No grapefruit juice.
Sorry for the long post, this is me, more-or-less, thinking out loud.
Yeah, my proposed dosing schedule is definitely on the conservative side of things. However, we don’t know enough IMHO of this drug, long-term, like 10-30 years. Yes, it’s unlikely my parents are going to make it another 30 years, but still–until we see large-scale, double-blind placebo studies, there’s still a risk, even if I think (or maybe a better word is “feel”) the risk is around 10% that there is a severe side effect lurking under all this seemingly good news, there’s still a too high of a risk for my (maybe overly conservative) conservative mind… Sure, Rapamune has been FDA approved since 1999, and typically given at 6mg on the first day, directly after organ transplant, then 2mg/day after that, then the dose is adjusted after 10-20 days, ending at some point after–month or 2?.. So, that’s great news it has been 24 years since FDA approval… But not hard studies on 6-8mg/week, for a year straight. Really, nothing even close to that in humans.
I just don’t want something to happen to them in 5-10 years, and something somehow points to Rapamycin–I couldn’t live with myself. We just don’t really have enough definitive results. And mouth sores & pimples & rashes all seem like the immune system is being negatively impacted–something that rarely happens at these lower, more conservative numbers.
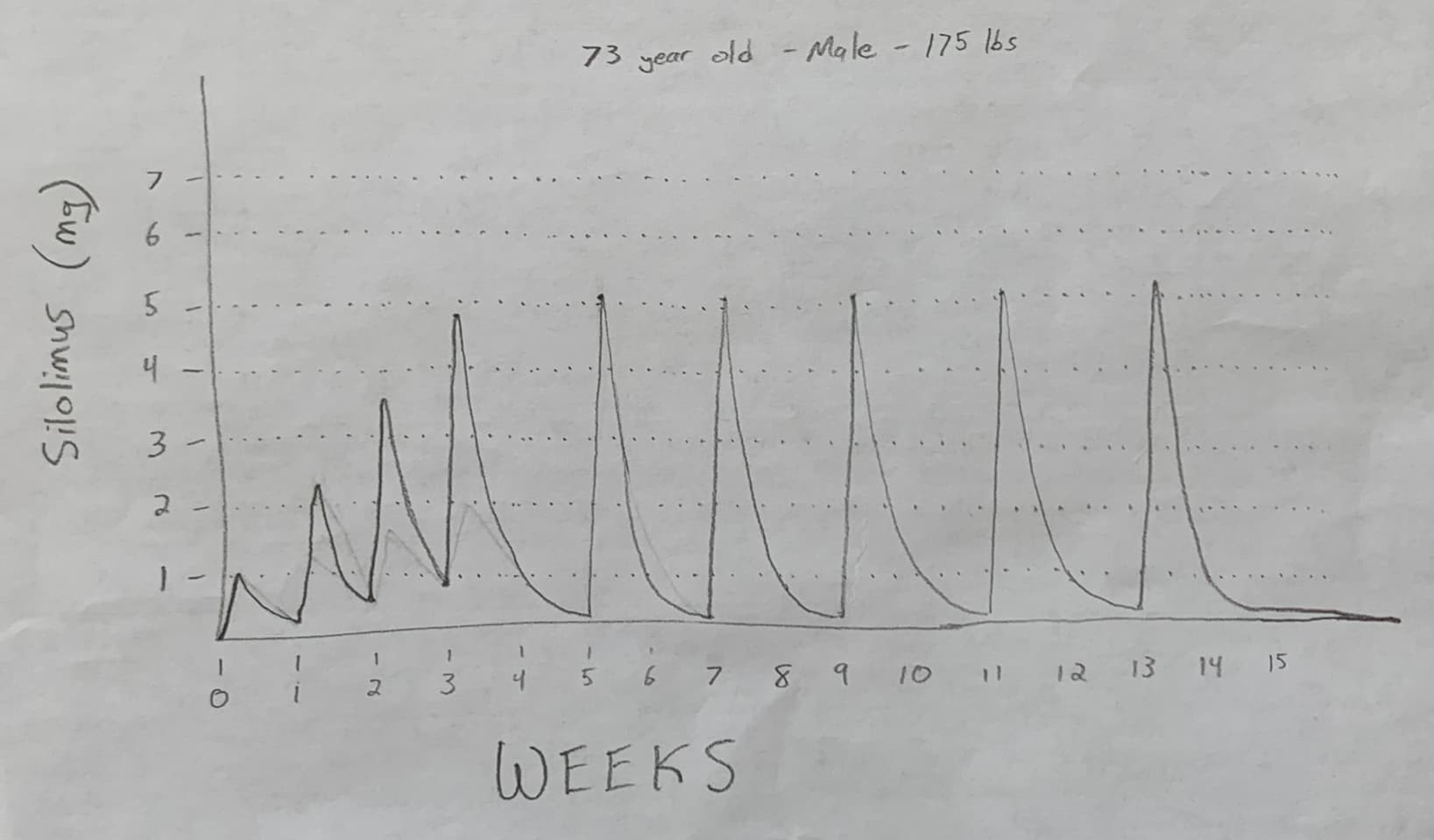
Also, I saw a video regarding how the modulation of mTORC1 is key–I believe by a guy named Bryan? Can’t find it. But that made sense to me, and if that’s true, then with such a long half-life of 60 hours, there is still 10-15% remaining in the blood if taken weekly, not allowing the body to ‘live’ with a lower %'s in the body for long enough, IMH (and non-medical mind) Opinion.
But more than all that, I just don’t want to do more harm than good, as it’s not my body, it’s my parents. I will let them know they have the option to increase it beyond this conservative starting point if they want to, and I have shown them the polls on this website showing how 75% take it weekly.
Or, perhaps have them take it every 10 days as a nice ‘happy medium.’ Don’t know.
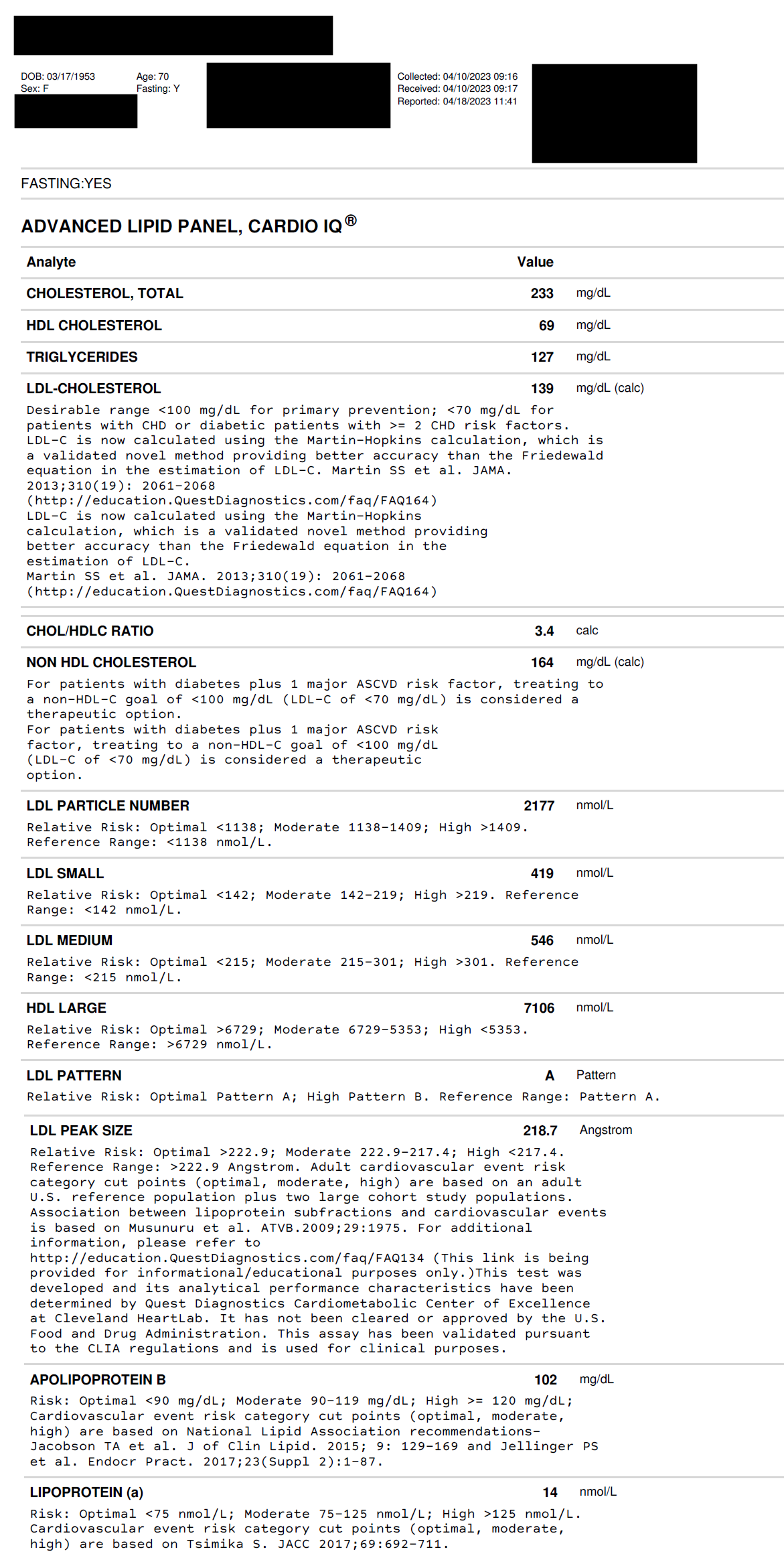
If anyone has any suggestions on exactly the bare minimum of ‘before tests’ to do, please let me know. At this time, the only thing they have done is a lipid test from 6 months ago during their annual check-up/blood draw. I just don’t know where to start. The Sirolimus Zydus in en route, shipping via India Post - so I probably have 1-2 weeks to figure this all out.
It’d be ideal if there were, like, 3 options outlined that the collective genius on this forum could more or less agree on. For example, 3 lists of pre-test/biomarkers before starting Rapa:
- Lower data, bare minimum looking at the most important numbers, mainly for safety, lowest cost
- Medium data, little more data, little more cost
- High data, tons of data, to get a full-meal-deal on all the potential benefits Rapa may have, costs the most
Then new users can choose their own adventure on how much data they want to log.
Also, where to get these? Do we just go to our family doctors and hand them a list? Or are these tests ordered online? This is where my ignorance shines bright, and something like this would make the ‘next steps’ more obvious for new users.