
Jeesh. Do you feel better right away, or just generally think it slows progression? It just looks so painful.
I get in the hot tub most nights and try to get my pulse up to at least 110, then jump in the “cold” pool after, but to me, “cold” can’t be anything under about 72 degrees F.
Maybe you say it somewhere, but if you don’t mind, would you tell me what other drugs/supplements you take? Thanks!
I saw this post on twitter a few weeks ago, but have not had a chance to dig deeply into it. Christine is a local and very active Longevity Biotech startup person here in San Francisco, and founder of Longevity Global and NeuroAge Therapeutics, a company focused on therapies to treat Alz. in new ways. Related article on her company: NeuroAge Therapeutics: A New Approach to the War on Neurological Disease - Spannr
Christine’s bio is here: Christin Glorioso, MD PHD - Berkeley SkyDeck | LinkedIn
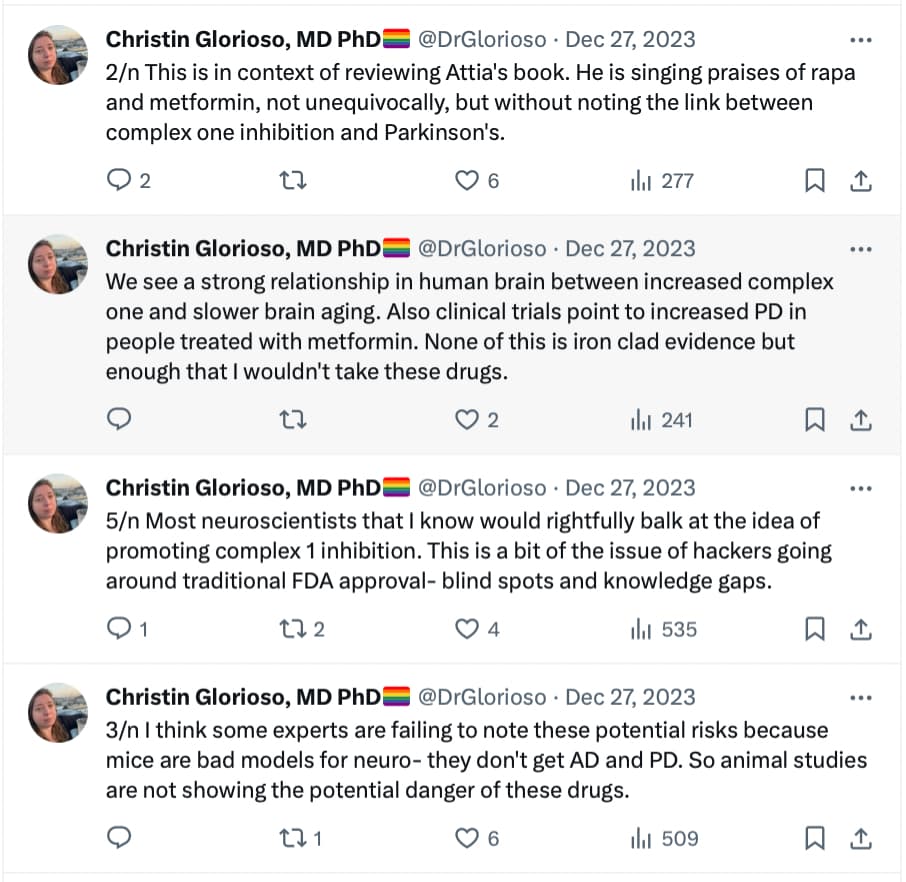
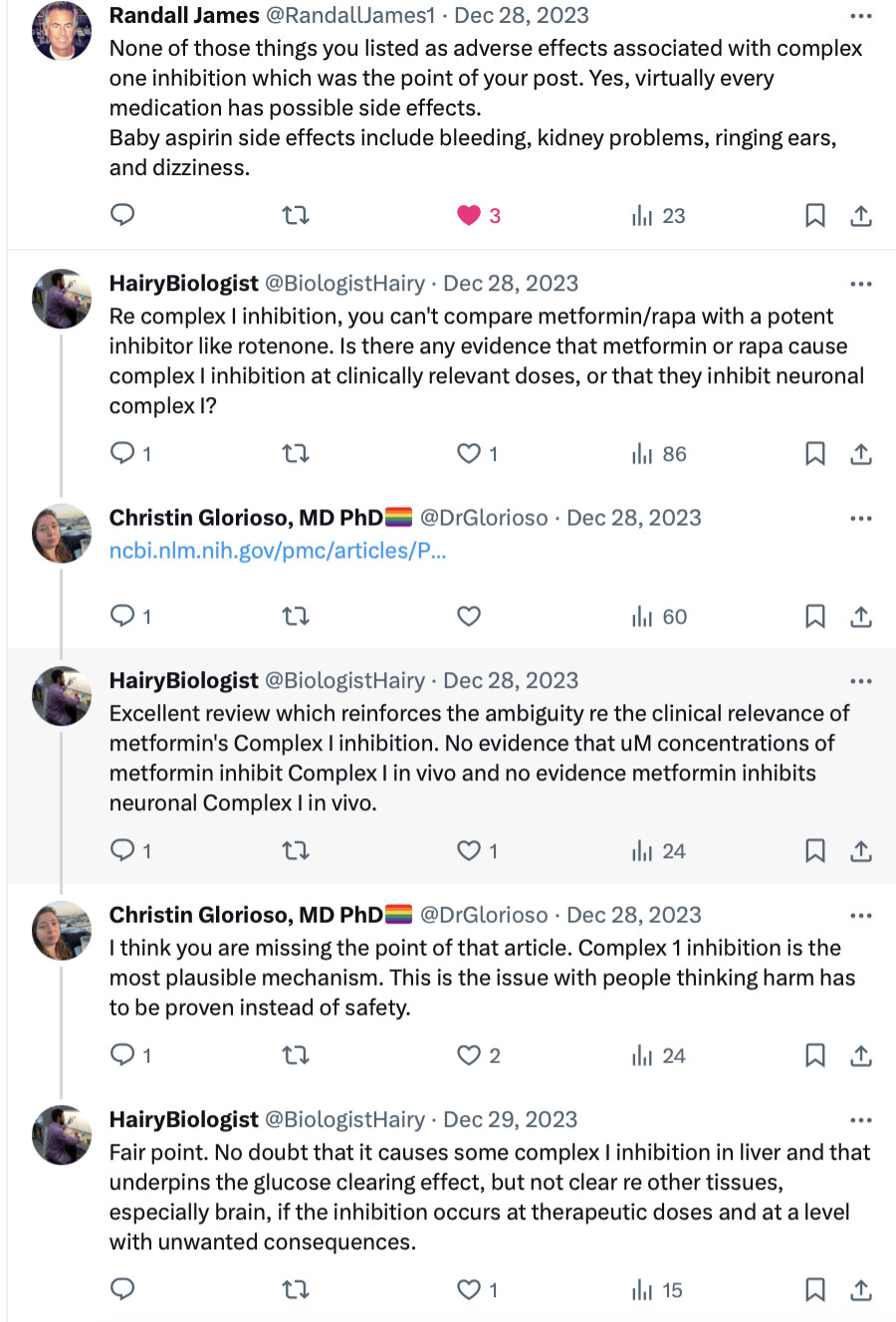
Perhaps someone here with deep knowledge of Mitochondria complex 1 can comment on her points here?
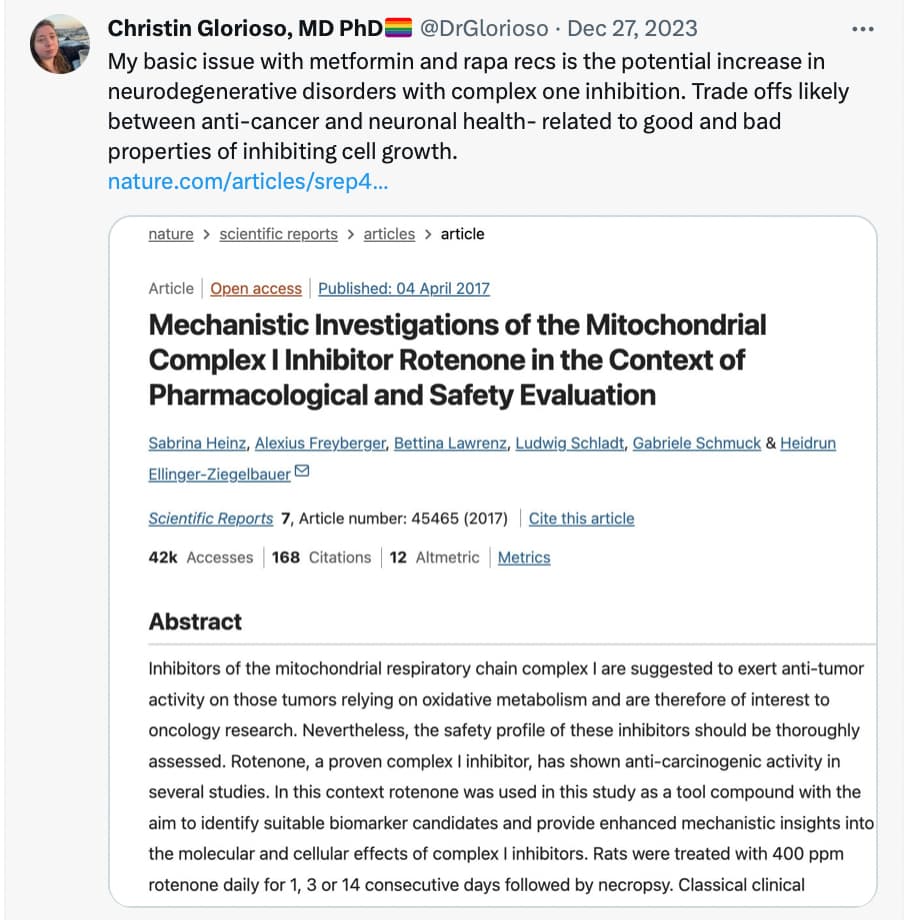
The paper referenced: Mechanistic Investigations of the Mitochondrial Complex I Inhibitor Rotenone in the Context of Pharmacological and Safety Evaluation | Scientific Reports

Another paper referenced:
Shouldn’t a signal have emerged for metformin and alzheimers disease already if there was any link? Or rather aren’t there any clinical trials looking at alzheimers patients and metformin use?
I think that the signal might be very hard to identify given the historically ill nature (typically obesity, diabetes, etc. for long periods of time) of the patient population, it would be hard to tease out of the data. If you have diabetes you are already at much higher risk of Alz.
So, if you have diabetes, you get Alzheimers. If you take Metformin, you treat the diabetes but you still get Alzheimers. Damned if you do. Damned if you don’t.
I’ll go with the no diabetes and take my Metformin. It also prevents fatty liver.
I am sure that many of the kidney transplant patients taking rapamycin also were taking metformin. Yes, if there was a significant increase in PD or Alzheimer’s disease I think it would have been detected by now as both drugs have been in widespread use for decades.
Somehow, I find this kind of post by Christin Glorioso very annoying and I want to say. post some direct evidence or be quiet.
The link between PD and metformin has been detected long ago. See, for instance: RENEWAL: REpurposing study to find NEW compounds with Activity for Lewy body dementia—an international Delphi consensus 2022
Meanwhile, several epidemiological studies have found associations between use of metformin and lower incidence of either all-cause dementia, AD or PD [152,153,154,155,156,157]. However, not all epidemiological studies have found associations between the use of metformin and a lower risk of dementia [158,159,160]. A study using the National Alzheimer’s Co-ordinating Center database investigated the effect of oral hypoglycaemic drugs on longitudinal memory decline among patients with T2DM with either normal cognition (n =1192) or with AD (n =807) and found that metformin was associated with better memory performance in non-demented participants (mean duration of follow-up 3.4 years) but it had no effects in AD (mean duration of follow-up 1.9 years) [161]. A systematic review and meta-analysis of observational studies testing the association between metformin and neurodegenerative diseases analysing a total of 19 studies with 285,966 participants found no association between metformin exposure and incidence of all subtypes of neurodegenerative diseases, and found that metformin monotherapy was associated with an increased incidence of PD compared to non-metformin or glitazone users (OR 1.66) [162].
The reason for the discrepancy between studies (besides the difficulty to separate the effects of diabetes from the effects of the drugs, but with a lot of data, comparison to other diabetic drugs, and genetic mendelian randomization, researchers now know how to do that properly) is probably that the effects of metformin seem dose-dependent (“The dose makes the poison” as the saying goes…): Dose–Response Association of Metformin with Parkinson’s Disease Odds in Type 2 Diabetes Mellitus 2022
Metformin was associated with PD odds in T2DM in a dose–response association manner. Patients who received low dosage and intensity of metformin use were associated with lower odds of PD, while higher dosage and intensity of metformin use had no neuroprotective effect.
What they call “low-dose” in the paper is <10 DDD/month so < 20 g/month, meaning < 0.650 g/d. But they also say that you shouldn’t take more than 300 cDDD = 600 g ⇒ 0.550g/d over 3y or 0.3g/d over 5y (as the study looked at people over a follow-up period of 3 or 5 years).
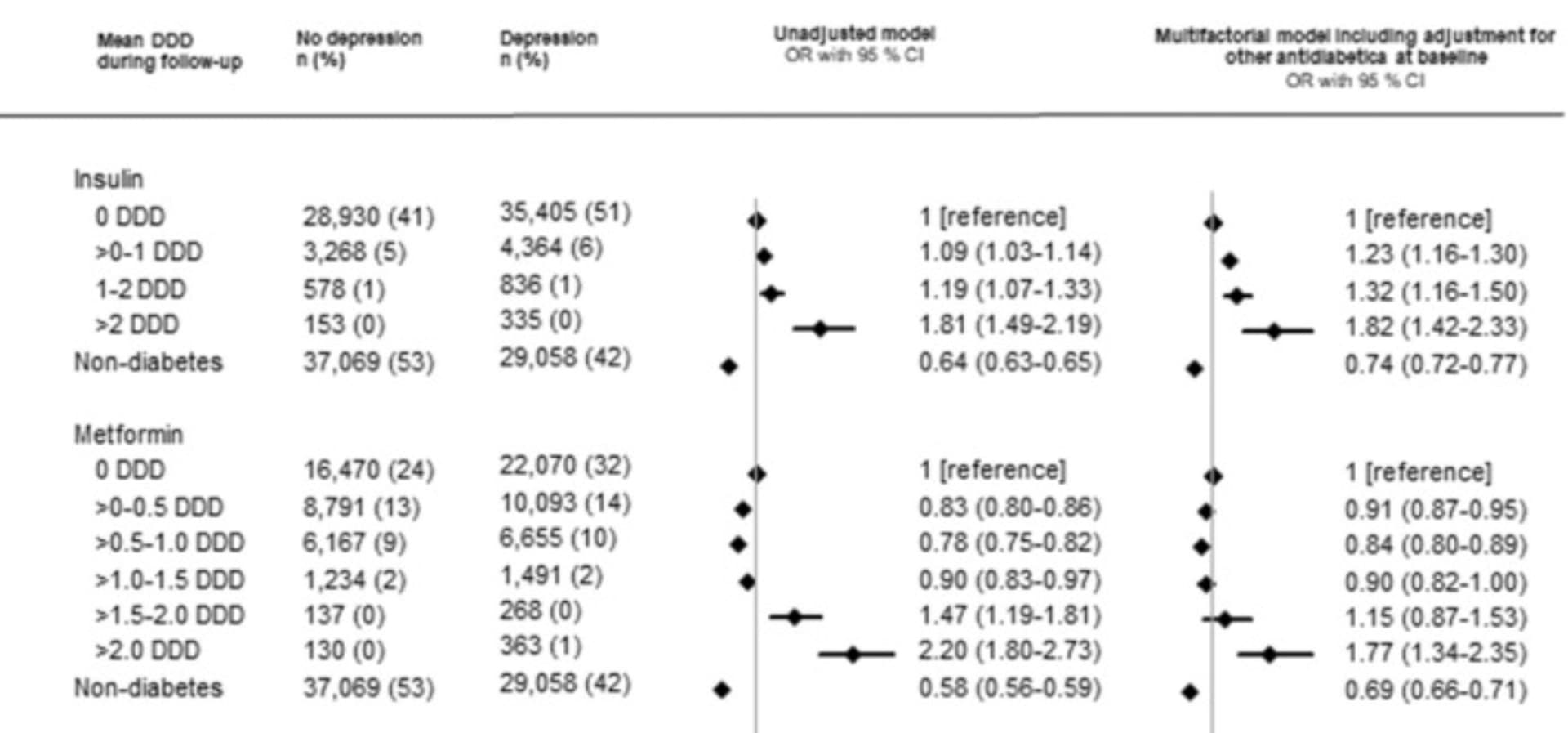
You find the same dose-dependent relationship between metformin and depression (and depression is often an early symptom of Parkinson’s / "pre-Parkinson’s), but with slightly higher thresholds (the optimal here is 0.5–1.0 DDD so 1 to 2g/day of metformin): Diabetes, antidiabetic medications and risk of depression – A population-based cohort and nested case-control study 2022
So yes, the risk is well known. I would not take metformin if I had any family history of Parkinson’s disease (or related genes). Especially as we know more potent and safer alternatives. GLP1 agonists and SGLT2 inhibitors are associated with lower rates of AD, PD, other dementia, and depression in most longitudinal studies on humans:
- “GLP-1a (0.44 [0.25–0.78]) and SGLT-2i users with dementia (0.43 [0.23–0.80]) experienced lower mortality compared to non-users.” (Glucose-Lowering Medications and Post-Dementia Survival in Patients with Diabetes and Dementia 2022)
- Sodium-Glucose Cotransporter 2 (SGLT2) Inhibitors vs. Dipeptidyl Peptidase-4 (DPP4) Inhibitors for New-Onset Dementia: A Propensity Score-Matched Population-Based Study With Competing Risk Analysis 2021
- Meta-analysis of Association between Newer Glucose-Lowering Drugs and Risk of Parkinson’s Disease 2023
- “In a post-hoc analysis using the non-diabetes population as reference, patients with diabetes using SGLT2 had even lower odds of depression compared to individuals without diabetes” (Diabetes, antidiabetic medications and risk of depression – A population-based cohort and nested case-control study 2022)
- (only dapagliflozin among SGLT2i) The potential antidepressant effect of antidiabetic agents: New insights from a pharmacovigilance study based on data from the reporting system databases FAERS and VigiBase 2023
These findings were confirmed in several rodent models, for instance:
- Empagliflozin repurposing in Parkinson’s disease; modulation of oxidative stress, neuroinflammation, AMPK/SIRT-1/PGC-1α, and wnt/β-catenin pathways 2023
- Empagliflozin attenuates neurodegeneration through antioxidant, anti-inflammatory, and modulation of α-synuclein and Parkin levels in rotenone-induced Parkinson’s disease in rats 2022
- Dapagliflozin inhibits the activity of lateral habenula to alleviate diabetes mellitus-induced depressive-like behavior 2023
Even better, we have three good-quality phase 2 clinical trials showing that 3 different GLP1 agonists (exenatide, liraglutide, and lixisenatide) slow down the progression of Parkinson’s disease. And one clinical trial showed that empagliflozin (SGLT2i) improved MCI: Empagliflozin Improves Cognitive Impairment in Frail Older Adults With Type 2 Diabetes and Heart Failure With Preserved Ejection Fraction 2022
I don’t know about rapamycin but there are two trials for AD (NCT04200911, phase 1 done, and NCT04629495, ongoing phase 2), both in Texas). And rapamycin was shown to have no effect (neither positive nor negative) on MSA: mTOR Inhibition with Sirolimus in Multiple System Atrophy: A Randomized, Double-Blind, Placebo-Controlled Futility Trial and 1-Year Biomarker Longitudinal Analysis - PubMed
So the jury is still out on rapa for NDD… (my two cents: given that diabetes is protective of PD and that rapamycin increases Hb A1c, I would not be surprised if rapamycin, alone or in combo with a GLP1RA or SGLT2i, would be highly protective of PD, but that’s a pure guess…)
Here’s an article from a trusted source providing observational study data that shows metformin can prevent dementia. I’ll take that over a tweet.
I think Metformin is a terrible drug for people who aren’t in the diabetic/pre-diabetic range because it is a mitochondrial toxin with a significant effect, it decreases zone 2 wattage and increases resting lactate. I would use a drug proven in ITP instead.
Did Peter Attia really sing the praises for metformin in his book? He disregards it everywhere else.
Heard that Mucuna Pruriens helps people with Parkinsons. I take it for mood improvement but and it really helps, but don’t know about Parkinson’s but could be worth a try.
Is Mucuna pruriens any better than taking L-dopa directly? L-dopa effectiveness gradually decreases in people with Parkinson’s and they need higher and higher doses, while levodopa also comes with side effects such as bradykinesia.
Never tried L-Dopa so couldn’t say about difference…
I can’t find the links now but back when I did a deep dive on metformin I came away satisfied that all its potentially negative effects on Parkinson’s and other neurodegenerative conditions could be accounted for but its property of severely impairing vit B 12 absorption and availability which has downstream consequences for neuronal myelination, cholinogenesis etc.
You can probably find the actual link somewhere in the intersection of these:
https://scholar.google.com/scholar?hl=en&as_sdt=0%2C20&q=Parkinson+vitamin+b12+deficiency+&btnG=
https://scholar.google.com/scholar?hl=en&as_sdt=0%2C20&q=metformin+vitamin+b12&btnG=
So anyone taking metformin should pair it with megadoses of Vit B12. That’s exactly how it’s bundled in one of those US based longevity focus online pharmacies. Once you take care of vit B12 depletion there doesn’t seem to be any other side effects from metformin.
……unless you’re also taking miglitol (or acarbose, if it’s a class effect) with your metformin.
I’ve posted about this before (see link below), but didn’t get any replies
For all those who use metformin and alpha-glucosidase inhibitor
Well, the little bit of Sinemet I take (100mg before my exercise class and another 100 later if I am going somewhere fancy, like a party) makes me so nauseated I can’t imagine taking mucina. It may be “natural” but it’s missing the carbidopa that keeps the dopamine from activating before it gets to the brain.
Have you tried quercitin? I think it might help. Also, I take ambroxol (though I have a GBA mutation so I believe it makes particular good sense for me) and also, exenatide. I’m thinking about dasanitib, though with the quercitin plus rapamycin I wonder if it’s overkill.
Basically, I look for phase 3 trials and (since I never seem to qualify) duplicate them myself if I can. But I don’t care so much about symptoms as I do about progression.
What do you consider an appropriate megadose of B12?