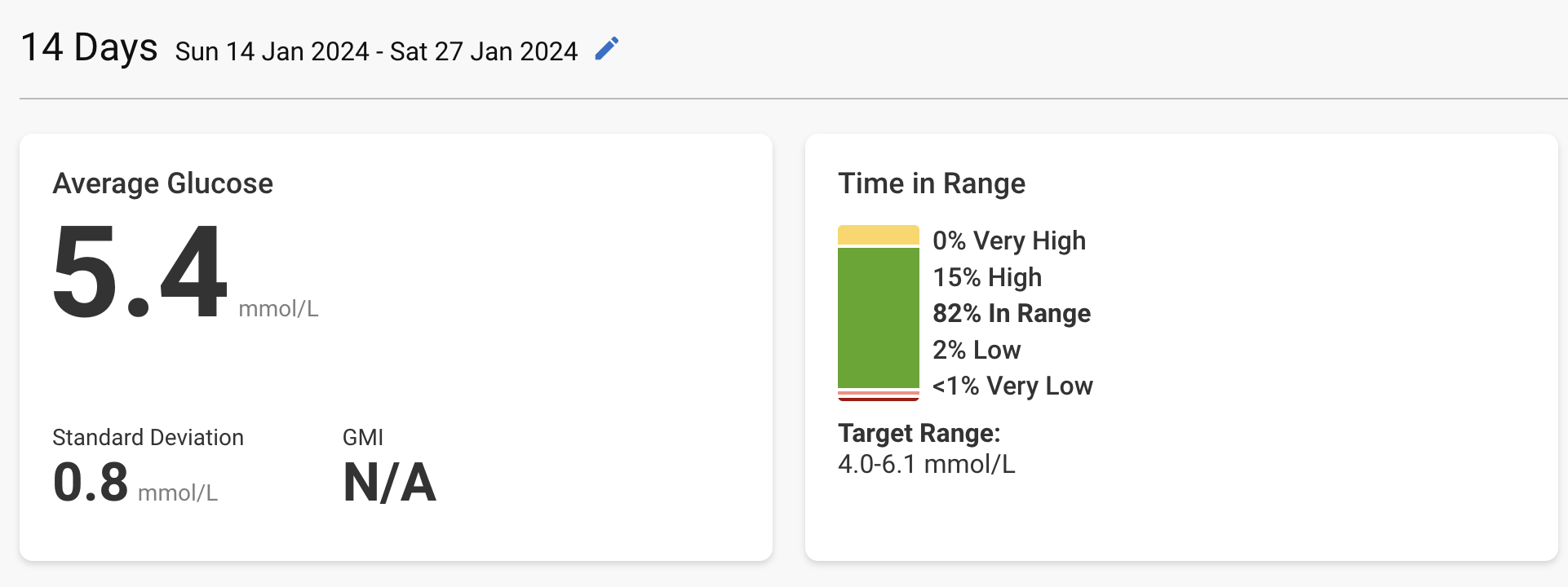
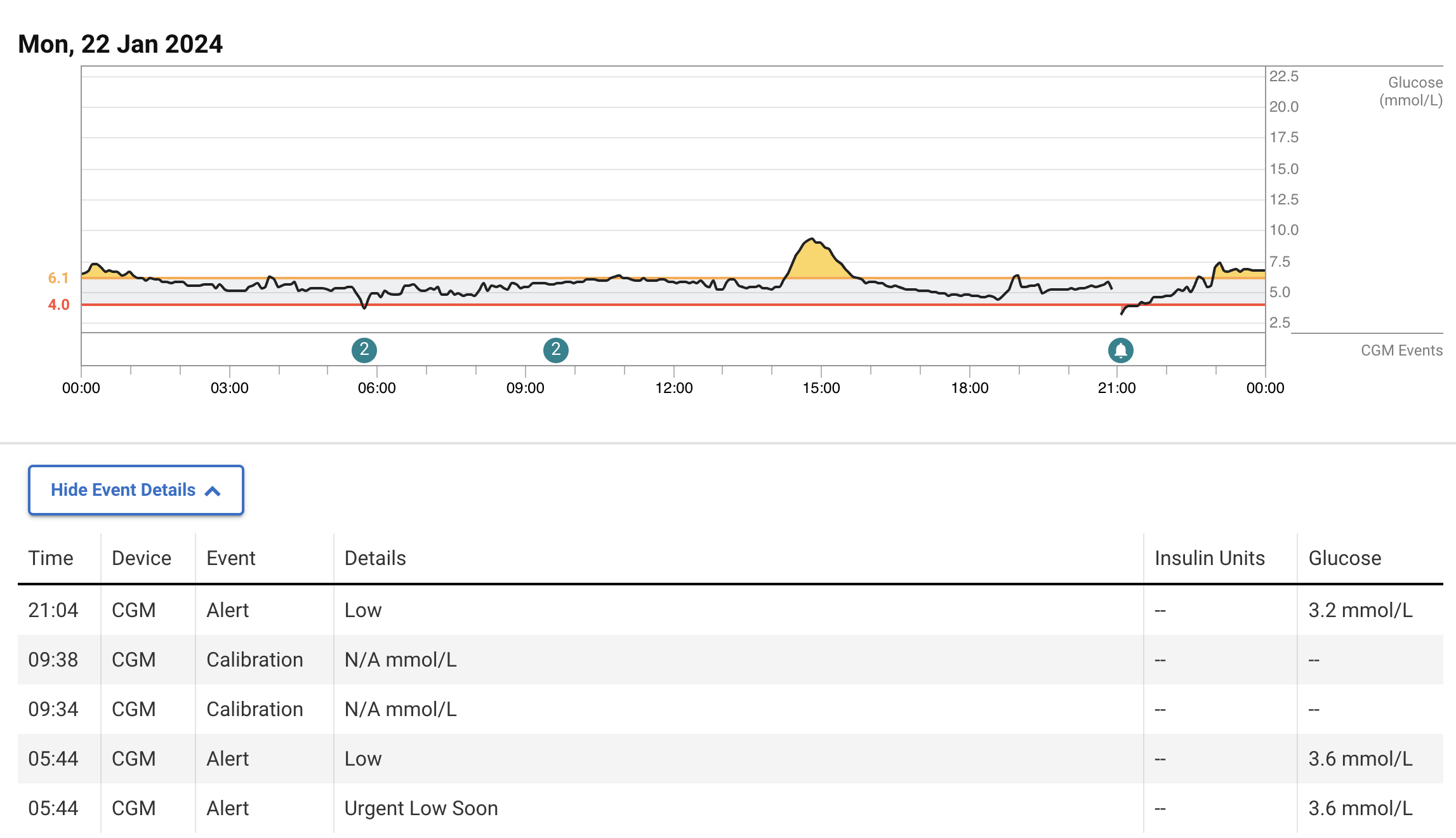
The average given by the CGM (5.4 mmol/L = 97 mg/dL) is equivalent to Hb A1c of 5.0% (source). My latest Hb A1c from early March was 5.1%. So, CGM and blood test are in agreement.
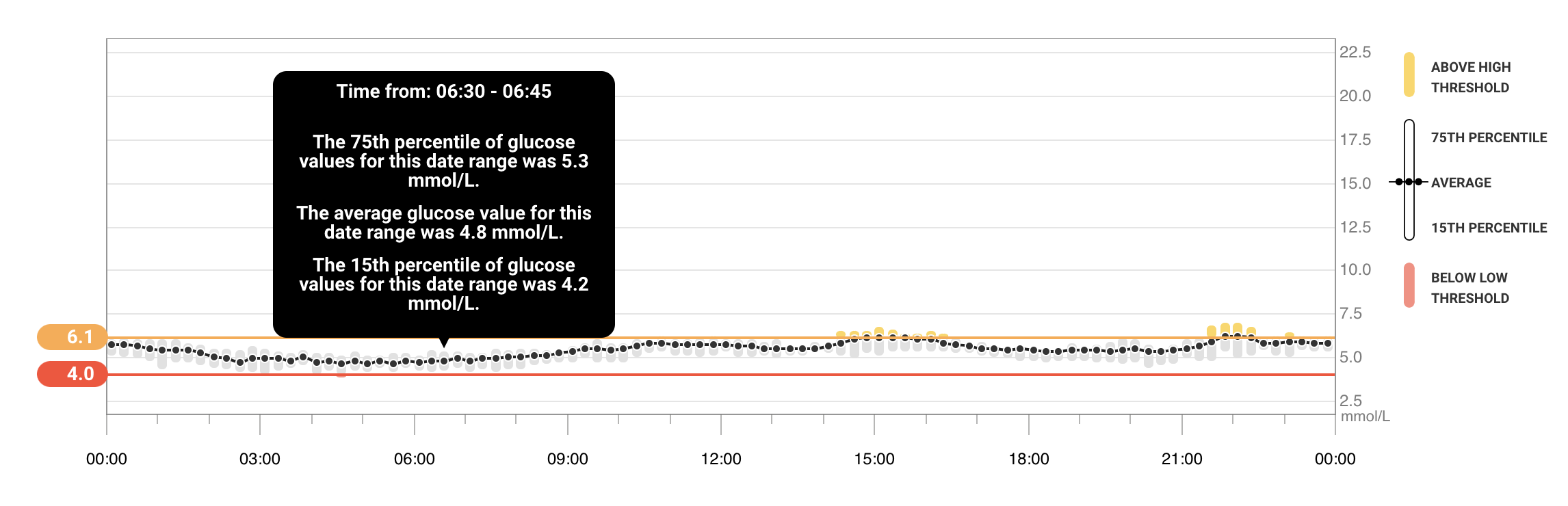
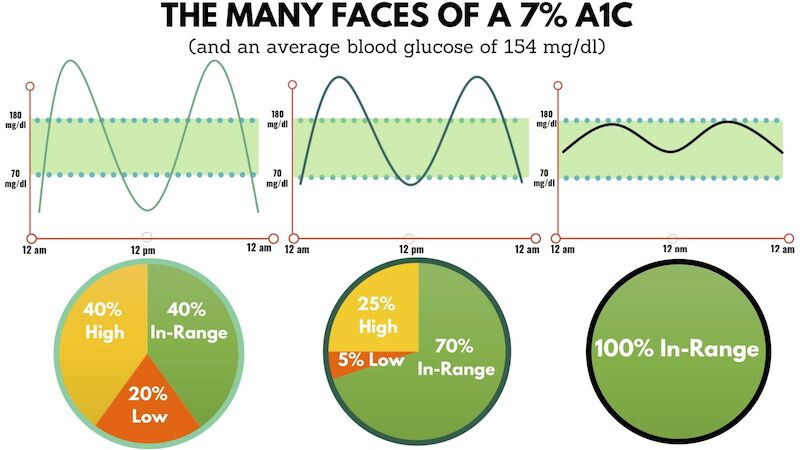
The peak is OK. But I’m “yo-yo-ing” a lot, and when this happens, I feel terrible. That’s why Hb A1c isn’t a great KPI; the same average can correspond to different patterns:
Using the last 7 days of my latest CGM data, with dapagliflozin 10 mg daily + acarbose 50 mg just before “big” meals + “good carb” diet (no white rice but whole grain quinoa OK for instance):
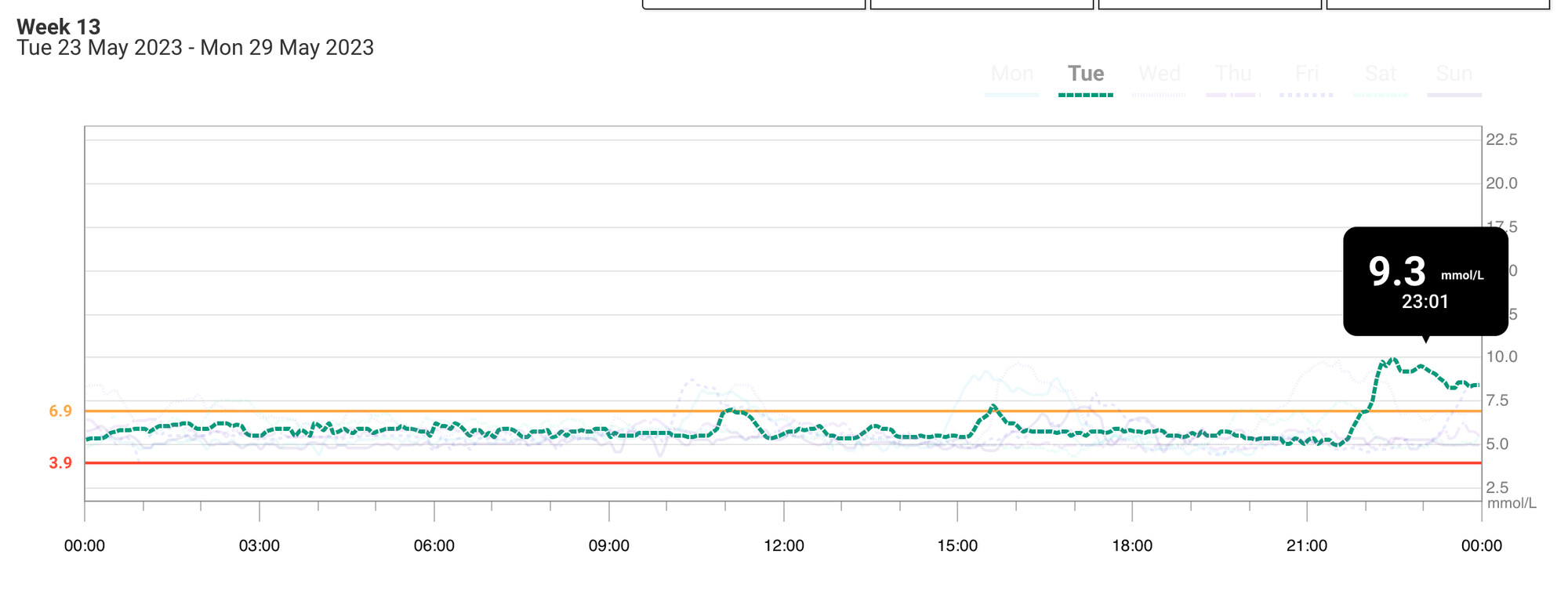
≥ 130 mg/dL (7.2 mmol/L): 5 times/week
≥ 140 mg/dL (7.8 mmol/L): 3 times/week
≥ 150 mg/dL (8.3 mmol/L): 1 time/week
Latest HOMA-IR from early March: 1.4 (glucose: 4.6 mmol/L & insulin: 39.8 pmol/L).
High level it seems like you have definitely improved your glucose dynamics a lot.
(Depending how how you sleep/where you were the CGM the nigh time drops might just be about sleeping on the arm where you are wearing the CGM).
Based on the data you shared I’d probably be more focus on the insulin part of the equation than the glucose. You might still benefit from some more glucose optimization, but ideally not if the cost comes at increased insulin.
Wish we had continuous insulin measurements… I could see how someone having big problems with glucose (more than you have on the SGLT2i + Acar) might lower their insulin peaks via knocking down the glucose more when on GLP1-RAs. Might be the case for you too, but would def try and get as many insulin datapoints before and after the GLP1-RA experiment if you decide to do it.
Would also try and see if there is data in non-obese/non-bariatric surgery/non-diabetes humans and mice about the direction of insulin on GLP-1 meds.
Btw, what are your IGF-1 levels? If they are not as low as you’d like from a longevity phenotype you might be want to be a bit more concerned about risking to increase your insulin levels.
(the issue I don’t think we know enough about is also to what extent the GLP-1 impacted insulin levels are increased 24/7 and not just associated with the postprandial pattern of going up, but then down again).
Lastly, have you explored doing some of the non-medical things to lower glucose (more fiber, order of eating different foods, some movement after meals, using vinegar and things like cinnamon going into meals, finding ways to destress / lower cortisol levels, etc, etc, etc)?
I didn’t know that it could cause hypos. Do you have sources on this by any chance?
Besides the longevity risk–benefit assessment, I want to stop my post-(big) meal symptoms and improve my quality of life. If the cost is increased insulin, I might be OK with it.
Yes, I couldn’t find such data. The results of semaglutide for CKD will be published soon, so hopefully, the full results should show insulin levels before and after among non-obese and non-diabetic people.
I think I’ve never measured it. What should I read about this?
I do ~ 80% of these things (I’m also a Zoe client). It helps, but not enough.
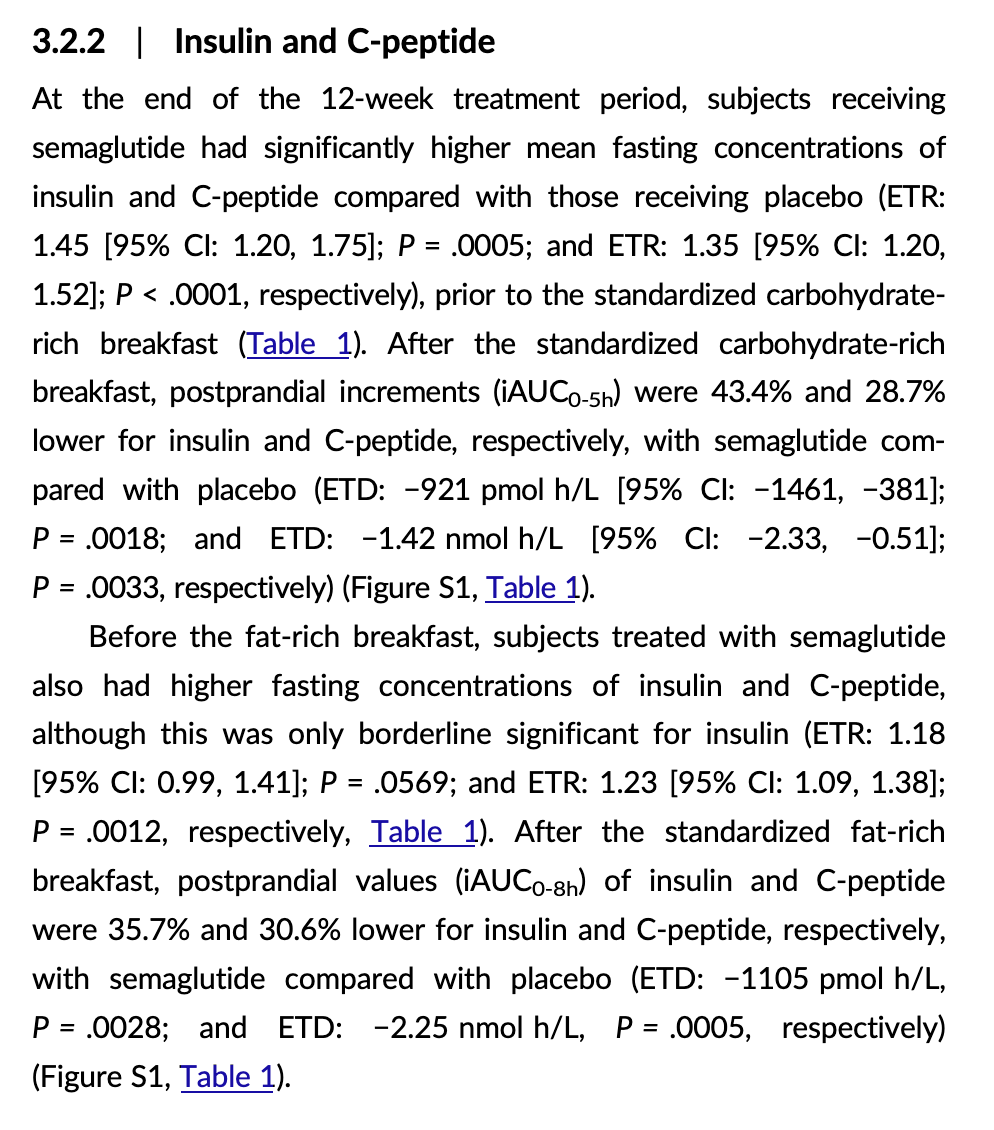
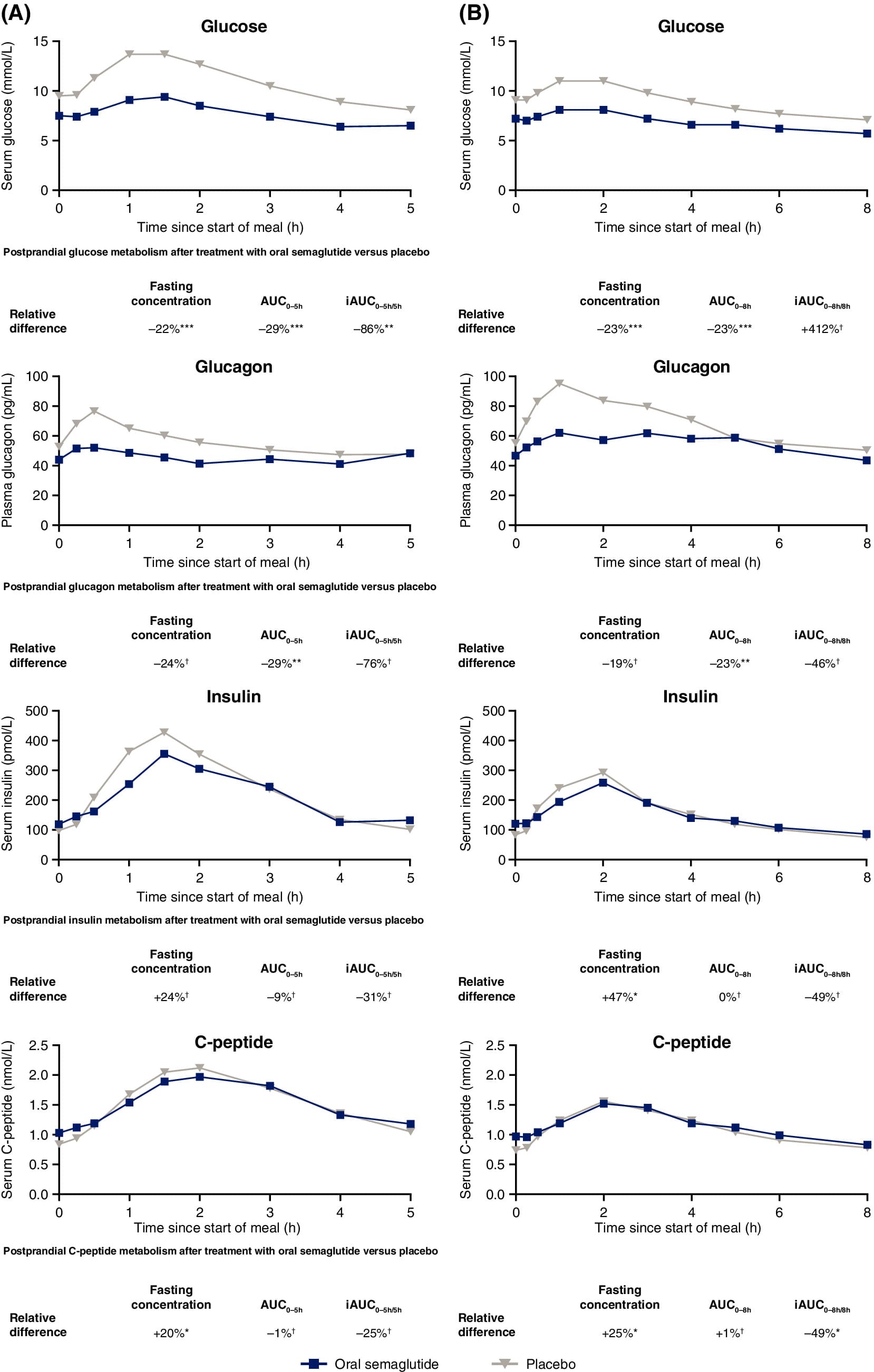
If I understand correctly, semaglutide increases baseline insulin levels by ~40% (fasted state), but it decreases post-meal insulin levels by about 40% as well. Do we know if, for insulin, what matters is the time in range (not exceeding a certain threshold) or the area under the curve (“the lower the better”)? If it’s AUC, then semaglutide might be bad (+40% 24/7 but -40% 3 times per day after a meal). If it’s time in range and the +40% in fasted state is still below the “threshold” and the -40% post-meal helps people not going over the threshold, then it’s semaglutide is a net positive. (not sure if my reasoning is correct though…)
I noticed it when I was lying down on that arm in the sofa. And then replicated it many times. And think I also heard others here having noticed it. You can probably experiment with it yourself, just try lying on the arms/sensor at different angles for 5-7 minutes.
Here is the first thing that comes up when I googled it:
When pressure is applied to a CGM sensor, such as when a participant sleeps on their side and lays on the sensor, the CGM may read a false low value
Great post and great questions. I don’t have good answers unfortunately.
Btw, one thing you might want to make sure you have considered is around known and unknown poly pharmacy risks/interactions of stacking increasing numbers of prescription drugs.
“The cost of medication is not included in the program’s base price. Without insurance, GLP-1s can cost between $950 and $1,600 per month, Sesame warned on its website.”
So that $179 is for the medical consultation only?
The mean follow-up time was 3.9 years (standard deviation 3.5 years) in the GLP1 receptor agonist group and 5.4 years (standard deviation 3.5 years) in the DPP4 inhibitor group. 76 of 145 410 patients (incidence rate 1.33 events per 10 000 person years) treated with GLP1 receptor agonists and 184 of 291 667 patients (incidence rate 1.46 events per 10 000 person years) treated with DPP4 inhibitors developed thyroid cancer. GLP1 receptor agonist use was not associated with increased risk of thyroid cancer (hazard ratio 0.93, 95% confidence interval 0.66 to 1.31; rate difference −0.13, 95% confidence interval −0.61 to 0.36 events per 10 000 person years). The hazard ratio for medullary thyroid cancer was 1.19 (0.37 to 3.86). In the additional analysis comparing the GLP1 receptor agonist group with the SGLT2 inhibitor group, the hazard ratio for thyroid cancer was 1.16 (0.65 to 2.05).
Also, I was told that although semaglutide doesn’t cross the BBB at all (contrary to exenatide and lixisenatide, which cross it very well), it’s still transmitted to the hypothalamus. Also, as the BBB in PD and AD is more porous, semaglutide might cross it in these populations. (poke @DrFraser)
@adssx
I’m not sure if this article has been viewed. Brain activation by area - Semaglutide (and others)
For an agent that doesn’t cross the blood brain barrier it certainly has some effects.
What do others make of this? The oral levels are clearly not getting anywhere near as high as the subcutaneous ones - but I appreciate the ease of giving patients something orally as in the Phase 2 study above.
I’m in a tight spot with patients financially, as we can easily and cheaply get semaglutide and tirzepatide - both of which likely have these impacts seen in this article. However, no significant brain level. Is it the brain level or is it the effect on the brain activation.
It’s a big deal to go from essentially $100/month for those agents vs. $1000/month for things like Trulicity - not even to mention the availability issues with the Rx GLP-1’s. Surprisingly with even the ones that don’t cause major weight-loss being in short supply many places.
Edit: Just found that Empower Pharmacy, the group I use for Semaglutide and Tirzepatide also compound Liraglutide. It’s about $260 per month at maximum dose. Certainly getting a little more affordable, at least for some people who have early PD and trying to stop progression. Sadly still not getting same brain levels as Trulicity.
I’ve stopped Rybelsus aka oral semaglutide. I lost 10 pounds, but the side effects of elevated HR, sharply decreased HRV, constipation and fatigue just weren’t worth it. After the fatigue finally got a bit better after about 4 weeks on the 7mg dose, the appetite suppression also seemed to go away. No WAY was I going to through another month of this (or worse) by starting the 14mg tablets.
After washout, I’m considering trying the 7mg dose for short periods of time during a 5-day Prolon fast in the hope of getting all the benefits of the fast while taking the edge off the hunger. I only hope that the mild insulin-raising effect isn’t enough to blunt the increase in autophagy which is one of the main reasons for doing the FMD in the first place (!)
Do they have exenatide (Byetta, Bydureon)? It’s THE best for brain levels.
Interesting fact: in the lixisenatide trial people with Parkinson’s did NOT lose weight. Similarly, the weight loss effect of GLP-1RAs is way lower on non obese people with T2D vs obese people. Did you notice significant weight loss in your non obese PD patients @DrFraser?
In regard to the compounders - I was shocked to find the Liraglutide as the focus with them isn’t to replace meds for people who have T2DM, as they are usually eligible for insurance coverage. It is for meds that people wouldn’t have access to via a regular Rx, and for meds that are expensive and would be cash pay. The classic example is Ozempic/Mounjaro. Given that someone wouldn’t usually be taking Exenatide off label - as it isn’t much good for weight loss comparatively; there just isn’t demand for it.
Certainly with meds like Semaglutide (Ozempic/Wegovy) and Tirzepatide (Mounjaro, Zepbound) it really doesn’t make a big difference if you are ideal body weight and not diabetic - most people will have very substantial weight loss, which is dose dependent. It can certainly be a real limiting factor for prescribing these for neurocognitive decline, as sarcopenia is an independent risk of poor outcome, especially in PD, but I also believe in AD.
Fortunately, living in America … only a small % of patients have no weight that would be beneficial to lose, so it is only occasionally a limiting factor.
The data however needs to come through on the more potent GLP-1 agonists that don’t necessarily get brain levels but have powerful effects on the brain. By choosing something like exenatide or dulaglutide which get good brain levels, but are less potent GLP-1’s than our newer agents - if the effect is a brain level - then these older drugs end up being the winner - however if GLP-1 activity ends up being the active ingredient, then we end up giving a weaker agent by chasing a brain level when this may not even be the reason for the benefit.
This article above somewhat goes through some of that discussion. Given the powerful behavioral changes which seem to correlate best with more powerful GLP-1/GIP agonists … I suspect the potency of the drug will end up being the active ingredient. Just can’t prove it today.
I have patients pursuing GLP-1’s with brain levels and others who are pursuing potency. My personal choice right now is for potency, but for neurocognitive decline/PD it seems like not putting all of one’s eggs in one basket is smart - so Rapa+SGLT2+PDE5+GLP/GIP/Telmisartan is probably a reasonable starting point (plus optimize other things like lipids/BP/Weight/Glucose/Sarcopenia). If one or more of these end up not panning out - the others will still be there.
That’s my current approach - and it will certainly evolve as more data comes in.
As usual - no medical advice meant here to anyone - just putting forward my present thoughts.
Collectively, the HbA1c and weight-lowering potential of oral semaglutide (7–14 mg) appear to be nearly similar to injectable semaglutide (0.5–1.0 mg) and larger than other GLP-1RAs, currently approved in people with T2D. […] Notwithstanding, unlike injectable semaglutide which has shown a significant reduction in MACE (SUSTAIN 6) and has an additional label for cardiovascular (CV) risk reduction, oral semaglutide is yet to show CV superiority over placebo (PIONEER 6). Since PIONEER 6 was not powered to assess the CV superiority of oral semaglutide over placebo, the SOUL (Semaglutide cardiOvascular oUtcomes triaL, NCT03914326) has been specifically designed for this purpose and is estimated to be complete by July 2024.