Thanks, I didn’t know. 50 mg/kg in rats: Quercetin administration abrogates the Parkinson’s disease (PD)-like motor and non-motor symptoms and attenuates the behavioral, neurochemical and biochemical deficits induced by rotenone toxicity in rats - MDS Abstracts
Unclear benefits per this poll though: Nutrients | Free Full-Text | Parkinson Symptom Severity and Use of Nutraceuticals
(but probably low risk as well, so good bet?)
I haven’t read everything yet, but: “Their re-examination points towards some results suggesting positive effects, but these findings will require further investigation. A parallel clinical trial of nilotinib (supported by Cure Parkinson’s and Van Andel Institute) did not find the same results and indicated that the drug was insufficiently accessing the brain. […] It is important to understand that these studies involve re-analysing data in a biased fashion – searching results for any interesting correlations or effects, and as such, these investigations should be considered as ‘hypothesis generating’ exercises. Researchers use these sorts of analyses to find new ideas for experiments that can then be tested, and further research will be required before isradipine or nilotinib can be re-examined in people with Parkinson’s.” ( Post-hoc analyses of the isradipine and nilotinib trial results - Cure Parkinson's ).
What’s the relationship between quercetin and nilotinib/dasatinib btw?
If you’re already taking lithium, then you may need to change your dosage if you start an SGLT2i (see: Starting empagliflozin or dapagliflozin in patients on lithium? Monitor lithium levels )
What’s your current lithium dose? This trial suggests 30-45mg/day, “slowly titrated in each patient up to the maximum tolerated dosage in this range”: CTG Labs - NCBI
Regarding Nilotinib, I guess we’ll soon get the results of this trial, which may help you to make a decision: CTG Labs - NCBI
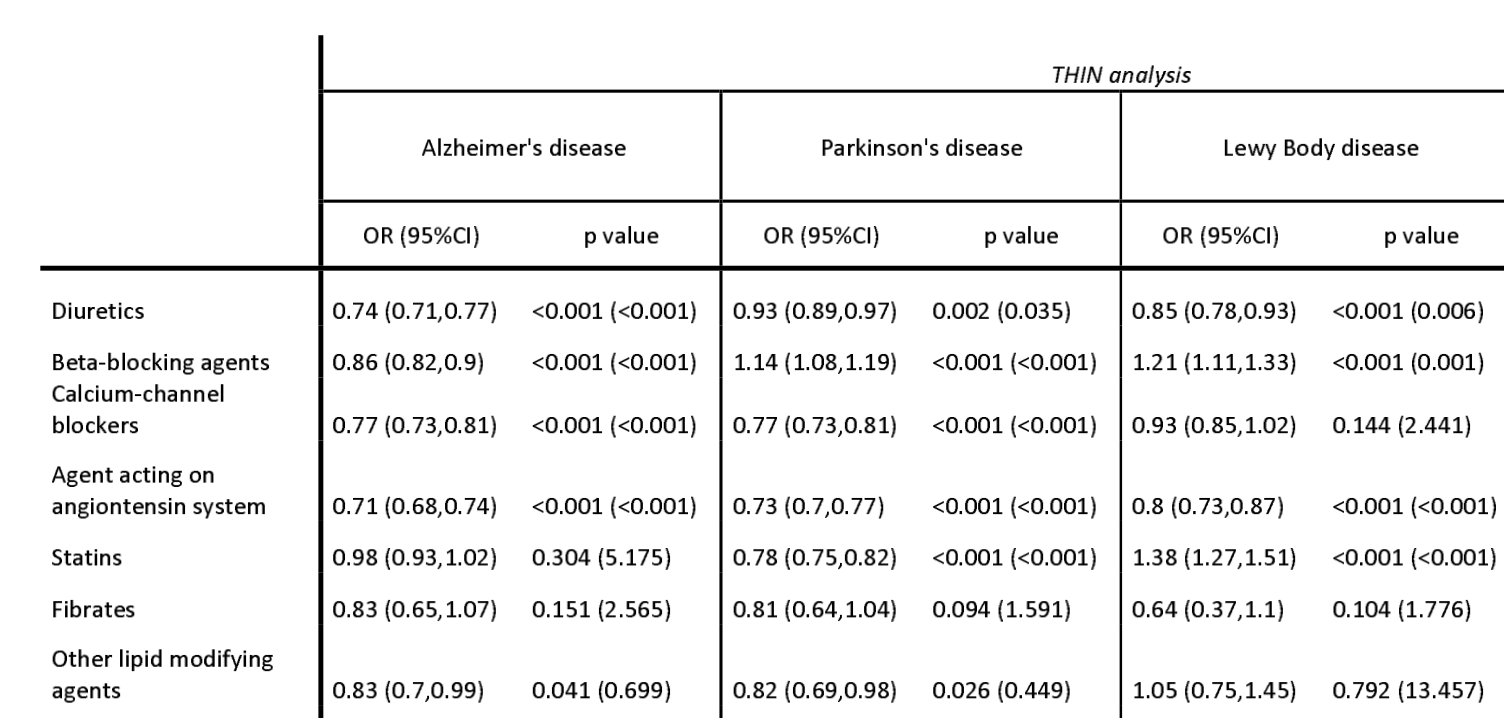
Also: have you checked your blood pressure? (see thread: Optimal Blood Pressure we Should Target? Systolic Under 110 or 100? ) I wonder whether lowering mean BP AND BP variability can decrease PD risk (for instance with an ARB/sartan or a dihydropyridine calcium channel blockers like isradipine).