SNK, Hilarious anecdote, I don’t think it proves your point but hilarious none the less, and I’m all for a sense of humor!
PS - although “HUGE” might be an exaggeration.
EDIT: Yes, I can see why it was inappropriate but I thought talking about Bryan Johnson’s…“johnson” was too, even if it is worth a million dollars.
2 Likes
I was certain someone will rightly note that hahaa
Nitric Oxide production is linked to lower risks of arteriosclerosis and heart attacks. Citrulline supplementation increases nitric oxide production and lowers BP.

2 Likes
I will do 10 mg rosuvastatin + 10 mg ezitimibe instead next.
I chose rosuvastatin over atorvastatin:
- I already had success with rosuvastatin.
- It is not metabolized at CYP3A4 which mean I can try rapamycin later with GFJ, and also fewer drug interactions I guess.
- It being hydrophilic might give benefits.
- I can monitor diabetes risk anyway so it doesn’t matter that much that is has a higher causal risk compared to atorvastatin.
- Both Trump and Biden takes it.
- Peter Attia recommends it to start with.
Why are you raising the statin dosage? Wouldn’t it be more logical to simply add Ezetimibe for a clearer assessment of the additional benefits?
2 Likes
That is already done in clinical trials. I don’t really need to test things more. It is expected to decrease apoB a little bit more.
I could wait and do 5 mg rosuvastatin + 10 mg ezitimibe first, doesn’t really matter as the difference isn’t that big.
I will also not focus so hard on eating “healthy”, instead I will focus on hydration and eating earlier in the day to avoid high serum sodium during night etc. If there is good food that is considered “healthy” I don’t mind so much, meaning if I want to eat it.
This seems to be the best approach indeed: Efficacy of combination therapy with ezetimibe and statins versus a double dose of statin monotherapy in participants with hypercholesterolemia: a meta-analysis of literature | Lipids in Health and Disease
The addition of ezetimibe to statin appears to be more effective on reducing LDL-C and TC concentrations than doubling the statin dose.
See Fig. 2 here for rosuvastatin specifically: https://www.sciencedirect.com/science/article/pii/S0149291818300079
I wonder if there are trials looking at rosuvastatin 10 mg vs 5 mg + ezetimibe in terms of insulin resistance (HOMA-IR), new onset of diabetes, and fasting glucose. [Edit: I quickly searched and could only find a few small trials run for just a few weeks that showed either no significant difference between the two options or some benefits for adding ezetimibe. So TBC over longer periods of time.]
2 Likes
I will try that, 5 mg rosuvastatin and 10 mg ezetimibe. I think based on all available information this seems like the best approach. Ezetimibe could be argued to be decreased to 5 mg as well but it doesn’t matter so much. It’s a very good stack to decrease risk of ASCVD and one I will test now.
4 Likes
I believe Ezetimibe has no adverse effect on glucose metabolism and no statistically significant effect on NOD when combined with statins (IMPROVE-IT trial), but I remember in mouse studies some markers of glucose metabolism were improved with Ezetimibe.
1 Like
Yes, ezetimibe seems to improve glycemic control, endothelial function, and mitochondrial health in animal and cell models:
- Approved drugs ezetimibe and disulfiram enhance mitochondrial Ca2+ uptake and suppress cardiac arrhythmogenesis 2021
- Ezetimibe attenuates experimental diabetes and renal pathologies via targeting the advanced glycation, oxidative stress and AGE-RAGE signalling in rats 2021
- Ezetimibe Protects Endothelial Cells against Oxidative Stress through Akt/GSK-3β Pathway 2018
- Chronic administration of ezetimibe increases active glucagon-like peptide-1 and improves glycemic control and pancreatic beta cell mass in a rat model of type 2 diabetes 2011
In humans, I could only find one not-so-recent meta-review: Effect of ezetimibe on glycemic control: a systematic review and meta-analysis of randomized controlled trials 2018
Compared with high-dose statin therapy, ezetimibe with low-dose statin for more than 3 months may have a beneficial tendency of effects on glycemic control.
But again, most studies are super short. This recent one, short as well (12w) found that “However, in our study, both HOMA-IR and HOMA-β were decreased only in the rosuvastatin/ezetimibe combination therapy group in which LDL-C was reduced by more than 50% from baseline. After adjusting for DM duration and hypertension, there was not a statistically significant difference in HOMA-IR change between the two groups. These results suggest that ezetimibe effects on insulin sensitivity might be influenced by several factors such as baseline insulin resistance and insulin secretory capacity.” (Comparative Efficacy of Rosuvastatin Monotherapy and Rosuvastatin/Ezetimibe Combination Therapy on Insulin Sensitivity and Vascular Inflammatory Response in Patients with Type 2 Diabetes Mellitus 2024)
On another note, I didn’t know that bempedoic acid led to a small weight loss (vs a small weight gain for statins): https://twitter.com/CMichaelGibson/status/1695452860815921635
4 Likes
There are actually four ongoing trials looking at this question over longer periods of time:
- Low Dose Rosuvastatin Plus Ezetimibe Versus High-dose Rosuvastatin in AMI (ROSUZET-AMI): 3,548 patients, running from 2020 to 2024 (results soon?), comparing rosuvastatin 5 mg + ezetimibe 10 mg vs rosuvastatin 20 mg.
- Usual Dose Rosuvastatin Plus Ezetimibe Versus High-dose Rosuvastatin on Coronary Atherosclerotic Plaque (Rosuzet-IVUS): 280 patients, running from 2017 to 2024, comparing rosuvastatin 10 mg + ezetimibe 10 mg vs rosuvastatin 20 mg.
- Comparison of Low-Intensity Statin Plus Ezetimibe Versus High-Intensity Statin Therapy on Risk of New-Onset Diabetes Mellitus (PROVE-DM): 4,000 patients, running from 2023 to 2027, comparing rosuvastatin 5 mg + ezetimibe 10 mg vs rosuvastatin 20 mg.
- Clinical Comparison of Low-dose Rosuvastatin Plus Ezetimibe Combination Therapy and High-dose Rosuvastatin Monotherapy in Patients With Minimal to Intermediate Coronary Artery Disease Without Percutaneous Coronary Intervention (ALMIGHTY): 6,356 patients, running from 2024 to 2029, comparing rosuvastatin 10 mg + ezetimibe 10 mg vs rosuvastatin 20 mg.
For whatever reason, they’re ALL run in Korea, and in Korea only, by four different institutions.
(I guess if I had to start a lipid-lowering therapy, I’d start ezetimibe alone first, then, if needed, add bempedoic acid. Then wait and see and reassess the decision whenever more data is available…)
3 Likes
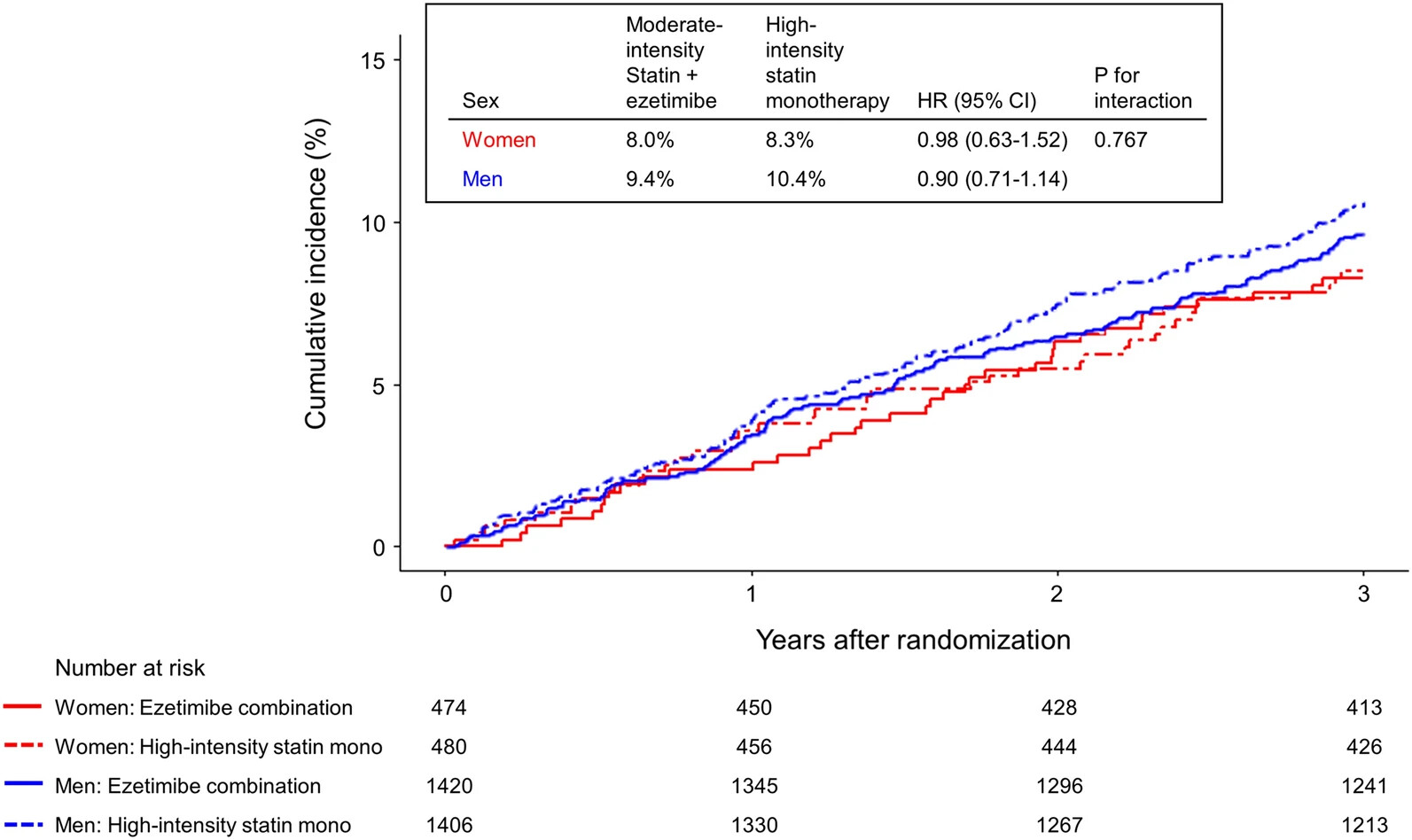
Actually there’s this large recent trial (in Korea again!): Effect of moderate-intensity statin with ezetimibe combination vs. high-intensity statin therapy according to sex in patients with atherosclerosis 2023
3780 patients over 3 years, rosuvastatin 10 mg + ezetimibe vs rosuvastatin 20 mg. Conclusion:
LDL cholesterol levels of < 70 mg/dL at 1, 2, and 3 years were more frequently achieved in the ezetimibe combination group than in the high-intensity statin monotherapy group (all P < 0.001) in both sexes.
They write that “The effect of ezetimibe combination therapy for the 3-year composite outcomes was not different in both men and women. The benefits of ezetimibe combination therapy on LDL cholesterol lowering and drug tolerance were similarly observed regardless of sex.” However, ezetimibe might be more beneficial among men over the long run based on the trend below:
It’s interesting because this MR indicated a potential pro-longevity effect of ezetimibe among men only as well: Ora Biomedical launches crowdfunding of Million Molecule Challenge - #69 by adssx
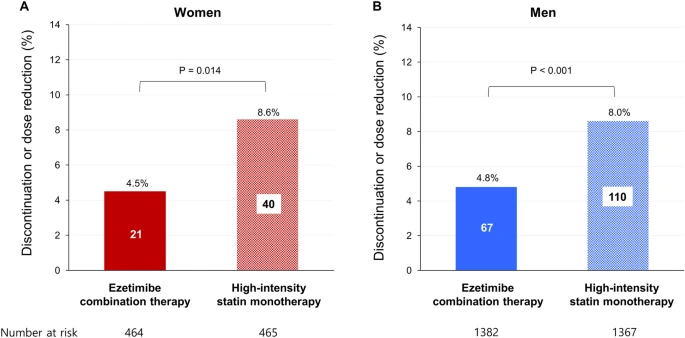
The improved treatment adherence in the statin+eze arm is also massive (especially among men):
The rate of discontinuation or dose reduction of study drugs due to intolerance was lower in the ezetimibe combination group than in the high-intensity statin monotherapy group in both women (4.5% vs. 8.6%, P = 0.014) and men (4.8% vs. 8.0%, P < 0.001).
5 Likes
Given both sources (Carlson and Calley Means).
1 Like
A glass of wine will definitely not help you sleep better: it will sedate you, but that’s not naturalistic sleep. Put on an Oura ring or another good-quality sleep tracker with HRV and watch alcohol wreck your HRV and REM sleep and distort your overnight sleep resting heart rate “hammock” pattern.
3 Likes
Who cares? --------===
1 Like
Well, anyone who wants their brains cleared of beta-amyloid, or their experiences encoded in memory, or their emotional regulation to be intact, or their executive function to operate, or to get any of the other benefits of naturalistic sleep.
4 Likes
This seems to me to be a reasonable question. You’re used to having a glass of wine with dinner and you really enjoy it. You sleep fine - no trouble - 8 hours - and wake up feeling well rested. You’re healthy, get plenty of exercise, feel energetic - never tired. But then you start hearing about sleep quality and sleep monitors. So you get an Oura ring or whatever and you discover that yes that glass of wine is causing (previously unknown to you) your sleep quality score on your app to be poor. Is that something you should lose sleep over?
1 Like
I don’t think we should overly worry about Oura or other sleep tracker metrics at this point in time.
But there seems to be a lot of clinical data from sleep labs that show how alcohol materially worsens sleep architecture?
Differences in sleep quality over the years and decades seems to be something very significant - perhaps as impactful as the other main pillars that we can influence.
1 Like
I’m not questioning the science behind it. I’m sure that there is something there. But we all have to prioritize and make decisions. For example, it’s probably true that air pollution is worse in the cities. Should we all move to the country or up in the mountains. The science seems to increasingly be saying that any alcohol is bad, but if that glass of wine with dinner is one of your pleasures in life, what are the tradeoffs?
2 Likes
Ok, I think I understand you now.
Each person will likely have a different decision on how to weigh the tradeoff. (Just thought it important that we all understand that it likely is a tradeoff).
3 Likes