High-dose atorvastatin therapy progressively decreases skeletal muscle mitochondrial respiratory capacity in humans
RESULTS. Maximal ADP-stimulated respiration, measured in permeabilized fiber bundles from muscle biopsies taken at each time point, declined gradually over the course of atorvastatin treatment, resulting in > 30% loss of skeletal muscle mitochondrial oxidative phosphorylation capacity by day 56. Indices of in vivo muscle oxidative capacity (via near-infrared spectroscopy) decreased by 23% to 45%. In whole muscle homogenates from day 0 biopsies, atorvastatin inhibited complex III activity at midmicromolar concentrations, whereas complex IV activity was inhibited at low nanomolar concentrations.
CONCLUSION. These findings demonstrate that high-dose atorvastatin treatment elicits a striking progressive decline in skeletal muscle mitochondrial respiratory capacity, highlighting the need for longer-term dose-response studies in different patient populations to thoroughly define the effect of statin therapy on skeletal muscle health.
They used 80 mg and it’s well-known that the dose response of statins is very shallow so you shouldn’t increase the dose but use something else like ezetimibe or bempedoic
What’s concerning to me is that the effect was seen after only 8 weeks! Would atorvastatin 10 mg show the same effect after a 2y?! Or is there a threshold under which the drug doesn’t cause that?
By the way, this company/charity has a nice approach: they combine the best drugs at a low dose to improve efficacy and reduce side affects: Developing Late-Stage Drugs - Our Pipeline - George Medicines
They started with antihypertensive and glucose-lowering drugs. I asked them about lipid-lowering, for instance rosuvastatin 1.25 mg + ezetimibe 2.5 mg + bempedoic acid 45 mg.
There is no control group with that study so it isn’t that useful.
ApoB will destroy your vascular system.
But I agree there isn’t really a point in taking high dose statins if other medications etc are available.
I had a mild heart attack in late 2017, followed by open heart surgery for a new aortic valve and 3-way bypass. My weight goes up and down and follows the seasons. When I can get out and walk I eat less and lose weight. I’m 5’-8" and weigh 190 to 210lbs. This year I am going to try and get down to 175lbs, the lightest I’ve been since the 1980’s.
I take 80mg of Lipitor and other prescriptions. My HEMOGLOBIN A1C was 6.1 recently. I do not have any other recent numbers to post, but my doctors all like what they see. In 2017 my numbers were all very high, now they are almost normal.
I take 35+ supplements, and 4+ tablespoons of EVOO per day. My doctors know of and do not approve of my supplements. I am counting on some help from the supplements and I am trying to LIVE. I ignore the doctors on things like supplements, it is my life and if I am desperate to live, so who is to say what I am doing is 100% wrong?
I am on a Mediterranean diet without much in the way of alcohol(12 to 24 beers a year MAXIMUM) and little to no sweets/pop. But one does not get there within days of the open heart surgery. I had to adapt or die(in my case). I figure it took me a year or more to get to where I am and I did it on my own with no help from doctors. I could have asked for a meeting with a dietitian but did not. I kept researching the subject of diet and exercise while adding/deleting food from my diet. My diet and lack of exercise are an ongoing battle.
I think it is important to remember that even relatively easy exercise like walking is good.
To continue a previous topic: Rapamycin and risk of cardiovascular disease - #3040 by adssx
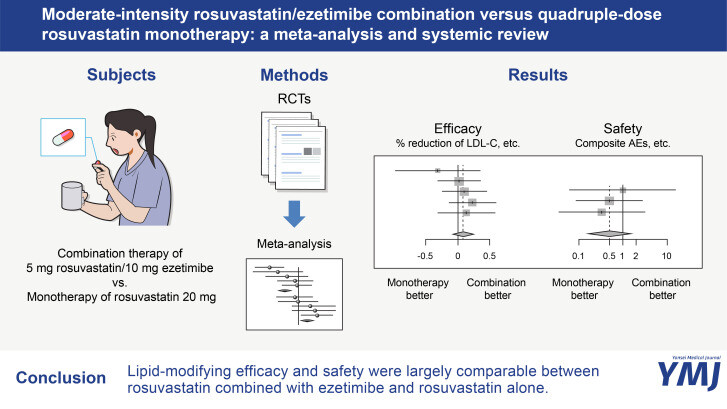
This meta-analysis showed that 5 mg rosuvastatin/10 mg ezetimibe had largely comparable lipid-modifying efficacy and tolerability as 20 mg rosuvastatin.
I’m surprised (and disappointed) that in terms of safety the combination doesn’t perform better than the monotherapy.
That high dose statins are bad and that ezetimibe and low dose statins are better is almost speculation.
These are hard for many if not most people, at some points in our life. I recommend you check into this mini conference: Stanford U. Mini-Conference (online) "The Household as a Unit of Health Behavior Change", Saturday, March 9th, 11:00 am - 2:00 pm (PST)
Also this book too: Amazon.com
Thank you.
I will check into those items.
I tried rosuvastatin 10 mg, but after a week I had discomfort in the right hypochondrium, after which I stopped, I suspect that rosuvastatin can cause pancreatitis and liver damage…
That’s not helpful as it’s not saying what you are doing instead.
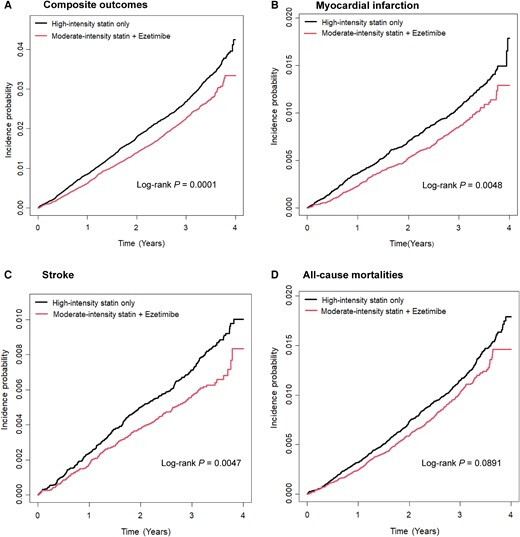
Another Korean study looking at this question: Combination of low- or moderate-intensity statin and ezetimibe versus high-intensity statin monotherapy on primary prevention of cardiovascular disease and all-cause death: A propensity-matched nationwide cohort study 2024
Compared to high-intensity statin monotherapy, moderate-intensity statin with ezetimibe combination significantly reduced the risk of composite outcome (hazard ratio [HR] 0.84, 95% confidence interval [CI] 0.77–0.92, P < 0.001) as well as individual MI (HR 0.81, 95% CI 0.71–0.94, P = 0.005) and stroke (HR 0.78, 95% CI 0.65–0.93, P = 0.005), but not all-cause death. Low-intensity statin with ezetimibe also significantly reduced the risk of the composite outcomes (HR 0.80, 95% CI 0.66–0.97, P = 0.024) compared to high-intensity statin monotherapy, but the risk of individual outcome did not differ between two groups.
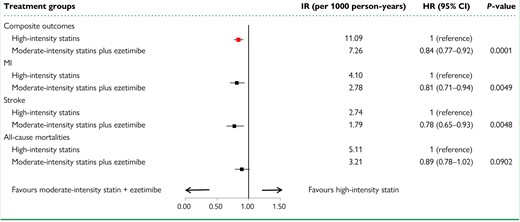
(HR for all-cause mortality close to significance in favor of the combination)
Compared to guideline-recommended high-intensity statin therapy, moderate-intensity statin with ezetimibe further improved the achievement rate of LDL-C in patients with acute ischemic cerebrovascular disease, with a higher reduction magnitude in LDL-C. In terms of safety, there was no significant difference between the two regimens, suggesting that moderate-intensity statin with ezetimibe can also be considered as an initial treatment option for patients with acute ischemic cerebrovascular disease.
Unfortunately they defend “safety” as “liver and renal function tests, and the occurrence of statin-related muscle events within 3 months”. I’d like to see new onset of diabetes or just Hb A1c increase.
Forget the statins and take Bempedoic Acid. There is neither muscle fatigue nor increased risk of diabetes.
That’s also what I thought but I don’t like the +15% increase in uric acid with bempedoic acid: Effect of bempedoic acid on uric acid and gout in 3621 patients with hypercholesterolemia: pooled analyses from phase 3 trials | European Heart Journal | Oxford Academic
I’d rather take higher uric acid levels than muscle soreness or diabetes. I’ve experienced muscle soreness from statins and it was intolerable. For uric acid, you can drink more water.
I tend to agree but uric acid seems important: Blood biomarker profiles and exceptional longevity: comparison of centenarians and non-centenarians in a 35-year follow-up of the Swedish AMORIS cohort - #5 by cl-user
Anyway now I’m focused on optimizing my BP. Once done I’ll look at lipids. One step at a time… But I guess I’ll start with bempedoic acid/ezetimibe (and/or obicetrapib if approved?).
Dr Rick Johnson agrees that Uric acid is a driver of poor health. He and others have pointed to Uric acid as one of the top handful of biomarkers to keep in range.
What are the top strategies to reduce uric acid? Is it a U-shaped curve? Or lower is always better?
@DeStrider Is lowering uric acid useful for longevity? - #3 by L_Hayes
This thread has a bunch of info. Dr Johnson emphasized reducing purines, as I recall. No beer, sadly.