But it does beg the question, what is optimal apoB? And does that optimal range vary if inflammation, bp, oxidation and other factors are optimal.
1 Like
I apologize; I didn’t frame my comment correctly. I did not mean to criticize anything. That said, please chill out and assume good faith and best intentions. We’re all here to help each other reach our goal(s). These goals might be different. And not everything is rational; we may have our own fears, justified or not. Or at least, I have. So I should have been clearer in my previous reply that because I have a family history + genetic risk of neuro-psychiatric conditions (MDD, AD, PD, etc.), I put more weight on this risk than on others such as CVD. Maybe unreasonably so. Still, @A_User summed it nicely, “If someone wants to live 200 years they must have optimal apoB.” and “If someone just wants to live to 50-80 yrs old and avoid PD, that’s different.” I feel like I prefer to die at 80 from a heart attack than live 100yo with AD or PD starting at age 60 and seeing myself decline every single day, incontinent and demented. Again, it might be illogical, but that’s how I feel now. I didn’t care that much before when my ApoB was at 68 mg/dL, but in my latest test, it surprisingly jumped to 97, and now I wonder what to do ![]() (First, redo the test…
(First, redo the test… ![]() ) There are more and more MR and longitudinal studies published so I’m convinced that this question will be solved in the next 24 months. Researchers might find that non-statin lipid-lowering agents have a better long-term safety profile for people at risk of PD (or other NDDs). Or they might actually dismiss all the previous fears around statins and prove that the effects were not causal. Time will tell. For now, for me, the jury is still out. For the general population, I agree with your statements (a), (b), and (c).
) There are more and more MR and longitudinal studies published so I’m convinced that this question will be solved in the next 24 months. Researchers might find that non-statin lipid-lowering agents have a better long-term safety profile for people at risk of PD (or other NDDs). Or they might actually dismiss all the previous fears around statins and prove that the effects were not causal. Time will tell. For now, for me, the jury is still out. For the general population, I agree with your statements (a), (b), and (c).
9 Likes
MDD - statins are positive, not negative.
AD - mixed results, LDL increase, increases risk iirc in MR. ApoE4 genes tend to increase lipids.
PD - slight decreased risk for higher LDL.
I like to work with one disease at a time, and find the causal pathways for that disease, especially the necessary conditions. First I solve heart disease, then the next one, and so on.
Remember that heart attacks are no fun, and the atheroschlerosis preciding that probably does cause damage to the brain, heart, increase risk of strokes, mini strokes, which can cause depression, etc and hurt the brain.
I think that meditation helps with worrying about dementia risk. I remember a meditator called Shinzen Young said that he’d prefer to live one day in his state of mind of enlightenment, than decades of being extremely rich, large house, lots of sexual partners etc, like a rockstar, but without that state of mind. He is an advanced practitioner.
He did try an experiment where they withdrew a medication for the thyroid I think for a study, which leads to a large deficit in cognition, and he was able to maintain the state of awareness he prefers. So it’s possibly to be quite happy despite losing one’s cognition, I think.
4 Likes
Also worth remembering that it’s not just your heart and brain that apoB is damaging, it also causes ED.
1 Like
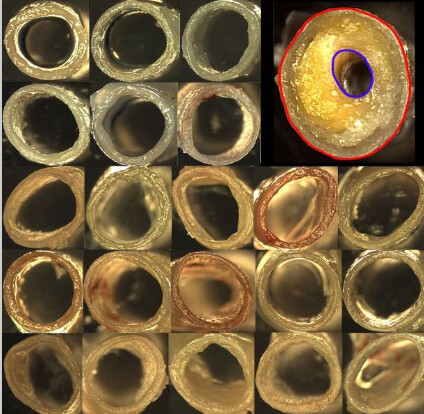
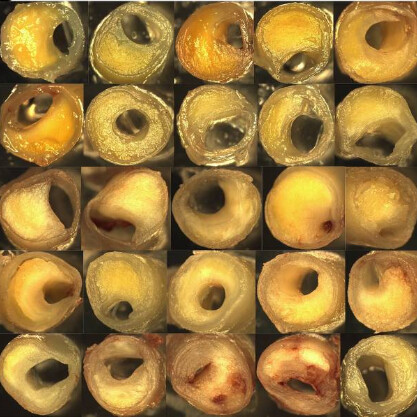
Atherosclerosis in the brain looks so nasty and it makes sense how bad it is for blood flow / brain function, can cause vascular dementia, as well as causing ED.
5 Likes
They’re positive when combined with antidepressants (Statins for major depressive disorder: A systematic review and meta-analysis of randomized controlled trials 2021), alone, I don’t know, probably neutral.
And among PD patients, statins accelerate motor decline and potentially also cognitive decline.
The difficulty being that PD starts at least 10y before diagnosis, so you don’t know whether you’re a PD patient or not.
Of course, that’s why I’d love to find something that can both lower apoB AND the risk of PD/DLB. Or at least be neutral towards PD/DLB. As I said there, ezetimibe might be the way. There’s some weak positive signal for fenofibrate in some papers as well. Bempedoic acid might be too recent to have data on it.
(and yes, meditation helps a lot ![]() )
)
2 Likes
Study might’ve been too small to detect an effect, I was basing my claim on that meta that did detect an effect combined with anti-depressants but most importantly all the association evidence.
Yes true.
Sure, but it also depends on your age. PD diagnosis happens mostly in 50’s I’d guess? So until 40 statins are ok to use. In 10 years we will have more meds / possibly gene therapy to lower cholesterol. I’m not going to do nothing until that time since it’s 10 years of exposure to above optimal apoB.
Ezetimibe is very weak and it won’t work on its own.
I’m below 40, and I wouldn’t take the risk still (“About 10%-20% of those diagnosed with Parkinson’s disease are under age 50, and about half of those are diagnosed before age 40.”) People who care about PD because of family history, genes, pre-PD symptoms, or environmental risk (such as lifetime exposure to pesticides like paraquat) might share the same worries (justified or not).
Weaker than statins for sure, but I wouldn’t say “very weak”:
- “ezetimibe monotherapy was associated with a statistically significant mean reduction in LDL cholesterol (from baseline to endpoint) of -18.58%, (95% CI: -19.67 to -17.48, P < 0.00001) compared with placebo”
- “Ezetimibe monotherapy (10 mg/day) showed a small (7.06%) but statistically significant reduction in the plasma levels of Lp(a) in patients with primary hypercholesterolemia.”
2 Likes
I don’t know how to combine the result in the simvastatin trial with the 10-20% probability of the PD diagnosis with the PD diagnosis risk. It seems small to me, even with family history. The cases of Parkinson’s in my family history is from people living on a farm. I think it might’ve been pesticides or something. How heritable is the disease? What’s the relative risk increase?
No one really knows. “About 15 percent of people with Parkinson’s disease have a family history of the condition”. Some think that “Parkinson’s Disease Is Predominantly an Environmental Disease” (from 2 weeks ago). Indeed, living near farmland is not amazing:
Finally, genetic differences also cannot readily explain the near perfect correlation between use of pesticides and PD prevalence [29], the strong association between agricultural activities and its incidence […] For example, in France the increased risk of developing PD is not limited to farmers [39, 40] but extends to those living near farmland or vineyards [30]. Pesticide exposure may also lead to faster disease progression after the diagnosis has been established.
By the way, from Sept 2023: Aggressive LDL-C Lowering and the Brain: Impact on Risk for Dementia and Hemorrhagic Stroke: A Scientific Statement From the American Heart Association
They conclude:
Although some older retrospective, case-control, and prospective longitudinal studies suggest that statins and LDL-C lowering are associated with cognitive impairment or dementia, the preponderance of observational studies and data from randomized trials do not support this conclusion, at least over the course of the trials that varied from a median of 1.6 to 6.0 years of follow-up. Additional studies are needed to ensure cognitive safety over longer periods of time. In the interim, contemporary guidelines recommending the risk-stratified attainment of lipid-lowering goals are reasonable.
Importantly, they did not include Parkinson’s in their assessment. Parkinson’s dementia and Lewy body dementia were not specifically explored but included as part of “all-cause dementia” I assume.
2 Likes
Head injury is also a major risk factor (think M Ali)
3 Likes
If we even assume some heritability, then the RR increase from using statins for 10 years must be very small, the total absolute risk. If the base rate is 2%, increases to 4% with genetic risk, 0.8% (20% of 4%) chance that PD develops before 50, or is my math off? Then you increase the 0.8% risk by whatever the RR increase is for statins which I don’t think we know. If we assume no heritability then it is half.
5 mg ezetimibe should reduce apo b by about 26%. Add in some fish (it may reduce omega 3 absorption) and you should be back jn the 60s.
Did your apo b rise due to rapamycin?
2 Likes
Thanks. I’m not even taking rapa so I don’t know the cause. As I got an incorrect result for another metric (PTH) from that lab I’ll first redo the test with another lab. But yes I’m not too worried, as there are available treatments.
3 Likes
Yes, I’m experimenting with policosanol at the moment, and you could always up your coffee (a weak psk9i) … I Just spotted this : Scientists discover how caffeine protects against cardiovascular disease
1 Like
Doesn’t coffee increase LDL? Coffee and cholesterol: Health risks, benefits, and more
(coffee is protective against PD btw)
1 Like
Again, I would like to point out that methylene blue and photobiomodulation is useful in both treating and preventing brain disorders.
The first paper below has quite an extensive discussion on the use of MB in treating or perhaps preventing Parkinson’s disease
What is especially helpful about this paper is the plethora of citations concerning MB and brain and mitochondrial functions.
2 Likes
Thanks a lot @adssx , nothing to apologize for.
100% agree with the sentiment that we are all here to help each other.
I think that actually might have been what triggered me - I did not want the information and rationale that our discussion to lead to misunderstanding by anyone else reading the thread and then taking away incorrect ways of thinking about things.
I do truly believe you have always acted with good faith.
And - I do think you with your data and publication driven approach are one of the best contributors to the forum in recent months! So thank you so much for all your contributions.
Onward and upward ![]()
![]()
![]()
5 Likes
Thx for this and the other paper with eg
Mitochondrial dysfunction plays a central role in the formation of neuroinflammation and oxidative stress, which are important factors contributing to the development of brain disease. Ample evidence suggests mitochondria are a promising target for neuroprotection. Recently, methods targeting mitochondria have been considered as potential approaches for treatment of brain disease through the inhibition of inflammation and oxidative injury.
@adssx have you thoughts about key thinks that sustain optimal mitochondria, like eg
- zone 2
- fasting (and I think time restricted eating)
- Mitopure, see eg link below
1 Like
I think that was discussed bought based on the worlds current data and understanding a few months ago on the forum?
Or let me know if there is any specific aspect(s) you think we should unpack further?
Otherwise perhaps ok to agree to disagree on how low optimal is in different contexts - and we can revisit as new studies, data and mechanistic understanding comes out?