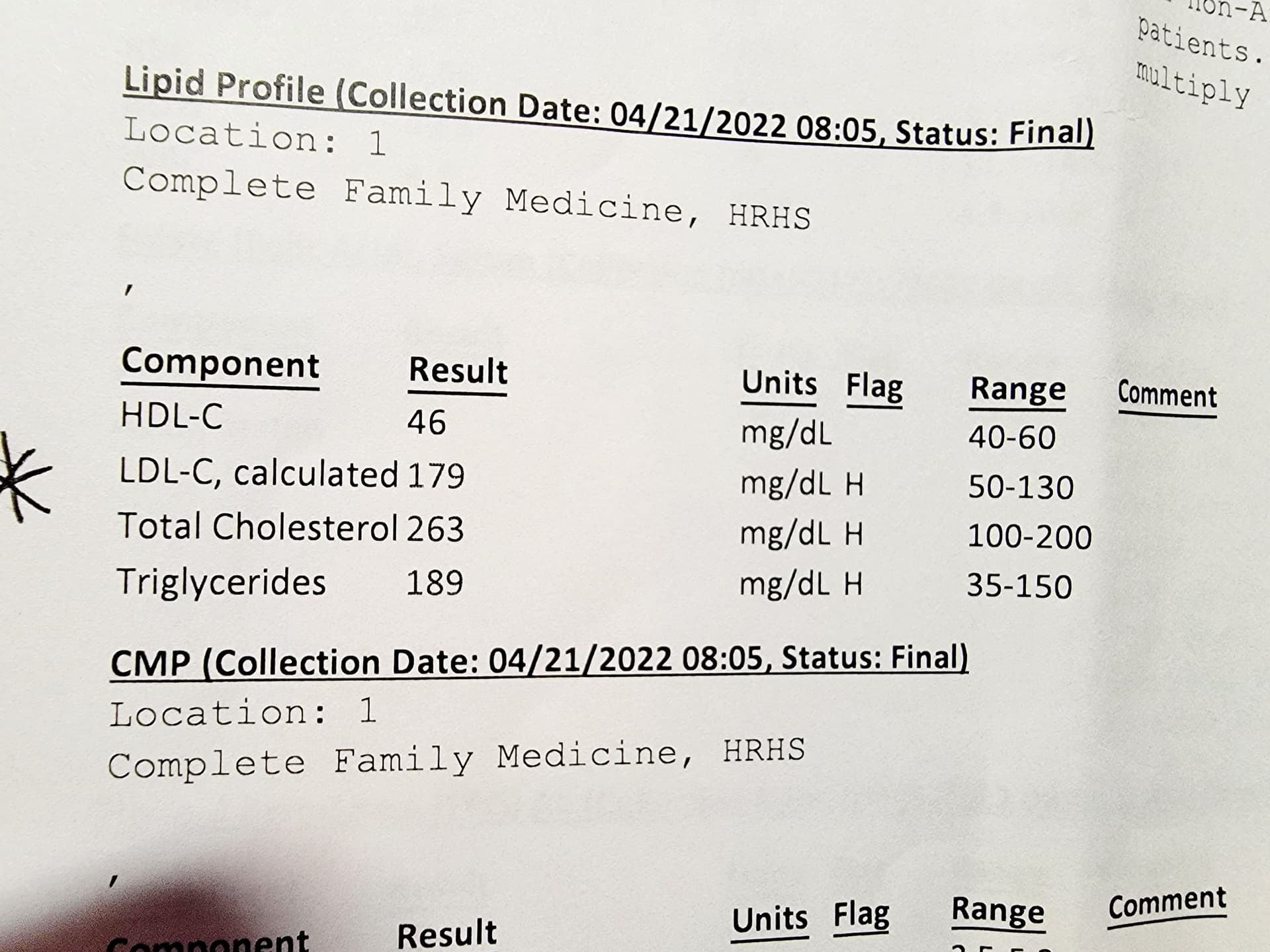
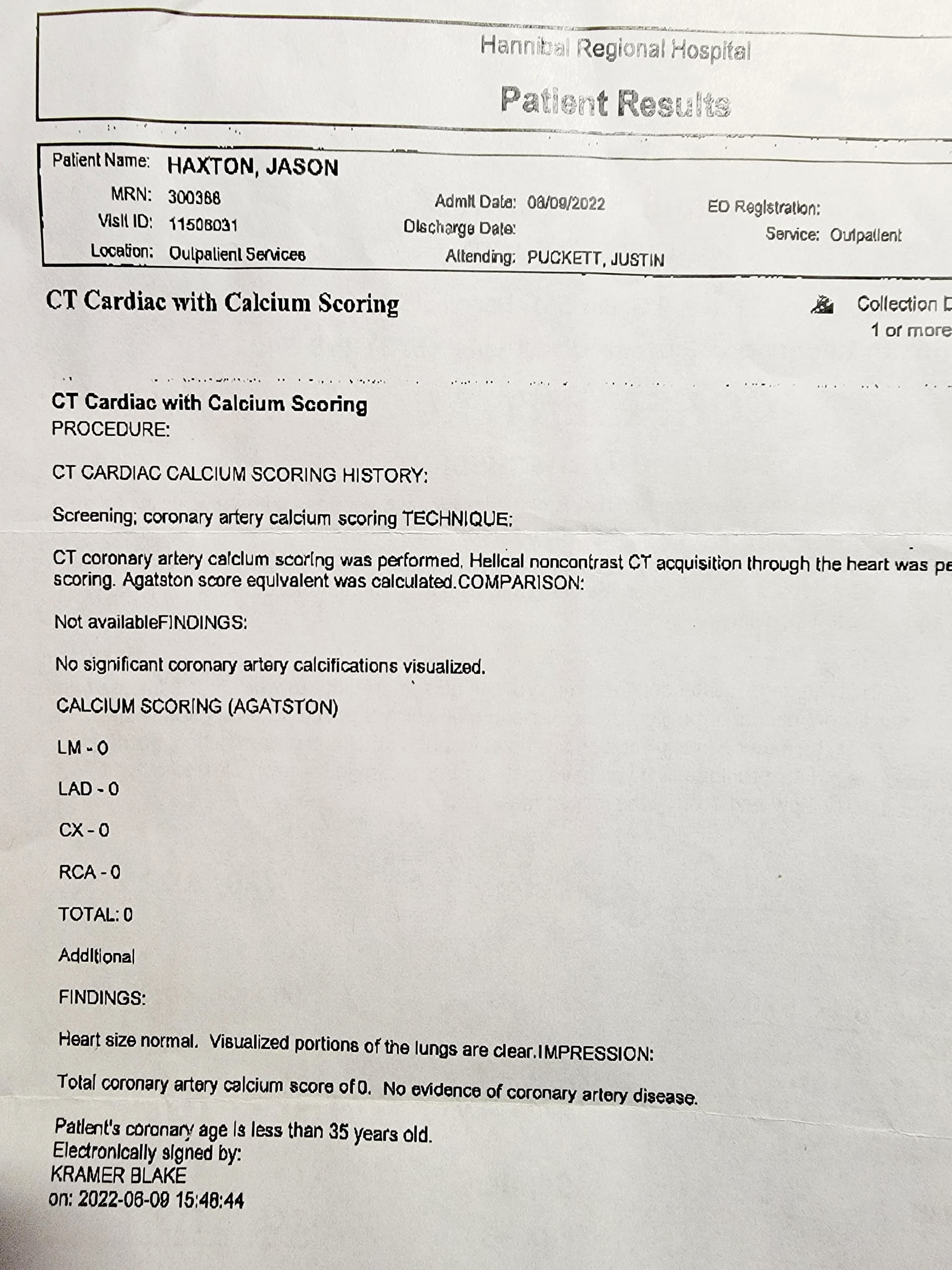
So before Rapamycin my LDL was above 130…then since being on Rapamycin the past two years my LDL has gone up even higher (enough it was a topic at each 3 month blood review). It has stayed these numbers consistently.
With my Cardiac Calcium scoring of absolute 0 zero. Discussion of my LDL no longer a concern.
This is excellent n=1 tracking, thanks for sharing!
Same diet before and after, no other major intervention other than Rapamycin?
You measure hba1c? CBC?
By classic atherogenic markers, your TG/HDL and TG and remnant cholesterol are all HIGH CVD risk profile.
So keep on eye on them and I would do another coronary calcium, maybe 2 yrs. Not wait 5 at your age. With a score of zero, you are at low risk. But I wouldn’t treat with zero CAC and your health profile.
The literature shows a cardio event is possible even with CAC of zero with other CVD risks. Seems like the only risk is lipids, otherwise excellent health and far away from metabolic syndrome, but are these benevolent elevations or not?
You are a classic Rapamycin reference case. Maybe it’s your genes.
MAC wrote: Same diet before and after, no other major intervention other than Rapamycin?
Exactly… never changed my diet… pretty much omnivore… heavy on meat, whole milk, and eggs.
Even before taking Rapamycin always have a steak and two big glasses of milk… loaded baked potatoe… after my gym work out… literally every other day… past 5 years. Pretty much eat what I like… lots of cheeses, dark chocolate, 2 cups of dark coffee, honey and french cream daily.
Did reduce white sugar 2-years ago …started using Stevia in my coffee.
Stay at about 180 pounds since Rapamycin was as high as 196 pounds before Rapa.
Just have not been motivated to look into that test… I’d rather pay and get lab information on methylation, DNA… and protein glycans from spit and blood tests… lol.
Spit says I am 51 biological age. Blood says 37 years. Neither is shabby. Want to do GrimAge!
Since we want you to remain ageless, and longevity is all about reducing all cause mortality, have you ever had a colonoscopy, you’re 62 yes?
Any family history? This is yet another very simple screening tool like CAC (ok, a bit more invasive!), and given your carnivorous diet (a major colorectal risk factor), highly recommend you get one. And yet, so FEW people get them as a screening tool. The earlier you catch it, the better your prognosis.
Very interesting data. Thanks.
Once again lipids do not = death. They are 1 risk among many.
And by many
Smoking, BP, genetics, sleep, stress,exercise, air pollution, age, gender,diet, telomere length, diabetes, past history of heart disease, alcohol, Etc.
I’d love to be a fly on the wall when your PCP sees your labs and hears your diet. He/ she will be the one with the heart attack.
I agree that the goal is to prevent all age related diseases. Prevention and early detection.
I like colonoscopy and also the yearly second generation FIT stool exam if colonoscopy is negative.
Mammograms are useful, but many false positives.
PSA and free PSA are less certain in my mind . I’m never sure what to make of the results. Many false positives. Might get a prostate MRI. Newer urine tests are encouraging.
I’m really thinking about Prenuvo screening. I heard about it some years ago on an Attia podcast. The false positives are very low and you can catch things very early.
All of that being said, I feel very confident that rapamycin is cancer protective to a large degree.
So like my research with Rapamycin… so was it with this procedure… recommended at age 50 to 55 years?
Saw my wife go through this…I was not about to have it… had to be something better. No colon cancer or issues in my parents or grandparents living into late 80’s and early 90’s.
Researched Cologuard… was almost as effective in detection of cancer as colonoscopy…talked to my doctor… he thought I was nuts. But years of research was there. Wife told me to just do the colonoscopy! I said nope! Reluctantly he signed the order. My new physician padt 3 years…obviously listens to me, on TRT, Metformin and Rapa. Says my health is amazing… the physical change …2 different people.
Nobody knew what Cologuard was… much like Rapamycin today…lol. FDA approved it mid-August 2024…by November…I was signed up…I was around Cologuard user 432. Yep!
Today it is standard screening… over colonoscopy. Because I was one of the first…and it can be done every 3 years… had my 3rd screening in February 2022. Negative.
In March 2022 another kit arrived… ??? Couldn’t figure out why I had another one … wifey said… “that’s her kit!” Hahaha.
She got a positive… negative… had to do the whole colonscopy route. Karma.
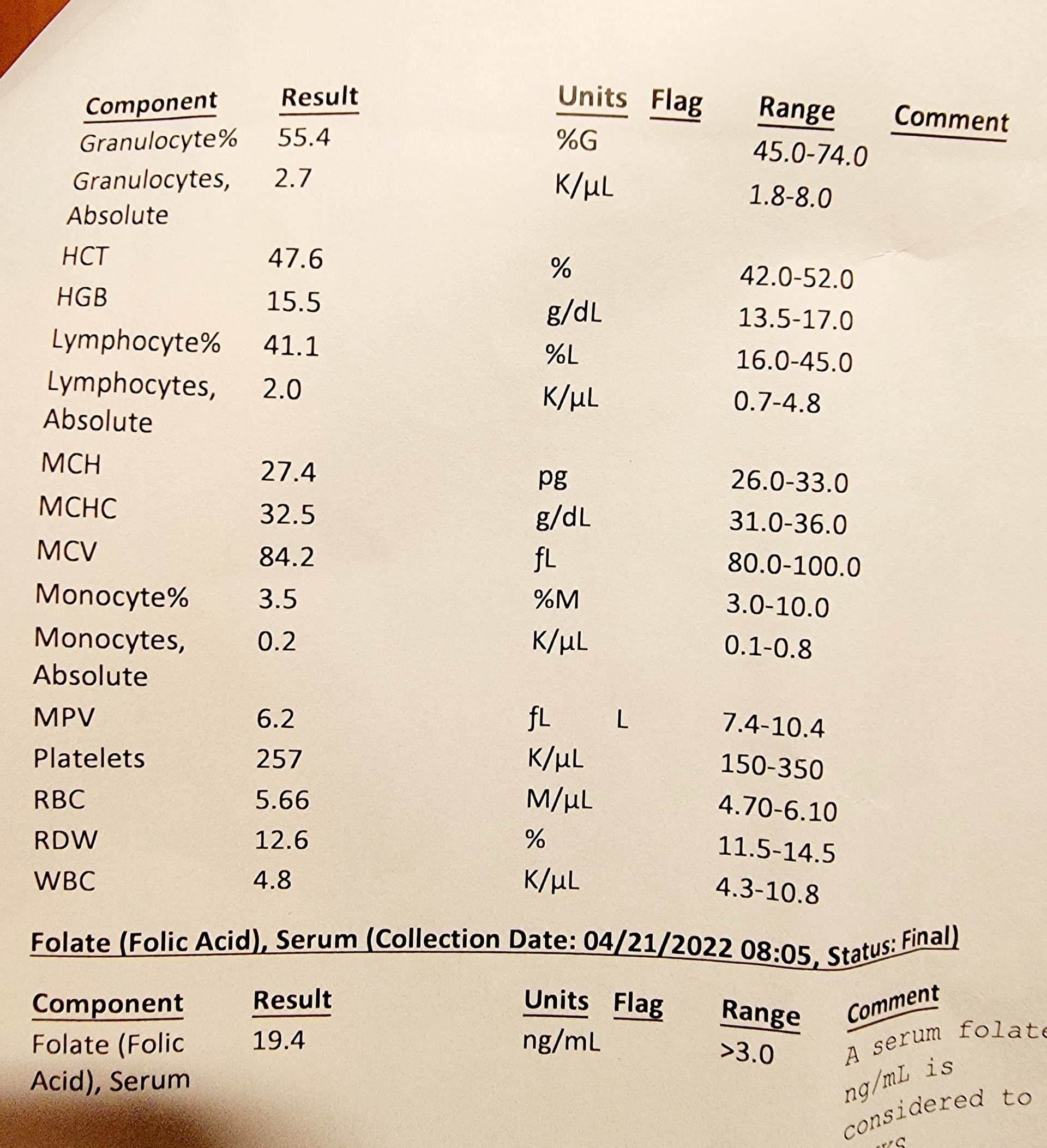
There’s something else I’m noticing in your data. Your granulocytes are at the lower end of normal. The major component of them are neutrophils. Neutrophils are necessary, but can be nasty and contribute to a whole variety of evils, including CAD, especially NETs
Rapamycin May have an inhibitory effect on neutrophils leading to suppression of the innate immune system and possibly increased bacterial infections. But, like everything with rapa, there’s a silver lining perhaps.