I ran across an article where Dr. Green described the improvements that rapamycin wrought. That’s what brought me here. Would like to induce something similar.
I hope to use this entry to track my results, quantitative and subjective.
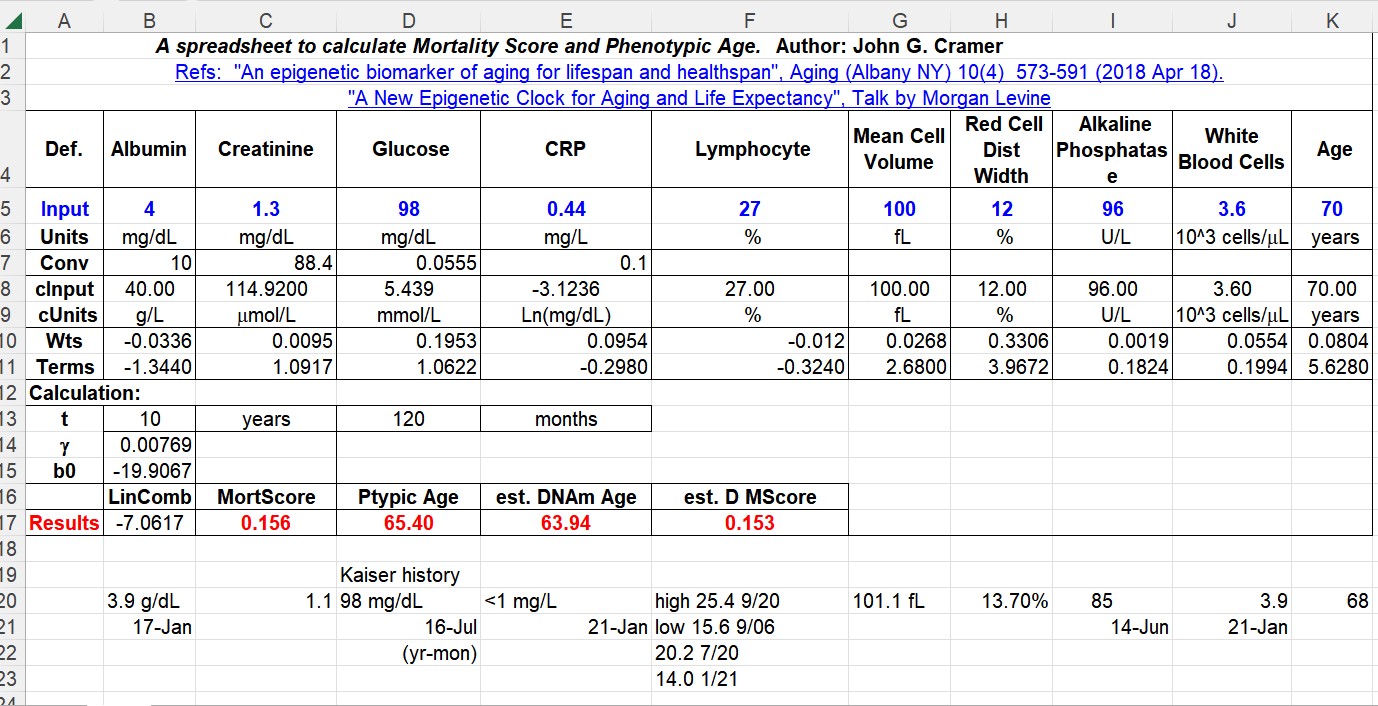
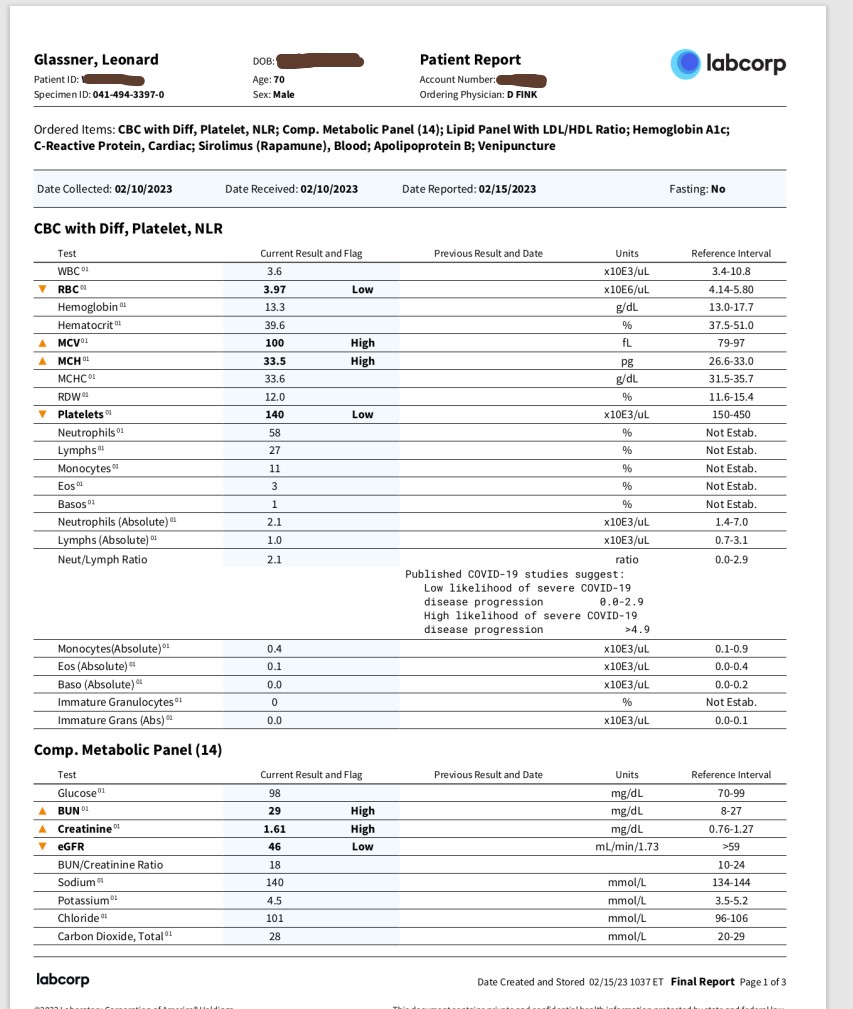
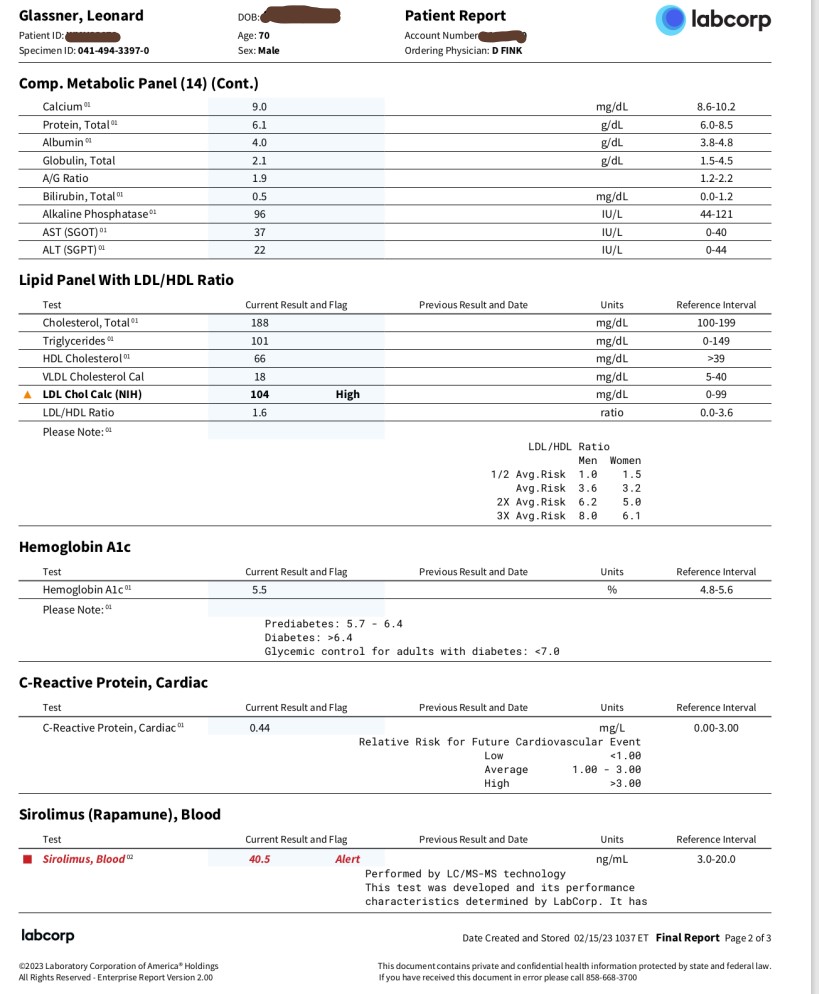
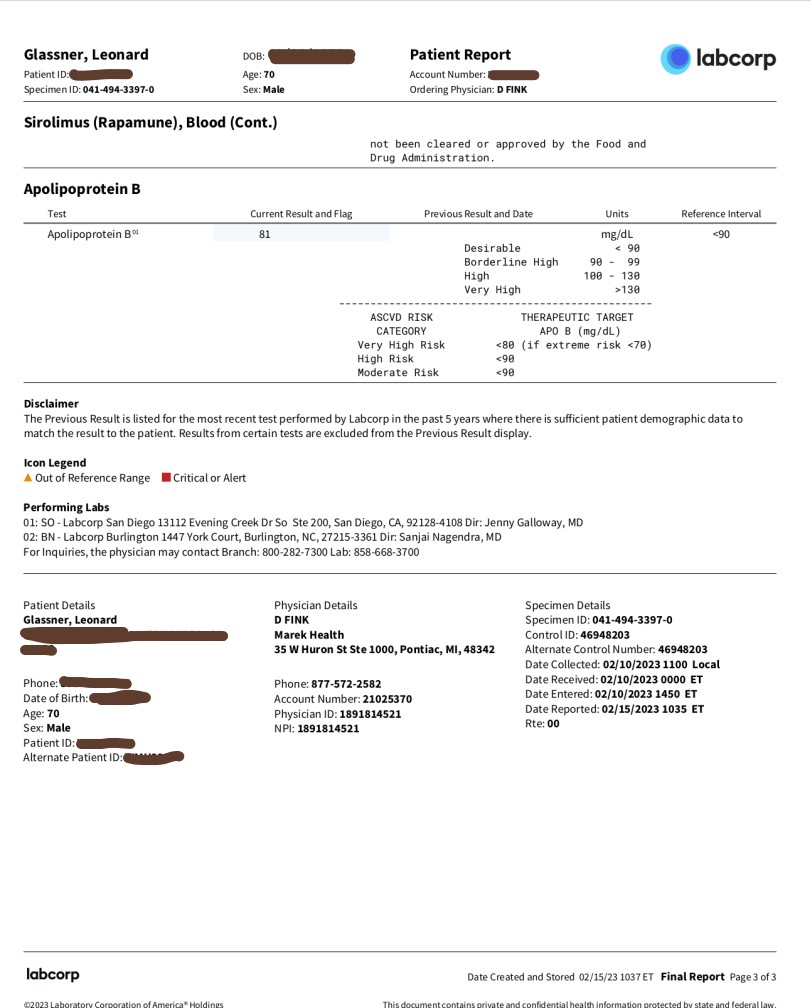
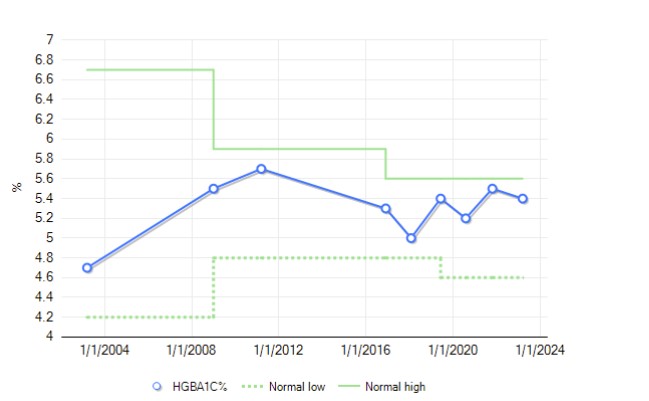
I will post some quantitative data as soon as I get test results from todays visit to Labcorp. I didn’t take a ‘before’ snapshot, but I have enough Kaiser history such that I hope I can construct something useful.
Profile
Caucasian male
age - 70y 5m
weight - 125 lbs BMI - 18
Fitness
Completed three 2000+ mile hikes at ages 59-61. Last long hike in 2019, six hundred miles.
Could still get over 5000 meter passes in Nepal, as of 2021.
Weekly exercise includes: 2-3 150 minute walks carrying a 27 pound backpack.
Once a week 5 hour hike which includes some 30%+ grades.
3-4 20 minute sessions of general stretching, sit-ups and push-ups. Very limited weight lifting.
Physical issues
Gelatinous transformation of bone marrow - as of 2003 biopsy.
Various out-of-bounds blood counts, noted since the bone marrow determination. Out of bounds, but stable.
-No symptoms associated with the above, accidentally uncovered when I injured a foot, and the usual blood tests were administered.
Osteoporosis
Poor dental health.
Osteoarthritis in hands and feet. Pain is minor, but let’s skip shaking hands.
DVTs in both legs. Taking Pradaxa.
Tinnitus
In 2016, I decided to try lifting weights after not doing so for four years. Induced neck and shoulder pains that can’t be eliminated. Issue involves muscles, not bones. I can still carry a backpack, but it’s a lot more painful.
Generalized aches and pains and tiredness that one usually associates with getting old.
…that’s enough.
Supplement regimen
Pradaxa, glucosamine/chondroitin, creatine, calcium, vit D, multivitamin, omeprazole (stopped for now) melatonin for sleep, verisol collagen, hyuralonic acid.
Rapamycin Objectives
Easily-noticed decrease or elimination of general aches and pains.
Overall feeling of greater energy.
Improvement in gum disease, noted by dentist without prompting.
Dosage plan
Started January 6, 2023 2mg Biocon Rapacan. Additional weekly doses - 3, 4, 5, 7, 10mg (today, Feb 10). Plan to continue at 10mg or greater. Not adding any boosters.
Benefits so far: None noted.
Side effects
A ridge on the inside of my cheek after the first dose. Receded after a few days.
Skin blemishes are ongoing, on scalp, face, elsewhere. Very annoying.
Some itching, seems to be reduced now, but still there.