Wow ![]() what a great argument !
what a great argument !
I really would love to see that tested in a PD model / human clinical trial ![]()
Wow ![]() what a great argument !
what a great argument !
I really would love to see that tested in a PD model / human clinical trial ![]()
I’ve just emailed Pr. Sekhar and asked him about GlyNAC in the ITP and potential PD studies. I’ll keep you posted if he gets back to me…
Just published: Modeling the neuroimmune system in Alzheimer’s and Parkinson’s diseases
Notably, the immune system has been implicated in both diseases, with a particular focus on the dysfunction of microglia, the brain’s resident immune cells, contributing to neuronal loss and exacerbating symptoms.
Recently, the discovery of increased circulating levels of pro-inflammatory markers in AD and PD patients suggested a strong interplay between various neuroimmune and inflammatory mechanisms.
These cells play diverse roles in maintaining the function, plasticity, and integrity of the CNS. Additionally, microglia are actively involved in maintaining homeostasis of the CNS upon various challenges. They contribute significantly to neurogenesis, synapse formation, modification and pruning, vasculature maintenance and repair, axonal myelination, and other essential activities that support CNS activity and health.
In healthy individuals, the central and peripheral immune systems are structurally distinct, thanks to the presence of the highly specialized blood–brain barrier (BBB). In PD, the BBB is known to be leaky, allowing for a less-regulated passage of the peripheral immune cells into the brain parenchyma.
Often, immunomodulation offers a relatively simpler treatment option, utilizing preapproved drugs with known safety and tolerability profiles. Current and prospective immunomodulatory therapies can be categorized into three main groups, broad spectrum immunosuppression, specific immune pathway targeting and microglial targeting
Surprisingly, they list “Kaeberlein M, Galvan V. Rapamycin and Alzheimer’s disease: time for a clinical trial? Sci Transl Med. 2019;11(476)” in the references but they don’t mention rapamycin/sirolimus or any rapalogs at any point ![]()
Table 3 lists various drugs targeting the immune response system currently being trialed, including two for PD:
Sargramostim is an immunostimulant while azathioprine is an immunosuppressant like rapamycin. Azathioprine is used for Crohn’s disease (IBD), and interestingly: “Patients with IBD who were not treated with anti-tumor necrosis factor-α or azathioprine had significantly higher PD risk (adjusted HR = 1.6, 95% CI: 1.2–2.2).” (Association between inflammatory bowel diseases and Parkinson’s disease: systematic review and meta-analysis 2022) TNF inhibitors include the following immunosuppressants:
I don’t think anyone is taking the above immunosuppressants for longevity. But the ITP is currently testing another immunosuppressant: methotrexate.
Surprisingly, telmisartan is also a TNF inhibitor (source) (and also being tested in the ITP).
If microglial protection/activation is a strategy, then it’s interesting to see that:
@momgotshocked, as you’re taking simvastatin, you might be interested in the findings of the above trial.
See also: https://twitter.com/AlbertoEspay/status/1632395647499345920
I wonder if there are better alternatives out there:
Their own point seems to be that statins would generally lower PD risk and the point above is about a subtype of PD only??
This is the opening paragraphs/abstract of the paper
Conclusion A casual association between HMGCRinhibition and reduced overall PD risk was identified, but there were increased the risks of tremor-dominant subtypes.
—-
Example of when MR is not the same as the medication:
Note that PCSK9 in MR are from lifelong exposure including within the brain and CNS - and including from in the womb and while young and brain is growing like crazy - and then through rest of life
The current medicines to inhibit PCSK9 do not have those impacts - both because you do not take them while you are a fetus or young child and because PCSK9i medicines are not small molecule medicines but large antibodies…. they are not thought to cross the blood brain barrier?
See also below post and the one that followed it if you scroll down from that link. Does this analysis make sense or what am I missing?
See also:
Today, virtually all large molecule drugs and more than 98 percent of small molecule drugs in the human bloodstream are unable to enter the central nervous system because of a ‘locked gate’ known as the blood-brain barrier.
Repatha and Pradulent as antibody based treatments should fit in the “large, non-small molecule” category.
From the link in
Found this interesting
COVID and the Brain
A study using stem cell derived dopamine neurons shows that SARS-CoV-2 targets dopamine neurons in the brain. Autopsy specimens confirmed this finding. Once infected by SARS-CoV-2, dopamine-producing neurons lose their ability to grow and divide. They also stop producing dopamine and send out signals that trigger inflammation instead. Parkinson’s disease is caused by the death of dopamine-producing neurons in the brain- specifically in the substantia nigra in the midbrain and this area is affected by COVID.
Some years after the 1918 Spanish flu epidemic, there was an increase in Parkinson’s cases. This new study suggests that there may be an increase in Parkinson’s cases related to COVID infection in the near future as well. Using high-throughput screening, the researchers in this study identified three FDA approved drugs that may protect the dopamine neurons in the brain from being infected by COVID. Riluzole (glutamate inhibitor for ALS), Metformin (oral type II diabetes medication), and Imatinib(tyrosine kinase inhibitor used for some leukemias) may be useful in protecting dopamine neurons from SARS-CoV-2 infection. The authors also recommended long-term monitoring of neurological problems in people who have had COVID-19.
Regarding COVID and the brain, a new multicenter study shows that people with Long COVID have severe cognitive slowing that is 2 to 3 standard deviations slowerthan controls. Comorbidities such as fatigue, depression, anxiety, sleep disturbance, and post-traumatic stress disorder did not account for the extent of cognitive slowing in patients with Long COVID. Severe slowing of brain function affects individuals, but it also has major implications for the work force and the economy on a population level.
That sounds like them (dopamine neurons) turning sensecent.
Another great reason to take Metformin. ![]()
Yes, but high-quality RCT > preprint MR, so I trust the RCT more regarding statins and PD.
On the other hand, this preprint MR is all we have regarding PCSK9i and PD, so it’s enough for me to wave a “red flag” (or maybe just yellow/orange? ![]() ) on PCSK9, for now.
) on PCSK9, for now.
That’s an interesting point, thanks.
It doesn’t need to cross the BBB to cause damage.
Is this the source? I agree with the author. There’s an increase of all NDDs (not only PD, also AD) after infections (not only Covid, also just the flu), see: Virus exposure and neurodegenerative disease risk across national biobanks 2023. So there we’ll see an increase in NDDs in the next few years. Long Covid is just the tip of the iceberg. It doesn’t mean we need to panic, but it’s good to be aware of the risk and to take preventive measures to avoid viral infections and help the body recover after unfortunate infections (we can’t avoid 100%).
It’s probably good at a low dose, indeed. At high doses, metformin is toxic to mitochondria and is associated with higher rates of PD.
Yes. I think if you take Metformin, it should be 500 mg or less daily.
Yes (extra characters)
Thanks.
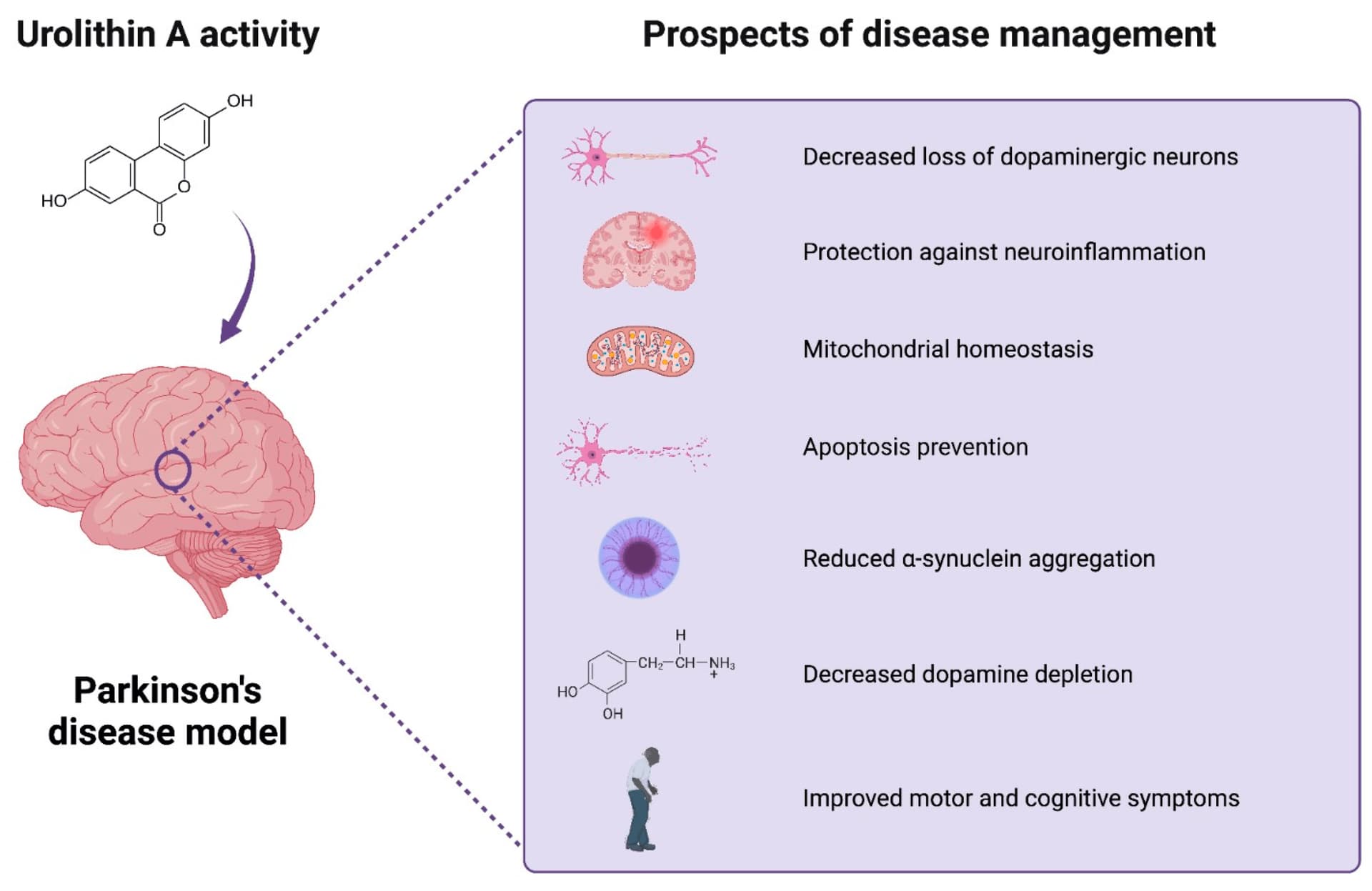
Not the best journal and authors not from the most prestigious institution but still an interesting article: Urolithin A in Health and Diseases: Prospects for Parkinson’s Disease Management 2023
Interesting conclusion:
Even though the compound can be produced from naturally occurring polyphenols in plant foods – ellagitannins and ellagic acid, the impact of direct UA supplementation on human health and its potential beneficial impact must be assessed. […] Safety, bioavailability, pattern of distribution, and mechanism of action in humans must be established. Regarding PD, given the recent advancement in detecting prodromal individuals before diagnosis and the potential prognostic value of the α-synuclein biomarker, research into selecting the right time for UA intervention shows promise to delay PD onset or progression to people at an increased risk [102]. Nevertheless, as predicted by computer modelling, low brain bioavailability of UA is orders of magnitudes lower than concentrations that provide neuroprotective effects [96], and thus should be managed by any supplementation scenario. Advanced nutritional approaches enabling the delivery of UA in a calibrated manner are likely to play a key role in bridging the gap created by the natural heterogeneity of the gut microbiome to deliver health benefits. […] In this context, UA was recently suggested as a potential biomarker of gut dysbiosis and disease stage in PD patients. Taken together, the data gathered herein support the health-promoting activity of UA. Regarding PD, UA-based intervention offers new strategies to improve the prevention, treatment, and even diagnostics of the disease.
For those who want to know more about UA, see: Urolithin A (UA) One of 4 Promising Agents 2024 by Brian Kennedy of NSU
Thanks A LOT again @Neo for pointing me towards UA! ![]()
Thanks for a good share - have you - or anyone else - seen anyway to test our levels?
The article cites this paper: Urolithins: potential biomarkers of gut dysbiosis and disease stage in Parkinson’s patients 2022
There they say:
Urolithin detection in urine is a feasible, non-invasive and fast approach that can reflect gut microbiome dysbiosis and intestinal inflammation in Parkinson’s disease patients.
Stool samples were collected for the gut microbiota analysis at baseline, while urine samples were collected for the urolithin analysis after consuming 30 g of walnuts for three days, a short polyphenol-rich intervention in which participants can produce urolithins. Urolithins were determined in urine samples by ultra performance liquid chromatography–electro spray ionization–quadrupole time of flight–mass spectrometry (UPLC-ESI-qToF-MS) as previously described.
They cite:
Ellagitannins and ellagic acid (EA) are metabolized by the gut microbiota to produce urolithins that could be responsible for the health effects attributed to ellagitannin-containing food products. Several urolithin aglycones could be present in fecal samples while glucuronide and sulphate conjugates are mainly found in plasma and urine. So far, the lack of available standards has made difficult their correct identification and quantification. In the present study, UV and MS spectra characteristics of urolithins and their phase II metabolites have been determined using different systems based on liquid chromatography (LC) coupled with diode-array or mass spectrometer detectors with different analyzers (triple quadrupole (QqQ) and quadrupole time-of-flight (QTOF)). Chromatographic separation was achieved on a reversed-phase Poroshell C18 column (3×100mm, 2.7μm). Elution order, characteristic UV spectra, and relative response factors (RRFs) with respect to their parental compound (EA) and the most common metabolite urolithin A (Uro-A) were determined. This contribution, along with the most important mass spectra characteristics (MRM transitions, qualifier/quantifier ratio, accurate mass and fragmentation pattern) will allow the determination of urolithin metabolites in different biological samples and their quantification even if not all metabolites are commercially available. The methods developed in the three systems have been fully validated in terms of linearity, sensitivity, precision, recovery, matrix effect, selectivity and stability. After that, they were successfully applied to complex biological matrices (urine, feces and plasma) from two human studies in which volunteers consumed ellagitannin-containing foods, such as walnuts and pomegranate extracts.
So you need UPLC-ESI-QTOF-MS. How much does this cost? Or can you access it from a lab?
[Update: OK 10 to 100k$: Waters SYNAPT G2 ]
Seems like something that one of the current testing companies, perhaps Jinfinity, Genova Diagnostics or Iollo could offer.
There was another source I think you or something else shared the last day or two where one could just do it from a blood spot card.
Wonder what Mitopure did for their different clinical tests. @RapAdmin did they even offer to test people’s levels in the past or something - I think I recall something like that from some post you made, but perhaps it was something else than Mitopure/UA?
I’d be ready to pay to rent a UPLC-ESI-QTOF-MS from a lab and test my sample…
I think they offered a free test to see if your gut microbiome could produce urolithin A from pomegranate juice.
https://www.timelinenutrition.com/blog/making-a-natural-anti-aging-nutrient-available-to-everyone
Yes - I still have the kit in the bedroom… did the test, but never mailed it in because I got busy with other things. See here: Urolithin A - Virtual Clinical Trial by Timeline Nutrition
I remember a podcast with one of the guys at the Buck Institute and apparently its a pretty easy, quick and inexpensive test (In the Timeline trial, you just dripped a few drops of blood on a piece of paper and sent it to them). Someone needs to create a commercial version of this test - perhaps if a bunch of us emailed a few test labs like Merek, and Life Extension foundation, they would offer it.
Interesting paper confirming the view of PD as a disease of aging: Dopaminergic neuron loss in mice due to increased levels of wild-type human α-Synuclein only takes place under conditions of accelerated aging 2024