I don’t try to maintain my fertility currently. I definitely want kids, just not right now. Matter of facts, I’m still virgin and don’t have a girlfriend so it is definitely not for soon. I could order rHCG (even an Ovitrelle pen is like 6500Ui for 25€ I think in France, so not costly), but what is mainly stopping me is the increase in aromatase enzymes creating more estradiol. Mine is already really high, wich could explain my BP (115 in systolic), and some water in my anckles. HMG is to expansive for a biweekly injection for months/years right now.
Meds like clomifene, tamoxifene etc. doesn’t work to imcrease LH/FSH while taking testosterone, especially at my dose, and their side effects are a no-go : eyes toxicity, blood clots, mood swing…
The idea is you use it 3 times a week, separated at least 1 day apart. You slowly titrate the dose up until you reach a point of overexcitement then start titrating downward. During this process you do mental exercises (also in the link I gave) and this drives up brain development.
I noticed by doing this for one month I gained a lot of mental benefits. I’m just starting this process up again.
Did you test your estradiol before and after starting tadalafil? Supposedly tadalafil slightly modulates estrogen metabolism.
Best to implement only if needed, and when you are trying to conceive.
Ok, so I guess all I’m saying is that it’s something to bear in mind. Some guys can conceive on TRT. Some guys can bounce back from years of TRT with no problems. Others need a lot of help to become fertile again. And others never regain fertility. You don’t know which group you’re in until the time comes. So if you definitely do want kids, at some point, you might want to think about preserving fertility, freezing sperm, or something to increase the chances in the future.
When I mentioned Clomid etc, I was meaning for when you came off, not to use them simultaneously with TRT, which would be dumb!
Totally agree. You see this in the trials of injections, gels, clomid, enclomiphene etc where the numbers on paper and the reported symptoms (qADAM etc) don’t necessarily line up.
For me personally there is a bit of a correlation with numbers and feel, but it’s hard to say which direction the correlation is. When everything is good, my normal total T is around 450-500, which isn’t a high boast-worthy number, but I feel good and function well. During a very stressful (work, study, life) period I measured my total T as around 150, and I felt horrible - but is that because I was stressed or because T was low. I’m not sure that boosting my T to 800 would have made me feel better, but maybe it would.
Anyway, with my stupid history of using prohomrones, oral steroids etc, I am just grateful that everything functions properly, my fertility was no problem, and mood etc is all good. I’ll periodically check, and if the numbers are dropping without cause, I’ll still keep an open mind to considering TRT.
I’ve had my testosterone higher than 1000 and I did feel great. Slight sleep interruption but it really felt good.
I’ve swapped from injection to cream. Lower testosterone overall I am presuming. Slightly higher DHT to test ratio. I feel a different mental quality in a good way on this.
I’m interested to increase the dosage but I will wait until my next blood test and see what the clinic thinks.
I’ve seen reports from men stating the same testosterone numbers on enclomiphene vs TRT injections feel totally different.
Same in the literature. Problem is, most studies are quite short, so the guys on Clomid get a big bump in T and free T and feel good. Longer term, that’s when the effects of blocking oestrogen happen, and when SHBG starts to creep up.
Personally, I would be curious to go for something like 12.5 mg Enclomiphene 3x per week, just as a “boost”, and see how the numbers and symptoms move.
Dr Fraser thanks that’s clomid still works on TRT and from my experience I believe so to. I take 25mg once weekly. Here you find it discussed (enclom. Vs Hcg);
An eleven months progress, from 58.5kg to 83kg currently, so +25kg, pretty sure at least 20kg of lean muscle gained.
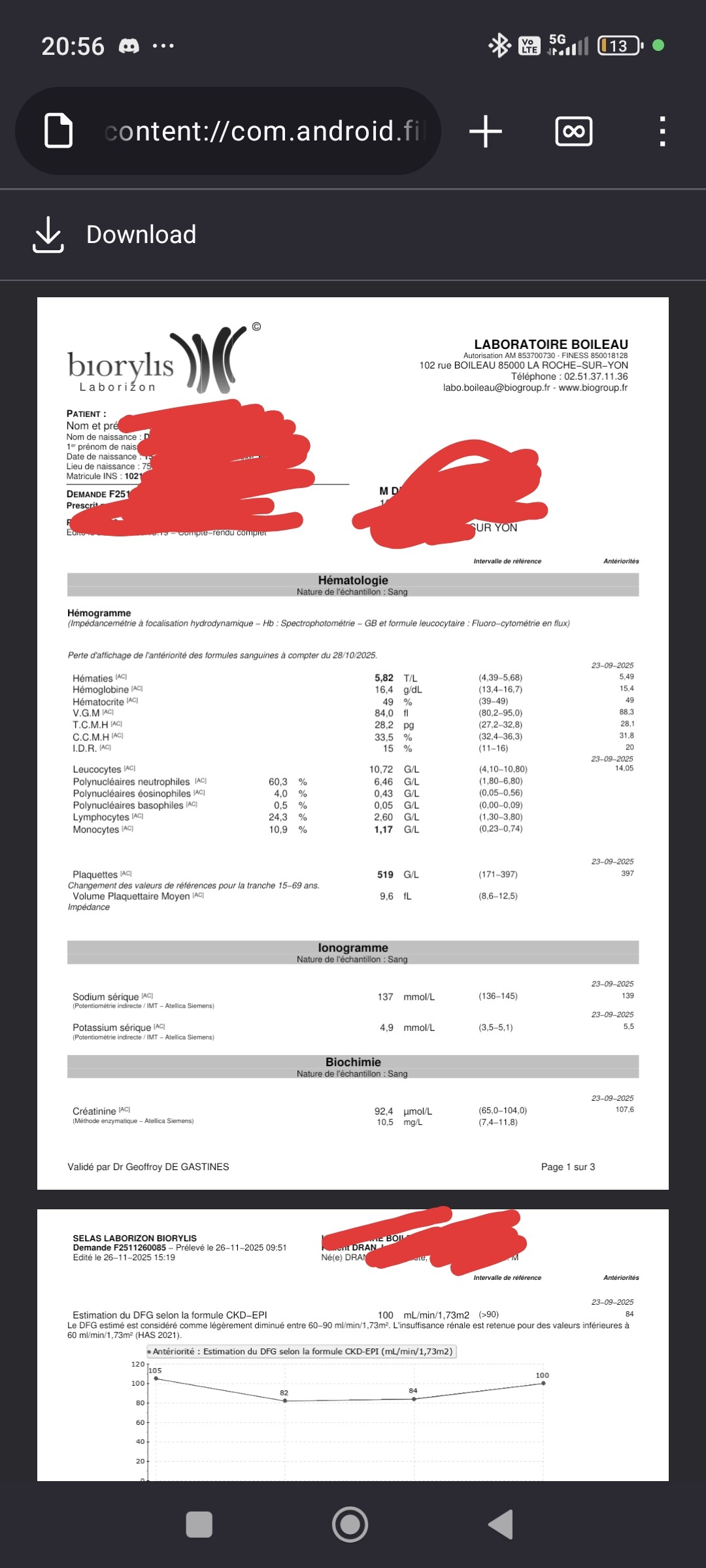
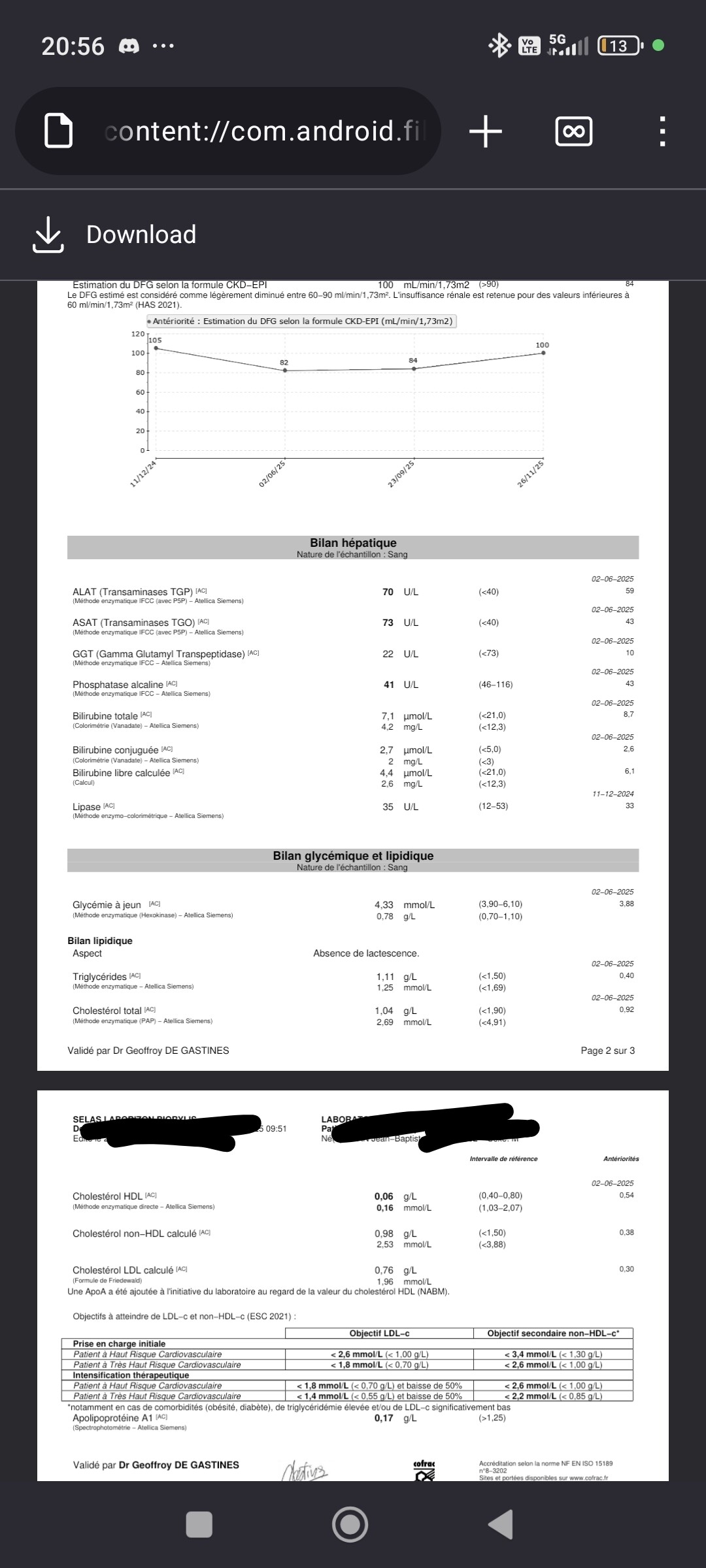
I’m not really putting all my energy in longevity but in bodybuilding, but still trying to mitigate risks, especially heart/liver and kidneys wise. What’s the point to live nit liking what you do? Concessions to make I guess sometimes.
Blood work isn’t t that bad for the cycle I’m currently doing and will be back to normal in my next cruise.
Well done on the 11 month transformation!
Can you post about your nutrition, supplements, and pictures of the back & legs?
Everything from the front looks very good (condition, muscle size etc). The upper chest area is the only thing I can see that could have more volume(overall roundness)
What exercises are you doing for chest?
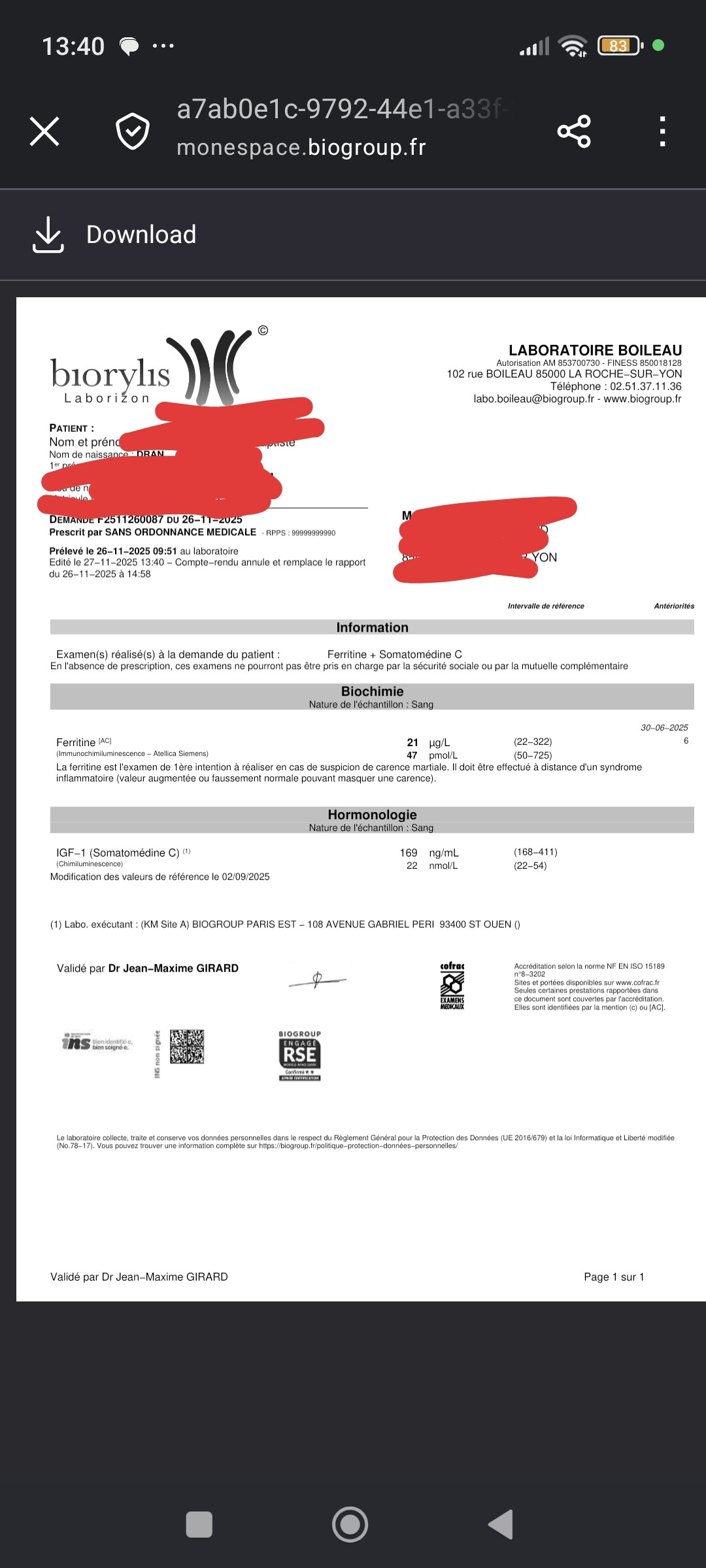
That’s odd your ferritin is still low, as it was also low before you started with the new cycle IIRC.
IGF-1 not very high either for what you are using.
Diet is composed of 5 meals a day with a small meal on top of that.
30g of animal protein per meal, usually 120g of fat a day from eggs and cheese, and carbs to go up to 5500kcal a day, usually pasta, rice, bread, fruit juice.
I agree for the upper chest, I prioritize shoulders so it does not help.
Right now I do on push workout
Flat barbell bench press, 2 sets
Incline dumbell bench press, 3 sets
Dumbell lateral raises, 4 sets
Triceps pushdown, EZ barbell, 2 sets
Less volume, max intensity.
I workout 5 to 6 time a week.
I’m at 6 UI of gh, igf1 is low but I was using raloxifene. I stopped it and in a few weeks I’m going to check again.
Some back picture (not my best body part)
Quads/Calves are okay, armstring and glutes are bad (IMO)
Total calories are 5500k or just carb cals? Cause that would be around 1350g carbs a day!
Various ideas:
Add use some type of fly exercise:
pec fly (pec deck) machines - bent arm machine and straight arm machine, cable machine flys, dumbell flys on various benches (incline, flat etc).
Good idea to check igf1 levels again. Hopefully it’s not from raloxifene. If not, I’m sure you know what to do.
Legs look pretty good. Outer quads could have more sweep. No hamstrings pics shown.
Front and back of calves look good.
Back looks good.
Maybe get tripod for phone to do pictures hands-free for all mandatory poses to get better idea overall of physique.
Keep up the good work!
I used to do flies for pump to feel my chest more, but I never really uses these exercise to build anything! I could try for sure.
I’m certain IGF1 is low because of the raloxifene, my baseline IGF1 is something like 220 so it should go up. I might not convert gh to igf1 that well, we will see!
I’m bad at posing and my front camera is bad on my phone. I look better in real life.
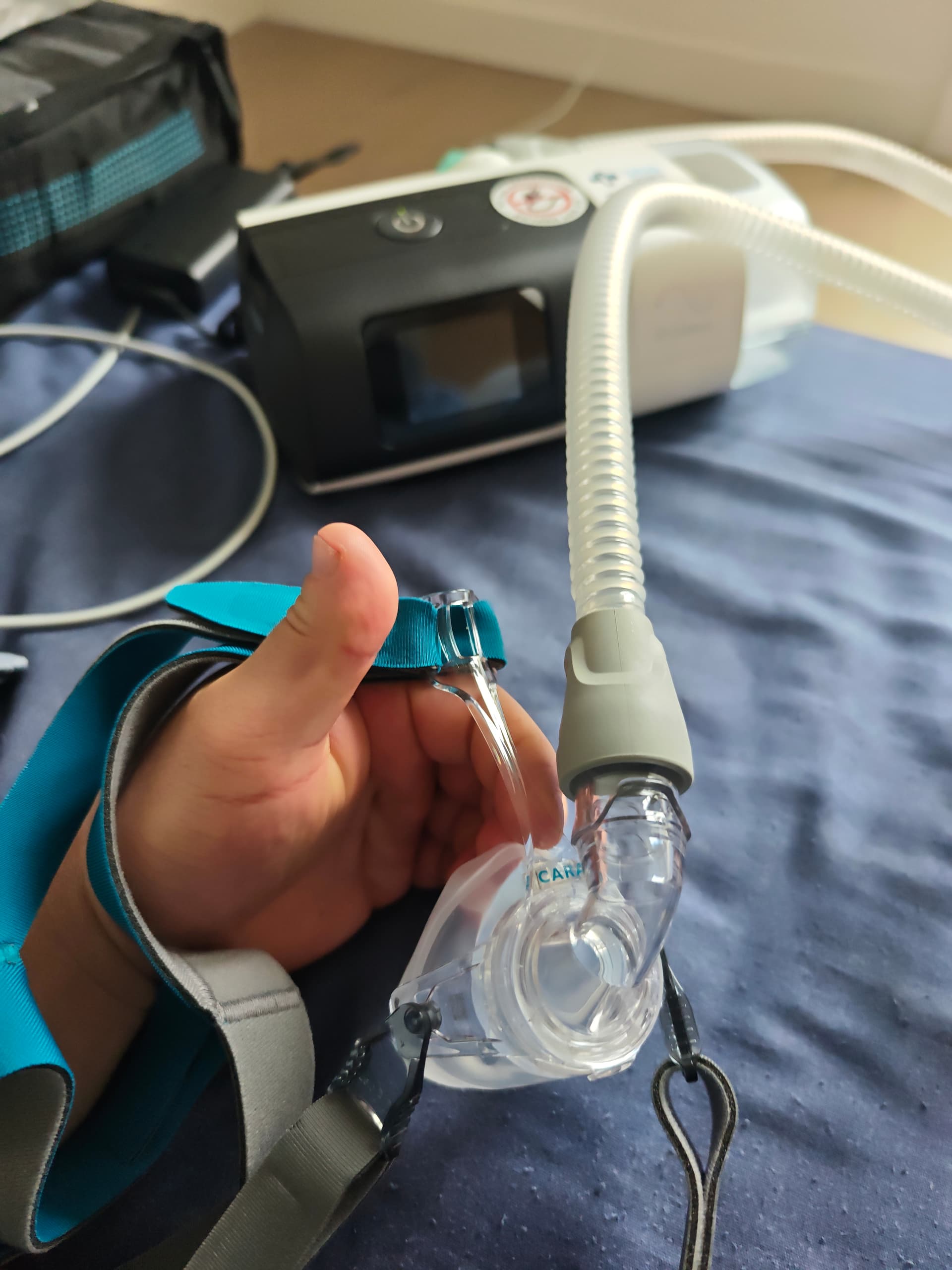
When you realise it’s way more expansive than you thougt…
For me it’s a month worth of salary every year.
I’m thinking of removing lactoferrin, very expansive and I already drink a few liter of raw milk every week.
Good luck with the CPAP, I also used one and it takes a long time to get used to it, but your numbers are not so good so I think it will be fantastic for you. One tip is to try Biotene to help with dry mouth as I found even using the humidifier it’s tough.
I also found later that I had a deviated septum, since having this fixed I have been able to stop CPAP. So something you could check out. Although I was only borderline with average 20/hr
Good luck