0.80 (0.67-0.97).
20 characters.
0.80 (0.67-0.97).
20 characters.
Thanks. I asked ChatGPT: ChatGPT
Its conclusion using the Bucher method:
The estimated HR for drug Y compared to placebo is approximately 0.714, suggesting a 28.6% reduction in the hazard of outcome 1 compared to placebo. The 95% confidence interval for this indirect comparison is 0.47 to 1.09.
It’s important to note that this estimation and its CI are based on indirect comparisons and carry the assumptions and limitations associated with such methods. Ideally, these results should be confirmed with direct comparative studies.
Drug Y = atorvastatin. Outcome 1 = ACM.
So it became wider and statistically insignificant.
I would like to know why JUPITER detected ACM benefit, while atorvastatin trials doesn’t seem to. What the explanation for that is. It would require a lot of research. (Might it do with the high CRP in JUPITER?).
I like the heuristic of prioritizing drugs with ACM benefit vs. placebo.
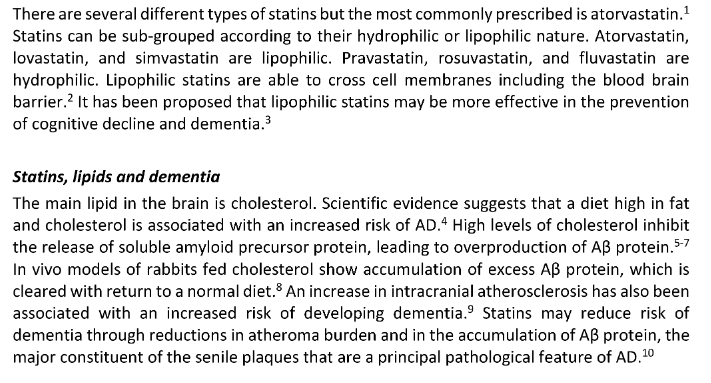
One of the other areas I look at is the controversy on hydrophilic vs. lipophilic is neurocognitive decline … there is literature showing concern for hydrophilic with increased disease progression in PD.
As neurocognitive decline is often a top worry for individuals. I’m interested in what conclusions people have made in this space - as it is another differentiator to consider between these two agents.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10141621/#:~:text=This%20study%20suggests%20that%20hydrophilic,have%20clinical%20and%20scientific%20implications.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9944858/
https://parkinsonsnewstoday.com/news/lipophilic-statins-linked-lower-risk-women-study-france/
I’m not sure what to choose for that as it’s a decision under uncertainty. Initially Attia and Dayspring had a preference of hydrophilic statins as they believed it had a lower probability of passing the BBB and reducing desmosterol of which reduced levels are at least associated with MCI. Later on at least Dayspring have said all statins cross the BBB, so it is a bit moot for AD.
Attia looked at many statin trials and they all had a neutral or positive effect on secondary outcomes for dementia IIRC. APOB seems causally linked with AD based on MR studies. So they seem positive in general (except possibly in the scenario where serum desmosterol lowers too much, especially in apoE4 carriers).
adssx maybe knows better about PD, but it seems lipophilic statins are better for this (?).
If ChatGPT’s calculation is correct then yes we cannot conclude with certainty about atorvastatin but the signal in its favor is quite strong.
Regarding neurocognitive decline, I think that obicetrapib is the most promising: Obicetrapib (CETP inhibitor for dyslipidemia)
In the absence of obicetrapib, ezetimibe is my best guess and I think that’s what I’ll start using. Reasoning here: Parkinson's disease - #89 by adssx
Some PD researchers and practicians now support statin cessation in PD patients. See also this discussion: Rapamycin and risk of cardiovascular disease - #3064 by adssx
The signal in the JUPITER trial may have been due to some subject selection bias. The massively high death rate for all subjects has never really be explained.
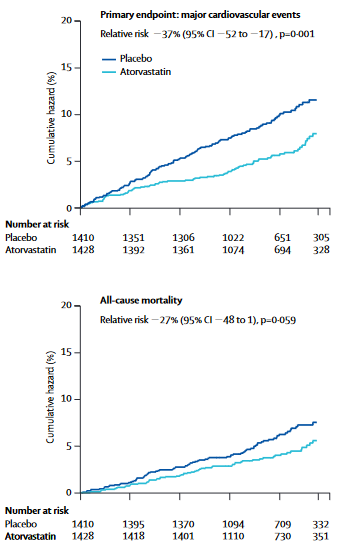
So atorvastatin 10 mg reduced ACM by 15% in hypertensive people who didn’t even have dyslipidemia (“total cholesterol concentrations at baseline of ≤6.5 mmol/L”) after 5y?
For JUPITER participants were “apparently healthy men and women with low-density lipoprotein (LDL) cholesterol levels of less than 130 mg per deciliter (3.4 mmol per liter) and high-sensitivity C-reactive protein levels of 2.0 mg per liter or higher”
So both trials are relevant to people here without dyslipidemia who want to act preemptively.
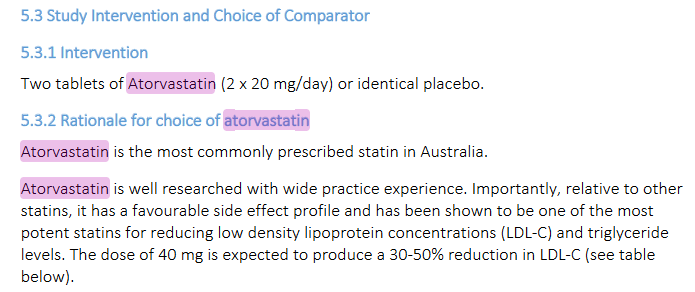
JUPITER used rosuvastatin 20 mg while the other used atorvastatin 10 mg, equivalent to rosuvastatin 5 mg. So it’s not an apple to apple comparison.
For those with diabetes or cataract (or at high risk of these conditions) then atorvastatin seems the best option.
For others: my bet is still on atorvastatin.
JUPITER is a questionable trial. It was prematurely halted and failed to demonstrate a statistically significant difference in ASCVD mortality. Although it initially indicated a reasonable reduction in all-cause mortality, the difference appeared to diminish over time. Moreover, the authors excluded data from the final months and adjusted the all-cause mortality graph, raising doubts about the trial’s reliability. Overall, it’s challenging to draw meaningful conclusions from this trial, which seems to be more about statistical manipulation than substantial evidence.
Two big red flags indeed.
What is nice in both atorvastatin trials cited above is the clear trend towards significance in ACM reduction over time.
(Actually it’s p=0.02 for ACM reduction in both JUPITER and ASCOT-LLA.)
In the UK NICE chose atorvastatin as first line because the benefit / side effect profile was seen as the best. The ASCOT trial was a big part of the evidence supporting that.
It’s worth reading the NICE protocol because it specifies when each statin is preferable for a specific individual. CKS is only available in the UK | NICE
There’s also a good nhs england pdf looking at intolerance to statins, what to test for, and what to switch to.
statin-intolerance-pathway-v2.pdf (236.0 KB)
It’s crazy that you need a VPN to read this content…
In general I find NICE recommendations well written and quite good.
Gosh you’re right, that’s insane. An example of inefficiency in a state run system. But i agree, most if what they do produce is decent.
This study halted prematurely as well, the end is a follow up, and led to the statistical significant effect, so it is a limitation (see end of LLA in the graph, which also “converged” a bit).
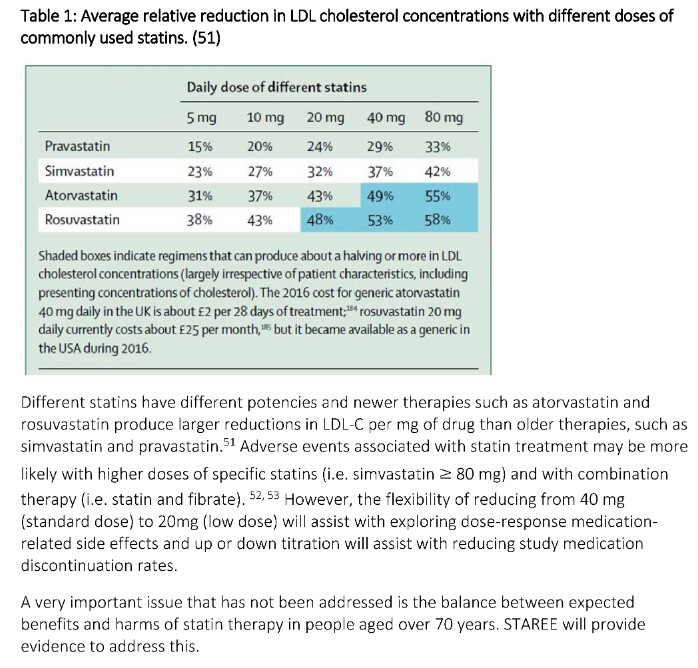
When comparing statins with more or less the same lipid-lowering properties there are still some differences in outcomes.
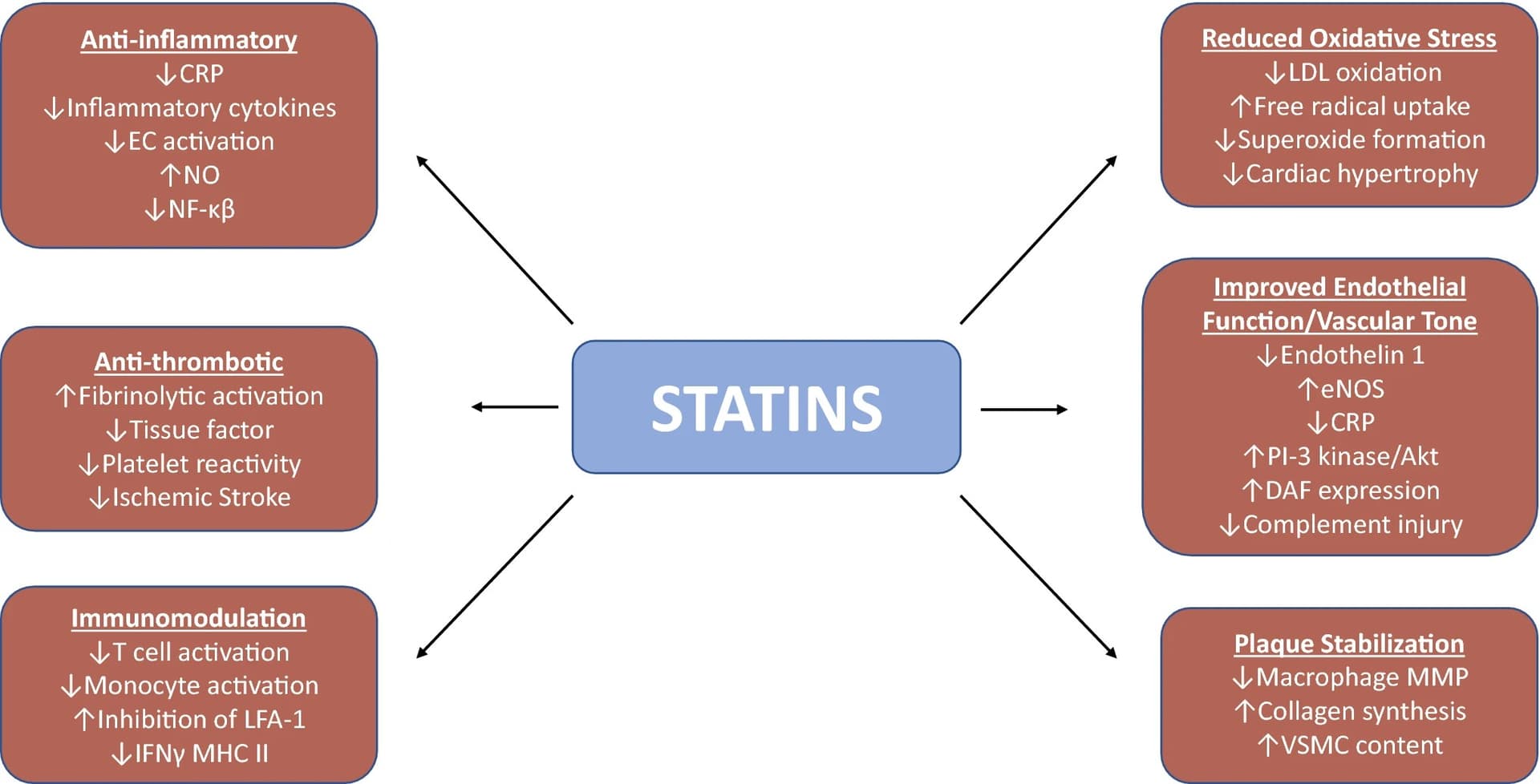
So, are there some beneficial effects from statins that are not related to their lipid-lowering properties? If so, what are the beneficial side effects of the different statins?
I understand that besides their lipid-lowering effect, statins also:
Other potential effects:
Understanding the molecular mechanisms of statin pleiotropic effects 2023
Do we have papers looking at the effects of various statins on oxidative stress, hsCRP, SPMs, and endothelial function?
The antiinflammatory affects are probably very important too. The strong short term benefit post a cvd event is probably due to those. But you make a good point, i should have emphasized that NICE regarded the evidence for atorvastatin benefit as strongest.
Each of the statins interact with different liver enzymes which may partially account for different side effects.
colhoun2004-1.pdf (198.9 KB)
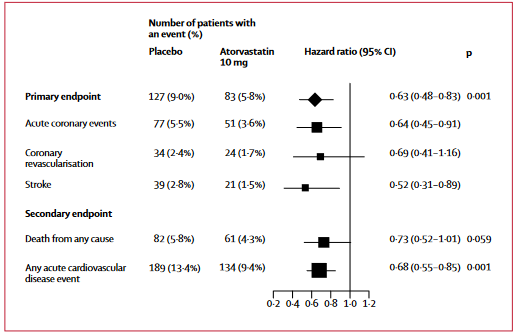
P=0.059 so technically not statistically significant, but I am pretty much convinced that atorvastatin reduce all-cause mortality in primary prevention for heart disease.
I did try 20 mg atorvastatin for a few days but I switched back to rosuvastatin. I will try again since the drug pretty much reduces all-cause mortality, all statins cross the BBB, and more importantly it has a lower causal risk of diabetes compared with rosuvastatin. If it wasn’t for the latter I wouldn’t try and switch.
The STAREE trial and STAREE-MIND trial chose 40 mg atorvastatin as well for its research, reading a bit in the supplementary information, they cite research which suggest lipophilic (meaning drugs that can pass the BBB), might be superior for dementia and as many of us know APOB causes Alzheimer’s according to MR studies.
bmjopen-2023-April-13-4–inline-supplementary-material-3.pdf (2.9 MB)
Meanwhile, until we know more about Lipitor vs. Crestor for dementia and Alzheimer’s, for example in E4 carriers of APOE, I think Lipitor is probably better based on current information. The STAREE trial should tell us more? (vs. bempedoic acid, PCSK9i and ezetimibe, I still think statins have more data like for mortality and net benefit, thus they are right now superior?).
Alongside a very likely decrease in all cause mortality, statins like atorvastatin seem good in reducing stroke, that does often reduce healthspan significantly I think, even if they are non-fatal.