"Dissolve the rapamycin in the DMSO first, then reduce to 50 to 70% {this is the best absorption % through the skin] Higher % of DMSO on skin is not absorbed well and on most people will burn/irritate are. Rapamycin dissolves in DMSO at 200g per ml. The solubility of rapamycin in 50/50 DMSO/water, as used in osmotic pumps, is about 0.5 mg/mL at ambient temperature.”
Re saline, off the shelf saline? I could buy some bulk saline, and then a fancy smaller saline spray to hijack the sprayer, or look for a more highly engineered sprayer.
Dilute the rapamycin/DSMO bulk mix down to 1% DSMO using saline to get 1mg Rapamycin/ml solution?
MAC:
Re: The Rapamycin Store:
They are now pushing transdermal cream. Their prices seem very reasonable.
Paying by Bitcoin is a bit sketchy right now. I do have a Coinbase account.
Have you ordered anything recently?
Re: nasal spray:
Do you really think the saline is necessary?
Does it actually add anything over distilled water?
Don’t know, for hermetic reasons since I might be making 1-2 months worth, keep it bacterial safe? I could make my own saline with distilled. Probably not materially important for this endeavour.
Mac
I am sorry, I was just lazy and thought maybe there was something you knew so that I wouldn’t have to look it up.
Apparently, a saline solution has no anti-bacterial properties. DMSO in concentrations over 15% is anti-microbial. Additionally, distilled water has less surface tension than salt water. So, in brief, I won’t be using anything but DMSO, distilled water, and rapamycin, unless someone can point out the benefit of using a saline solution.
The study referenced saline in the vehicle, so just telegraphed. Thanks for this information.
Wow, DSMO is regulated in Canada, need a script? Ordered through my Amazon US account, ships to Canada, back door. Will go with distilled water as well.
@desertshores are you good with putting some of this DSMO into the brain??
I recommend you download the PDF copy of the book I posted, and review.
Dimethyl Sulfoxide (DMSO) in Trauma and Disease” by Stanley W. Jacob
See link in post above.
This is a medical book not a consumer book.
Medical metered spray bottles are commercial available, supplies from a compounding pharmacy.
There are forum members here who are pharmacist, mybe could add to this thread.
I would mix as follows
Assayed grade rapamycin to Pharmaclocigal grad DMSO till totally dissolved.
As a reference 200mg of rapamycin will dissolve in 1ml of DMSO
Then dilute to 1% using standard saline 0.9%
You have to calculate the dose of rapamycin you want per ml deliver sprayer.
In my view I would use 1mg per ml of raperymicin in a 1% DMSO from a nasal sprayer that would deliver 1ml per squeeze.
You get 1mg of rapamycin per ml from each squeeze, 1 squeeze up each nostril would be 2mg of rapamycin.
The laboratory supply company mentioned by RapAdim several times sells Rapamycin, >99% with Certificate of Analysis. They do not sell to individual as RapAdim has stated.
I read briefly through the book mostly looking for toxicology/safety.
Will investigate spray/misters some more.
How much volume of liquid do you think should be sprayed per pump into a nostril? Want to cover the key uptake cells but not have any spillover/dripping?
Or do full headstand or tilt head back 90 degrees after application to allow for diffusion!
Yes, squirting DMSO up your nose would certainly be scary at this time and I wouldn’t recommend it.
Most of you are not old enough to remember the DMSO craze of the hippy era. Everybody was using it for arthritic pain etc. Then the government temporarily banned it and all kinds of conspiracy theories evolved.
However, I have found the following mentions:
“It also has a calming effect on the central nervous system and it reaches all areas of the body, when absorbed through the skin, including the brain”
So, I don’t think you have to squirt it up your nose to get into your brain.
I have changed my mind and don’t personally plan to do it.
“If you have dirt or anything else on your hands and /or skin, DMSO will take it down to your deep tissue, as far as to the seventh layer into the dermis”
“The clinical use of pharmaceutical-grade DMSO as a penetration enhancer is supported by the robust data that have accumulated over the past 3 decades demonstrating the favorable safety and tolerability profile. Dimethyl sulfoxide is a safe and effective mechanism for facilitating the transdermal delivery of both hydrophilic and lipophilic medications to provide localized drug delivery.”
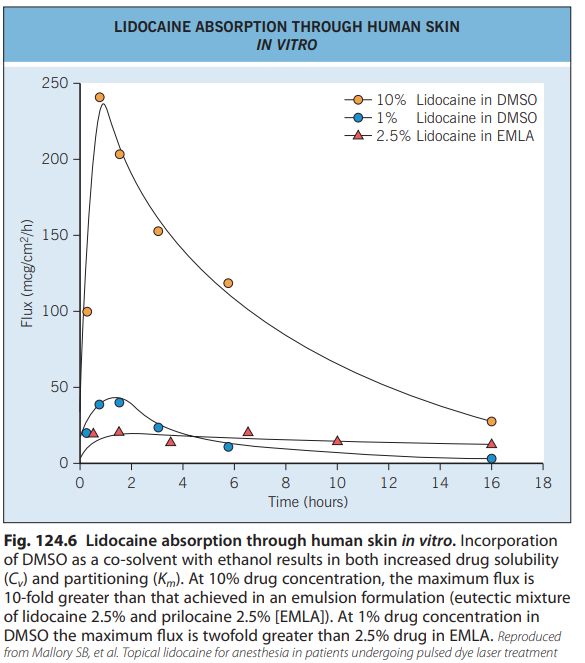
A number of other compounds have been identified as enhancers.
Dimethylsulfoxide (DMSO), the archetypical enhancer, exemplifies the
effects that can be achieved ( Fig. 124.6 ). As with ethanol and propylene
glycol, both C v and K m are affected. Because DMSO is a superb solvent,
higher drug concentrations can be achieved than with other solvents,
but it also expands the stratum corneum barrier, permitting increased
drug uptake and possibly an increased rate of diffusion ( D) through the
barrier. However, the use of powerful enhancers such as DMSO is
constrained by excessive skin irritation or toxicity 41.
“Soluble in DMSO at 200 mg/mL; soluble in ethanol at 50 mg/mL; very poorly soluble in water; maximum solubility in plain water is estimated to be about 5-20 µM; buffers, serum, or other additives may increase or decrease the aqueous solubility.”
Ok, looks like it’s either DSMO/water or Transcutol (Diethylene glycol monoethyl ether). Both appear to have good toxicology re system absorption, and Transcutol is a food additive.
For Transcutol, water is a very poor cosolvent with Rapamycin, so would be used at 100%.
@joseph votes DSMO 1%/water and @desertshores A no for DSMO, but what about 1% DSMO in water?
In the mice study, nasal dose is 50X lower than ip injection dose. So assuming 2mg nasal full absorption, that could be a massive oral equivalency dose.
I would have to do some more dosing equivalency (look at ip injection vs oral mice) and calibrate the mister, titrate from low and work up.
At this point, I think I will wait for further developments. I have no relatives, living or dead, that I know of, that suffer or have suffered from dementia or Alzheimer’s, so putting rapamycin up my nose is not a high priority at this time.
Unfortunately, DMSO is a two-edged sword.
I consider it relatively safe as it is being used as a carrier for some medications.
And, I like it because, unlike most other solvents, it will carry rapamycin beyond the first layers of skin.
Having said that, it may also carry contaminants that are on your skin or in the medication you are using.
I have not been able to obtain pure rapamycin powder at this time so I don’t know what additives or contaminants are in the pills that I am crushing to get the powder. Zydus and Rapacon both contain titanium dioxide and some other fillers.
I have used a mixture of 50/50 DMSO and water mixed with 20mg. of rapamycin on my skin. I am going to discontinue doing this for the time being.
This has been debated before so I don’t want to debate it again, but I believe high doses of rapamycin, 10 - 20 mg, with grapefruit juice pass the blood-brain barrier.
So, I will continue with this as an alternative to spraying rapamycin up my nose.
Well even if I don’t pursue the intranasal experiment, I am ready for the next corona virus pandemic.
Application of nasal spray containing dimethyl sulfoxide (DMSO) and ethanol during the COVID-19 pandemic may protect healthcare workers: A randomized controlled trials
"The present study aims to evaluate effects of a solution of 20% ethanol, 3% DMSO, and 0.1% menthol as a nasal spray in preventing from SARS-CoV-2 infection. Individuals assigned to the intervention group were advised to spray a puff of DMSO spray into each nostril every 8 hours for four weeks in addition to routine daily care. It was recommended for the control group to continue daily routine care. Two hundred and thirty-two participants were randomly assigned to intervention and control groups to receive DMSO/ethanol or routine care, respectively. The subjects were followed for 4 weeks to determine the incidence of COVID-19 infection in each group based on the RT-qPCR test. Finally, absolute risk difference and relative risk were calculated to evaluate the effect of DMSO in prevent COVID-19.
Results: The results showed that the incidence of COVID-19 in the control group and intervention group were 0.07 and 0.008, respectively. The relative risk (RR) was 0.12 (0.9-0.02) according to the incidence rate in the two groups.
There are all sorts of intranasal spray formulations containing DSMO for retail sale.
Thanks for coming up with articles for our entertainment.
“Clear Mind Nasal Mist”
I must confess I am very skeptical of a “DOCTOR OF NATUROPATHIC MEDICINE” but, it is further evidence that squirting a little DMSO up your nose might not be harmful.
Still, another taking a few cents worth of common ingredients and figuring out how to charge a lot.
Of course, the scary part of his formula is the “essential oils”. Do I really want them carried into my brain by DMSO?
I didn’t include these for any interest other than doing further due diligence on the safety of low % DSMO as enabler for Rapamycin entry through the nasal passageway. The more I dig, the more I see on clinical and retail use, the less concerned I am about DSMO chemical and limited exposure. Moving on to the nitty gritty of concentration and dosing.
@MAC Thanks for pulling all this info together here… I will be doing a deep dive into it next week to see what might be a reasonable strategy for me would be. I think the intranasal dosing strategy seems like a good one.
One of my key concerns is that it would really seem that we would want to start with the raw powder (not crushed tablets, just due to all the filler that is the vast majority of the tablets), and as you know, I’m very concerned about the purity and contaminants in any rapamycin powder that is purchased from China (and the cost and difficulty of testing for the purity and the various potential contaminants - the common ones seen like nitrosamines, but the bigger concern for me is the potential for uncommon contaminants that we don’t know to look for because we don’t know the supply chain / manufacturing process so its hard to know of any potential cross contamination or impurities (e.g. impure water) that might be interjected into the process. Obviously you can search via analytical chemistry for the known contaminants, but its harder for the unknown or unexpected contaminants…
I think so too…high potency directed delivery to the brain without resorting to immunosuppression/metabolic dysregulation of periphery with high oral doses? I would still do periphery dosing (w blood panels, sirolimus monitoring), but perhaps more conservative.
Agreed. I have 4 grams of powder, a lucky benefit for this exploration.
Yes always. The mass spec/HPLC didn’t indicate any obvious negative signal, but risk to everything. I might be more at risk eating a grilled beyond meat burger or driving in the polluted toxic air of a big city.
“Nitrosamines can be found in a wide variety of foods, such as beer, salted fish, non-fat dry milk, cured meats like bacon and hotdogs, and cheese, agricultural chemicals like fertilizers, tobacco products, detergents, rust inhibitors, cutting fluids, rubber additives, solvents, drugs, plastics, tanned leather products, textiles, and cosmetic products.”
“PM from central London over two periods in winter and summer. The average total nitrosamine concentration was 5.2 ng m−3, substantially exceeding a current public recommendation of 0.3 ng m−3 on a daily basis. The lifetime cancer risk from nitrosamines in urban PM exceeded the U.S. Environmental Protection Agency guideline of 1 excess cancer case per 1 million population exposed after 1 h of exposure to observed concentrations per day over the duration of an adult lifetime. A clear relationship between ambient nitrosamines and total PM2.5 was observed with 1.9 ng m−3 ± 2.6 ng m−3 (total nitrosamine) per 10 μg m−3 PM2.5.”
We all have our risk/reward equations. I’m liking this new paradigm opportunity to unlock a better pharmacological/longevity benefit of rapamycin.
Now if these guys take VISA? Craniotomy is a no for me.
While we’re thinking outside the box, what about ip injection, far superior to oral? LOL
Comparison of rapamycin schedules in mice on high-fat diet
"Here we demonstrated that i.p. injections of rapamycin prevented weight gain on high fat diet, whereas rapamycin by gavash (also given 3 times per 2 weeks) did not. Orally administrated (gavash) rapamycin has poor bioavailability. The i.p. route of its administration ensures high peak of systemic levels of rapamycin. We can conclude that acute high levels of rapamycin may be necessary to prevent obesity."
" It may seem paradoxical that intermittent administration (by i.p.) is more effective than everyday administration (by oral gavash). One plausible explanation is that at high peak levels, rapamycin may affect cell types that are not sensitive to low concentrations of rapamycin. In fact, the effective concentrations of rapamycin vary broadly in cell lines in culture" (most especially the brain)