It seems like a good plan. Definitely do not do grapefruit juice. That is playing with fire. Fine if it is for you, but I would never do that to my parents. The bioavailability of rapamycin varies greatly among individuals. When you add grapefruit juice, you are just compounding the problem.
2 Likes
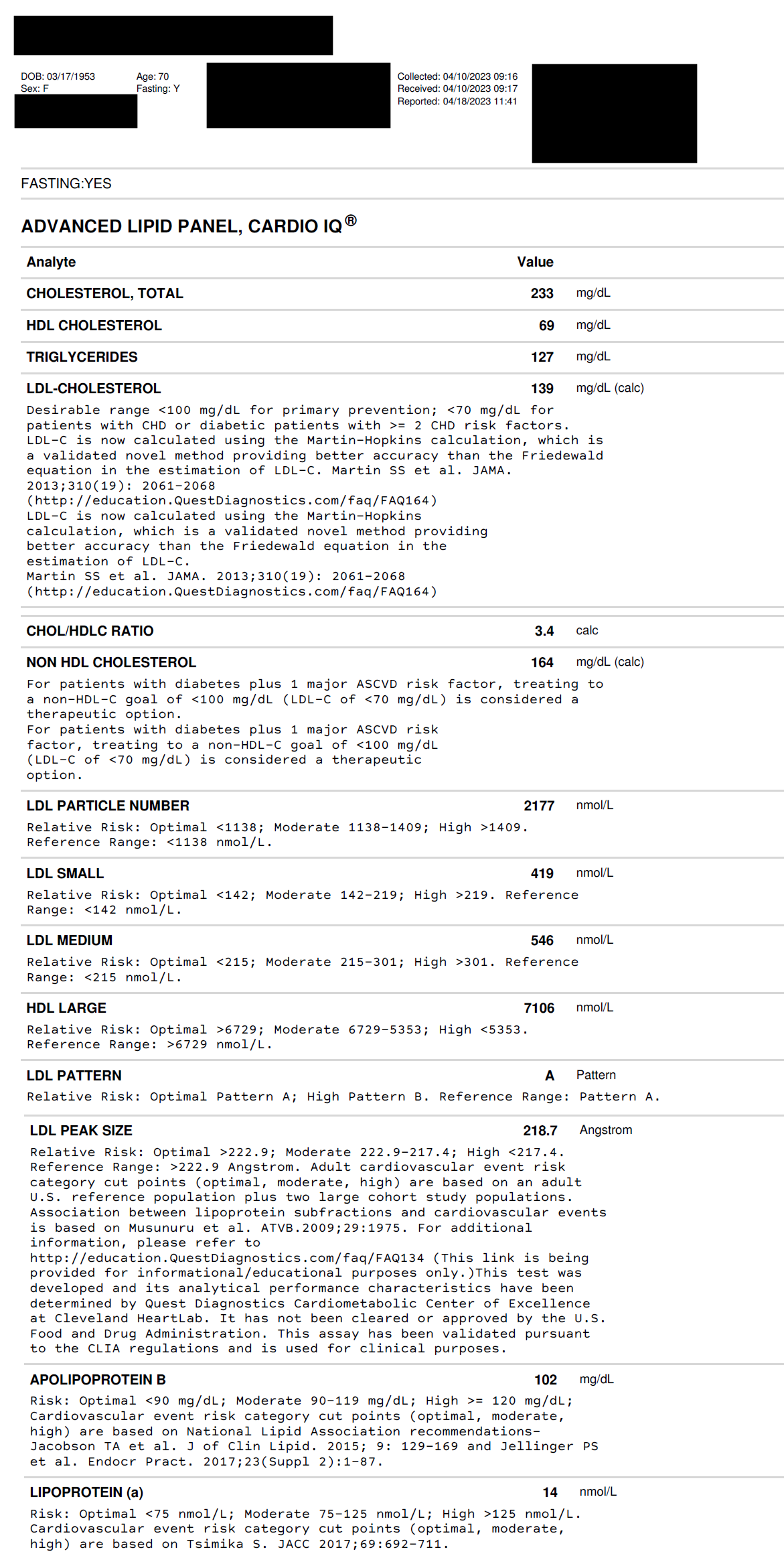
Here is my mother’s blood just done a few days ago.
Would this be considered ‘bare minimum’ of tests to be done before starting Rapamycin?
1 Like
Well, obviously there is not hard and fast rule on what the minimum is. I tend to think that at a minimum you want the information provided by CBC and hsCRP blood tests. This at least allows you to track ongoing biological age testing results using the free Levine Phenotypic Age Calculator (out of Yale), and the Aging.AI biological age calculator. I wouldn’t put a ton of value in the absolute values these calculators provide, but they at least provide a good tracking mechanism to gauge how things are going over time, based on some solid science. I would be more interested in how things change over time, than the absolute numbers.
More details here: A Friendly, Biological Age Reduction Competition?
4 Likes
I think it is great what you are doing. Do keep in mind that I believe it is technically against state and federal laws to give prescription drugs to others (without a medical license). Obviously your parents would not cause you a problem, but one never knows what sort of busy-body person might. Possibly even a family medical doctor if they were irked at losing control of their precious “power of prescription”, or, for instance, the person you gave the Rapamycin to ended up in the ER for something unrelated but reveled they were taking this prescription medication that you gave them. Maybe the ER doctor is legally required to inform the police, who knows. My own policy is to tell only very close family and friends exactly how I have purchased Rapamycin, but to let them buy it themselves.
Being prosecuted is probably an outlier, but I tend to be a bit careful about such things in this crazy world.
5 Likes
I think you may be talking about the following video. Dr. Brian Kennedy covers the mTOR modulation issue in this video here, queued up to the discussion on mTOR modulation:

4 Likes
ad. 1 I would do Levine blood panel markers (google it or search this forum, there is a lot debated about it, here is the link to spreadsheet)
ad. 2 I would take http://aging.ai/ their Aging.AI3.0. blood panel with 19 parameters (you can take the blood test anywhere just use their website to evaluate results, which is free)
additionally I would test lipoproteins, apoB and apoA1 and glucose (especially HbA1c test)
this two would give you a good insight IMO.
Regarding rapamycin dosing, this is highly individual. But there are common wisdoms I gathered reading this forum, podcasts, twitter and research papers is that you should take the maximum dose without unwanted side effects (you need to test this in vivo) and space the doses that your level of rapamycin before next dose is almost zero not to suppress MTORC2 all the time. If you space doses to two weeks, you can take considerably higher dose than weekly.
This post below can give you an idea what experts and rapamycin researchers are taking and their schedule. In any case it is worthwhile monitoring blood biomarkers while taking rapamycin and I would consider testing the trough level of serum rapamycin at the end of dosing period too to see that you are not suppressing MTORC2, but other biomarkers and probably side effects and rise in bacterial infections would be a telltale sign that the dose is too high or spaced too close. One can also take vacations from rapamycin (eg 8-12 weeks on / 4 weeks off) to make sure immune system is not inhibited.
3 Likes
btw how did you get to 6mg/week for your dog? If I am not mistaken the dosage for dog in Dog Aging Project TRIAD Study is roughly 0,15mg/kg… if your dog is around 18-23kg (I googled average weight of golden doodle) you are looking at 2-3mg per week.
3 Likes
You need a good baseline. That’s just the lipids.
Getting at least the phenoage biomarkers is a good idea.
Albumin ALP Creatinine Overnight fasting glucose CRP Lymphocyte % of total WBCs WBC (total) MCV RDW
1 Like
I would say an absolute minimum is a full blood count (FBC) just to ensure that the immune system is in good working order and not already compromised in any way.
1 Like
My dog weighs 70 lbs, and read 2mg/20lbs once every week, so figured 6mg/week.
1 Like
You should check your hip mobility. Often these issues are related to lake of internal rotation mobility in the hip. See a good PT.
1 Like
Why did you decide skipping Rapamycin every second week after reaching the desirable end dose for your parents? Why not to continue with the dose on a weekly basis?
1 Like
That is some heavy pooch ![]() 5mg is more correct using 15mg/kg formula I guess.
5mg is more correct using 15mg/kg formula I guess.
I want very minimal side effects regarding mTORC2 inhibition. I find this to be a good starting point, “ooching” into this Rapamycin off-label new world.
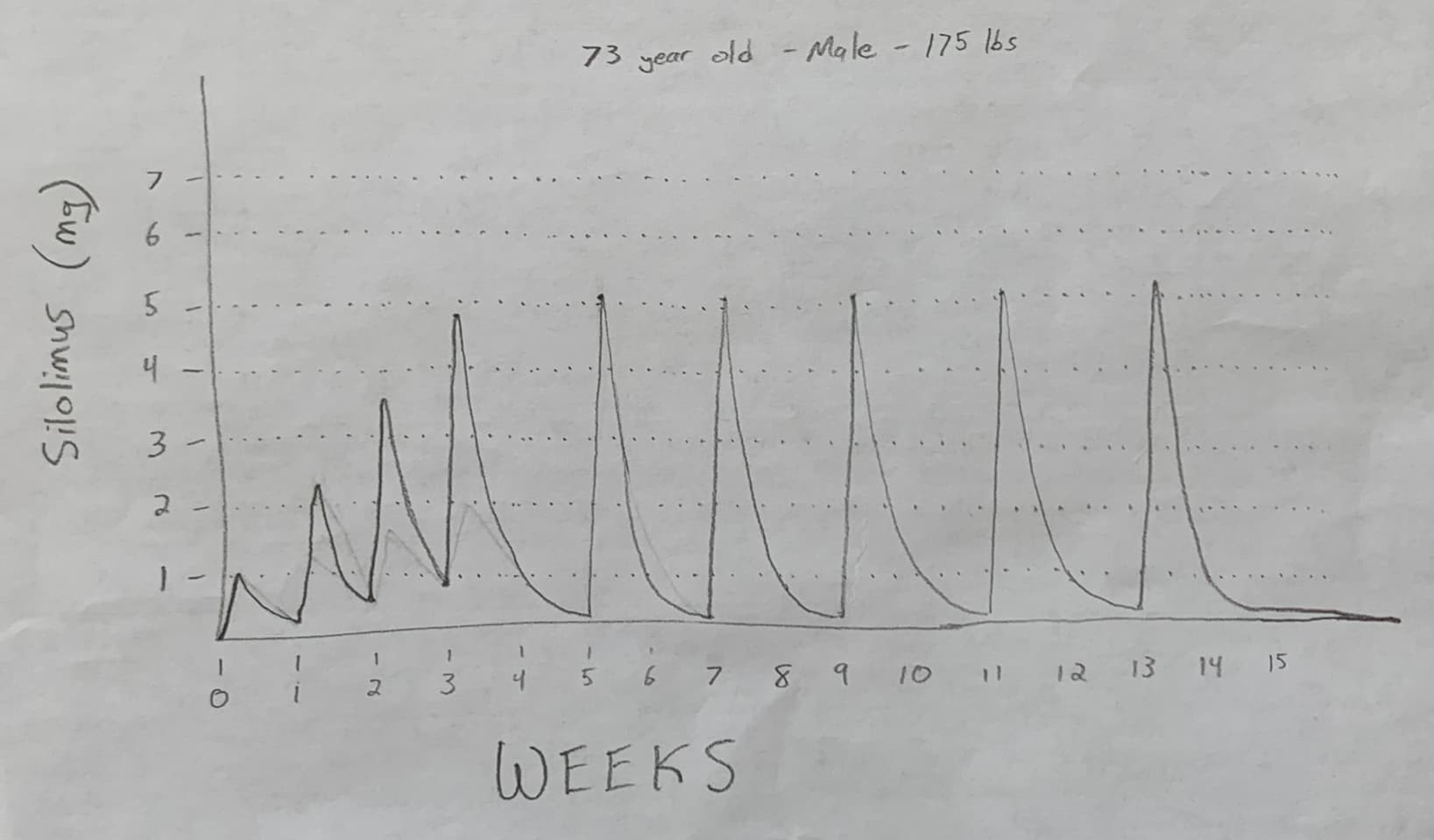
See sketch below. I understand bioavailability is different from the pill’s mg’s—but this is the idea/trend I’m going for. Shoot holes in it.
Look it is not right or wrong, 5 mg every two weeks is a very conservative dosing. But we have no idea what is the correct dosing. If we keep with aging dog study the human dose would be something like 10mg every 10 days, 7mg every 7 days or 14mg every 14 days for a 70kg male respectively or 7mg every 10 days, 5mg every 7 days or 10mg ever two weeks for a 50 kg female. This is also what most experts use. This would be a good guidance. You want as high dose as possible to inhibit MTOR but give enough time between doses to keep MTORC2 not inhibited all the time to keep immune system running. The older you are the more you want to supress MTOR, hence older you are the higher dose would be rational. Finding a good balance between both is a fine personal balance and needs some experimenting. Even transplant patients make fine adjustments on how they react to rapamycin and how they metabolize it and side effects they experience.
I myself was considering 10 days spacing between doses as in my regard gives you this fine balance but it is highly impracticable and difficult to remember and stick to schedule. My next thought was two weeks between doses but since taking first dose of 1mg I experienced really not pleasant effects I did not want to take it to a very high dose so I stick now at 5mg weekly and do not plan to increase that for a while. And I feel this is a conservative dosing and schedule.
4 Likes
100%
I’ll leave it up to my parents to increase their 2 weeks dosing, and I’ll start them off very conservative. I’d rather start erroring on the too-low vs too-high.
If they want to increase up to 8mg/2 weeks, or 10mg/2weeks, up to them on regarding how they feel, and what their bloodwork is looking like.
Dr Alan Green is at 2 week dosing and he is 79, and has been taking it and prescribing it for ~7 years… And he is only 6 years older than my pops. So, every 2 weeks seems optimal starting point.
Here’s one option for your idea to help you remember taking it every 10 days:
- Every month take it on the: 1st, 10th, 20th, then 1st again—repeat.
- Setup recurring reminder in your smart phone for these 3 dates every month.
- Sure, February you’ll go 8 days, and other days you’ll go 11 days, but likely close enough.
1 Like
In terms of shooting holes if the half life is 60 hours (worth working on its a usable figure that is probably not too far out) then it does not go that low after the 5mg dose.
Three half lives is 7 1/2 days, that would be 1/8th of the original dose. 5/8=0.625mg.
Your chart seems to imply something like 0.1mg
Obviously also the 1mg then becomes 0.125mg and your chart implies something like 0.25mg.
1 Like
Yah, true you’re right about the “ramp up” area—the troughs or “valley’s” should be a little lower, however the “peaks” seem correct.
During the 2 week dosing though, it’s actually around 5.5 half-lives in 14 days, so that’s about 2%. So 5mg x 2% = 0.1mg.
So the 2 week dosing peaks & valley’s seems correct to me still.
But yah, the ramp up’s valley’s seem slightly off.
The main thing is that it doesn’t go down that far in a week. Two weeks is indeed about 1.5%.
Obviously the half life is likely to be different for different people and it may not have a smooth exponential decay.
1 Like
Thanks Admin.
Parents are both talking with their doctor to get:
- Full Lipid Panel
- Showing the Aging.AI 3.0 - 19-parameter list, in hopes their Dr’s will add whatever additional tests to ensure all 19 parameters are measured.
We’ll see what their docs say.
2 Likes