Start your Skunk Works.
Do you know the makeup/delivery of the “InRapa” from Pfizer used in this study?
From the paper:
“6-month old Ts65Dn mice and euploid were administered intranasal rapamycin (InRapa; Rapamune, Pfizer, New York, NY, USA) and Vehicle (Veh; saline with 1% DMSO) for 12 weeks. The treatment was conducted 3 times per week, with a dose of 0.1 μg/μl of rapamycin solution or vehicle in 10 μl (1 μg/mouse)”
Anything intransal off the shelf I could piggy back? Or what carrier to formulate into for nasal spray into my brain?!
1 Like
To start consider dissolving pure{as pure as you can purchase] rapamycin in DMSO{as pure as you can purchase] dilute to 1%{the DMSO at 1%] You need to calculate what you want as your mg per ml.
200mg of rapamycin will dissolve in 1ml of DMSO
Tablet have many other compounds other than the rapamycin.
1 Like
I have currently a recent sourcing of raw powder I could use. So injecting some DMSO into the brain is benign? The mice didn’t have a say.
“Compared with liquid (solution or suspension) and gel formulations of drugs, powder particles are stable and not easily dissolved so they can remain in the nasal mucosa for a long time.”
So, I will see if my rapamycin supplier can sell me pure rapamycin powder.
Get a straw and it will be like snorting cocaine. I don’t want anyone watching me while I snort rapamycin lest they get the wrong idea.
Trying to cross the blood-brain barrier is the main reason for my high doses of pulsed rapamycin.
This would appear to be the easiest way to start as rapamycin is very poorly soluble in water.
2 Likes
I posted a copy of a medical book on DMSO on another thread, book titled;
“Dimethyl Sulfoxide (DMSO) in Trauma and Disease” by Stanley W. Jacob
Go to
See posting 16, the link to the upload book
1 Like
This is a great question… lets look and see if we can find anything already on the market:
Here is one of the vendors of this intranasal technology:
https://sipnose.com/technology/
Here is a recent paper on the different intranasal systems:
CLINICAL TOXICOLOGY
“A short-term study (14 days) and a long-term study (90 days) were undertaken by
Brobyn who reported his findings on 213 healthy human volunteers. These volunteers were periodically examined by specialists after being administered 1 g/kg/day 80% DMSO daily. This dose was considered 3–30 times higher than the typical DMSO dose used or recommended. The specific clinical examinations included complete physical examinations with laboratory examinations of blood and urine, ophthalmologic, dermatologic, cardiologic, neurologic, pulmonary function, and bone marrow studies. The results of this study concluded that no significant adverse effects from either the short-term or long-term administration of DMSO were observed after a very
extensive toxicology study was conducted. DMSO is a relatively safe drug. Side effects to DMSO are common, but these are usually minor and are related to the concentration of DMSO used and the route of administration”
Toxicity (wiki)
DMSO is a non-toxic solvent with a [median lethal dose] higher than ethanol (DMSO: LD50, oral, rat, 14,500 mg/kg; LD50, oral, rat, 7,060 mg/kg"
Is there some consensus it’s biologically safe to ingest internally,
1 Like
I wonder if Temsirolimus would work as a nasal additive to some existing nasal product? Its going to go off patent soon I think…
Mechanism of action
“Temsirolimus is a specific inhibitor of [mTOR] and interferes with the synthesis of proteins that regulate proliferation, growth, and survival of tumor cells. Though temsirolimus shows activity on its own, it is also known to be converted to sirolimus (rapamycin), therefore, its activity may be more attributed to its metabolite rather than the prodrug (despite claims to the contrary by the manufacturer). Treatment with temsirolimus leads to cell cycle arrest in the [G1 phase, and also inhibits tumor angiogenesis by reducing synthesis of VEGF”
1 Like
It may be safe, but trust me, you don’t want to squirt it up your nose in the undiluted form.
FWIW
I have used it topical, orally and by IV on more than one occasion.
Review;
“Dimethyl Sulfoxide (DMSO) in Trauma and Disease” by Stanley W. Jacob
1 Like
@rapadmin Thanks for the reference.
@Joseph Thank you for the DSMO study and being an oral/IV DSMO guinea pig.
“Intranasal delivery means rapid, noninvasive access to the brain enabling numerous
novel therapies. However, this is not a panacea, and careful optimization will be needed
for any of these new treatments to reach patients. A major factor will be the formulations
and devices described in this article.”
ok expected that
Some “engineering” parameters to consider.
“Hydrophobic and charged hydrophilic molecules have been shown to diffuse poorly through mucus, whereas uncharged hydrophilic molecules are able to diffuse rapidly through the mesh of mucins nearly the speed of water for smaller molecules. Drugs larger than 500 Da in size will be especially prone to poor mucus diffusion and becoming stuck, though most drugs will be smaller than 500 Da in size, thus it is not an important issue. Optimizing a formulation to maximize crossing into the lamina propria will be crucial for any therapy. This size limit is not entirely inhibiting though, as molecules as large as wheat germ agglutinin–horseradish peroxidase (80 kDa) and even whole stem cells have been transported to some degree. Nonpolar compounds are thought to be transported poorly to the CNS intranasally, though there is a growly body of evidence that the proper microemulsion formulation can greatly increase the intranasal brain area under curve (AUC) compared to IV administration of the compound. Indeed, there is evidence that with some drugs increasing the hydrophobicity can increase delivery to the CNS. It is known that hydrophobic compounds cross biological membranes such as the nasal epithelia, blood vessels, or BBB well. This shows that not only are hydrophobic drugs capable of being administered intranasally with the correct formulation, but this may be an advantage. Often, researchers are administering doses as low as 25 µL but usually closer to 200 µL in size in these experiments; a size selected because this is the maximum volume of the nasal cavity in the model rodents. In humans, the nasal cavity is 6–7 mL in volume, which is impractical at best. Furthermore, 50% of the rodent nasal cavity is covered in olfactory epithelia, compared to <5% in humans. This limitation in area will make delivery to the CNS less efficient and adds emphasis on making sure administered drugs reach the correct region of the nasal cavity. Intranasal administration devices are another compelling strategy that will find a role in the clinical use of intranasal drugs. Recall that the olfactory region is <10% of the entire nasal cavity and located on the superior aspect as well as the rapid mucus clearance in the motile respiratory regions. Traditional spray pumps tend to only reach the anterior and lateral aspects of the nasal cavity, with <3% of the dose reaching the olfactory region.”
Rapamycin is both hydrophobic and a HUGE molecule…26,000 Da. But clearly in the study, no problem getting into the brain. Intranasal bypasses the entire gastric pathway, degradation loss, the massive system dose (and unwanted peripheral side effects) needed for therapeutic brain Rapamycin levels.
In the study, they used “InRapa” by Pfizer. I could not find “InRapa”, is this the same as their oral solution?
https://www.pfizermedicalinformation.com/en-us/rapamune/principal-display
“The treatment was conducted 3 times per week, with a dose of 0.1 μg/μl of rapamycin solution or vehicle in 10 μl (1 μg/mouse) for 90 days total”. 6 mice were treated by single intranasal delivery of rapamycin, with the dose of 1 μg/mouse (0.05 mg/Kg/mouse)"
Based on the 1 ug/ul reference, this is the same as 1mg/ml oral Rapamycin solution, so I am assuming same.
That’s a super lower dose intransal to get large brain Rapamycin levels! Consider in some of the mice longevity studies, oral dose 2.25 mg/kg to 8 mg/kg. "To note, InRapa dose is about 50-times lower than i.p injection dose"
“Collectively, our data demonstrate that rapamycin delivered by intranasal route reached a therapeutic brain concentration comparable to that obtained by i.p. injection but with an extremely lower distribution at plasma level. Therefore, these results, coupled with the analysis by WB of mTOR inhibition in liver and heart tissue, which showed no changes between Ts65Dn rapamycin and vehicle treated groups”
“Overall, our data show that intranasal delivery of the mTOR inhibitor rapamycin was able to target and modulate mTOR kinase activity in the hippocampus. Our analysis of mTORC2 activity, indexed by phosphorylation of mTOR at Ser2481, show no alteration between Eu and Ts65Dn mice either with or without InRapa administration (supporting the low sensitivity of mTORC2 to rapamycin treatment”
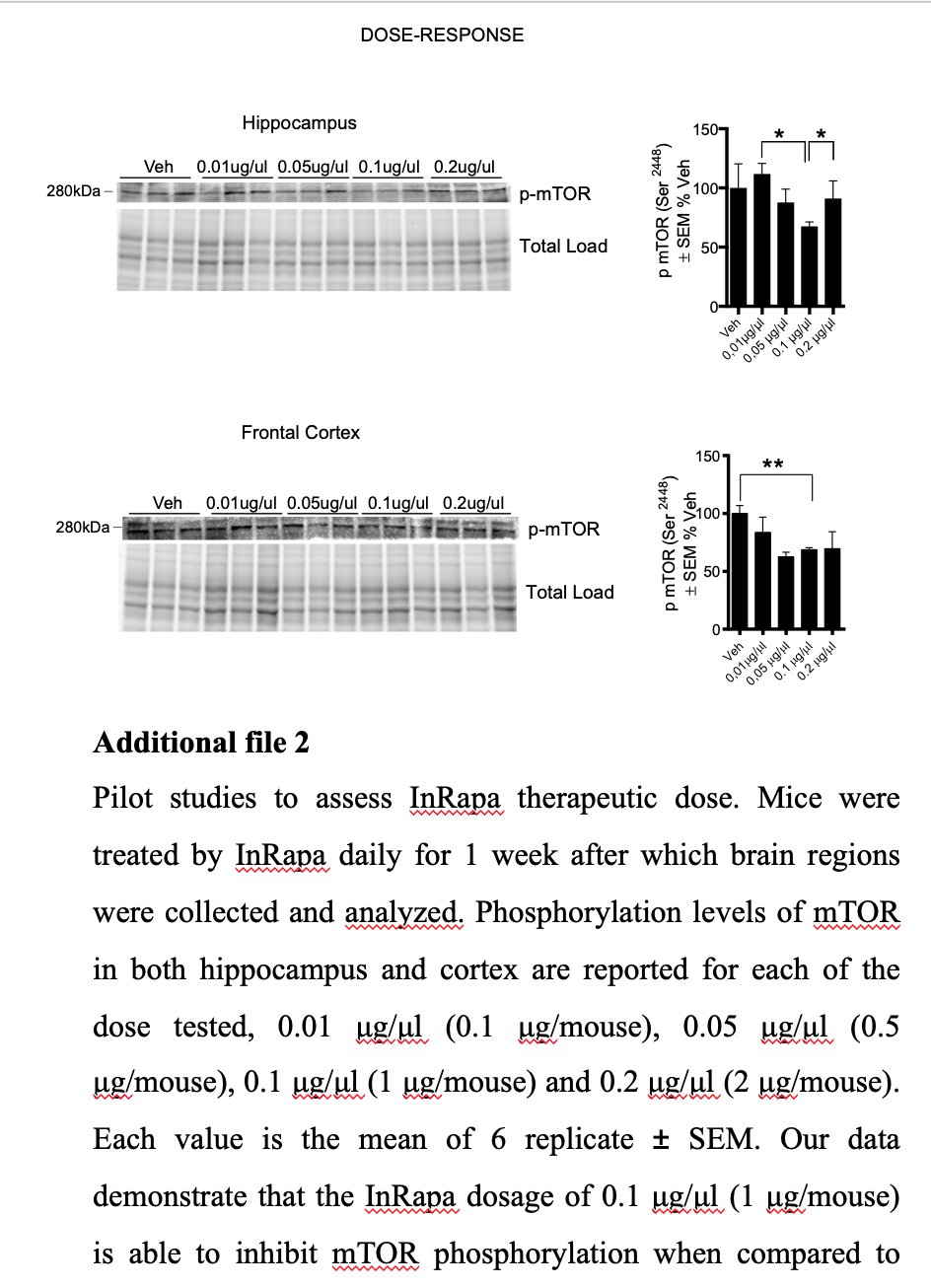
Notice the 0.2 ug/uLdid not reduce pMTOR more than the 0.1 ug/uL.
Converting 0.05 mg/kg mouse to HED = 0.29mg @ 70 kg human (if oral or ip is equivalent to intranasal)
I think I won’t reinvent the wheel, make up a DSMO/water/Rapamycin powder solution and find a good intranasal device to deliver where it needs to go.
Now the black hole…qty, dose, and what the heck am I measuring as response?
Maybe will circle back and review some of those online tools…do some baselining, then re-test.
My solution/mix
DMSO
Rapamycin
Saline
Final solution
1% DMSO,
Rapamycin at 1mg per ml,
each spray delivers 1mg of the solution = to 1mg of rapamycin
1mg in each nostril
@joseph You posted this elsewhere
"Dissolve the rapamycin in the DMSO first, then reduce to 50 to 70% {this is the best absorption % through the skin] Higher % of DMSO on skin is not absorbed well and on most people will burn/irritate are. Rapamycin dissolves in DMSO at 200g per ml. The solubility of rapamycin in 50/50 DMSO/water, as used in osmotic pumps, is about 0.5 mg/mL at ambient temperature.”
Re saline, off the shelf saline? I could buy some bulk saline, and then a fancy smaller saline spray to hijack the sprayer, or look for a more highly engineered sprayer.
Dilute the rapamycin/DSMO bulk mix down to 1% DSMO using saline to get 1mg Rapamycin/ml solution?
I think you asked me where I got the powder?
1 Like
MAC:
Re: The Rapamycin Store:
They are now pushing transdermal cream. Their prices seem very reasonable.
Paying by Bitcoin is a bit sketchy right now. I do have a Coinbase account.
Have you ordered anything recently?
Re: nasal spray:
Do you really think the saline is necessary?
Does it actually add anything over distilled water?
Not recently but I think they are legit.
Don’t know, for hermetic reasons since I might be making 1-2 months worth, keep it bacterial safe? I could make my own saline with distilled. Probably not materially important for this endeavour.
Mac
I am sorry, I was just lazy and thought maybe there was something you knew so that I wouldn’t have to look it up.
Apparently, a saline solution has no anti-bacterial properties. DMSO in concentrations over 15% is anti-microbial. Additionally, distilled water has less surface tension than salt water. So, in brief, I won’t be using anything but DMSO, distilled water, and rapamycin, unless someone can point out the benefit of using a saline solution.
“A study has been made of the antimicrobial activity of dimethyl sulfoxide (DMSO) against three organisms, Escherichia coli, Pseudomonas aeruginosa, and Bacillus megaterium. Growth was inhibited by increasing DMSO levels and was virtually eliminated for each of the species at approximately 15% DMSO.”
Antimicrobial Activity of Dimethyl Sulfoxide Against Escherichia coli, Pseudomonas aeruginosa, and Bacillus megaterium - ScienceDirect.
1 Like