Yes, hahaha - I guess its a Deck- Pec - I can do 190 lbs 30 reps in a set. The medical students call it the chest/fly machine. Been stuck at 190 lbs for a year or two. I weigh about 190 right now. If I go up to 200 lbs with no stress - for me that would be a significant improvement.
As you might guess, he is booked solid. He has 3 offices in the area - all rural Missouri - Unfortunately, he doesn’t do telemarketing. Younger progressive doctor. My visit yesterday, he old me his personal practice will be focusing more on weight loss and hormone therapy, but I will still get total care.
Very focused on shared research and worked with me. Has been a freind for 20 years and my physician for the last 6 years – approved me to go on TRT, Rapamycin, HGH and Empaglizozin SGLT-2 Jardiance and now Maraviroc.
He just took over my Finasteride and Tadalafil prescriptions from my Urologist who is no longer seeing patients due to his own health issues. My PSA is under 1 … at .9 didn’t really need a urologist. I just liked it – and insurance covered the extra physician.
Post-finasteride syndrome is not a real condition. Moreover, dutasteride is a more potent inhibitor of 5ar type 2 compared to finasteride and strongly inhibits 5ar type 1 while finasteride only binds very weakly and reversibly to it. On top of that, finasteride has a half life of 6 hours, totally leaves your tissue within two weeks and from all the rcts and case studies we have, side effects totally disappear within 1-3 months. Dutasteride, on the other hand, has a half life of 5 weeks and can potentially stay in your system for 6-12 months after cessation.
The only reason less mentally ill men claim they got persistent side effects from dutasteride is simply because far less men are on it than on finasteride. But there certainly are forum anecdotes for persistent dutasteride side effects.
The translational protocol you quote is errorenous. AI made a major mistake and didn’t account for species differences in receptor affinity nor differences in delivery method. A proper translational calculation shows 37mg every two weeks is the human equivalent to the dosing the mice received.
Combo - based on his familarity with the drug from HIV infected patients on treatment. We discussed trial and if anything is an issue - immediatley get in touch with him. Was the same for starting rapamycin as an early adopter. We selected a 3-month visit plan and daily outreach if any issues arose. Nothing ever happened. But, back then it was even more experiemental - with a dosing plan 6-8 mg weekly.
He perused a few articles on Maraviroc and the one posted by RapAdmin with the translational information during our visit - we spent over an hour chatting on everything longevity as it pertains to my protocol. Pretty typical visit because he is fascinated by my progress and benefits. Calls me a medical case study in improvement and longevity. He is about 46 years old. So, maybe preparing for his future too.
The HIV dosing is designed to provide continuous receptor occupation asymptotically approaching 100%. For aging, this sort of dosing is completely unneccessary. I had Claude Opus 4.5 estimate receptor occupancy profiles for differing dosing frequencies using a 37.5 mg dose for a 70 kg individual.
Summary Table: All Frequencies
Dosing Frequency
Peak RO
Average RO
Minimum RO
Time <90% RO
Time <50% RO
Time <20% RO
Daily
98.9%
98.4%
97.5%
0%
0%
0%
Every 2 days
98.4%
96.0%
92.0%
0%
0%
0%
Every 3 days
98.2%
93.0%
81.8%
25%
0%
0%
Twice weekly
98.1%
91.0%
75.0%
35%
0%
0%
Weekly
98.0%
65.0%
13.0%
62%
30%
12%
Every 10 days
98.0%
45.0%
1.2%
73%
50%
33%
Biweekly
98.0%
28.0%
~0%
79%
64%
50%
The optimal receptor occupancy for anti-aging benefits is unknown. The mouse studies achieve low occupancy. I think this is an artifact of mouse receptor binding affinity rather than by design. The key piece of information from the mouse studies is that despite low occupancy, significant benefits were seen. Analyzing the mechanisms of action seems to indicate better benefits would be achieved with continuous 50-80% occupancy, but again this is speculation. The biweekly dosing best represents the mouse study profiles. Taking everything in aggregate, I’ve decided to move to dosing 37.5 mg/weekly.
Really appreciate your deep dive here @fasterfour . Maraviroc is a totally new opportunity in muscle growth and strength… so of course still seeing what protocol is best. And, accounting for diffences by genotype and phenotype.
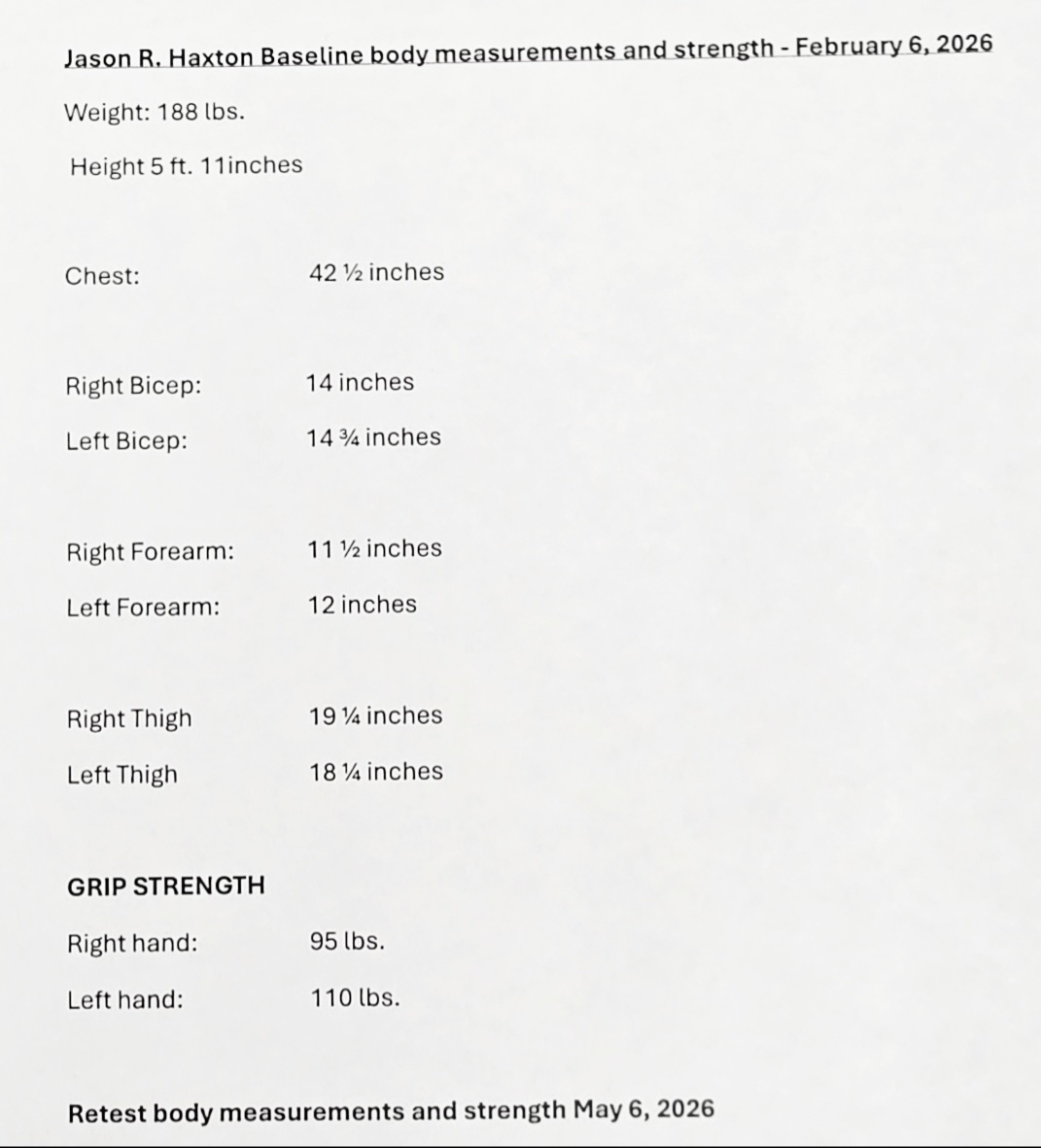
Should be receiving my Maraviroc today, as I mentioned, only 1 out of 3 pharmacies stock it… or have access. So my main pharmacy sent my prescription to another pharmacy to be filled. I have my baseline bicep and chest measurements. And my workout routine for past year… machines, weight amount and sets.
I am planning on a doing a loading dose of of 32 mg daily for a few weeks… much like you would do when starting Creatine. Then, see about backing it off, same dose every 3 days. Try this for 3 months and compare muscle growth measurements and any workout improvement in weight load and reptition number per set, to baseline.
Should have something to report by end of April or early March.
I am glad you lift regularly (so later strength measurements are not confounded by newbie lifting gains) and have some pre-Maraviroc baseline benchmarks to compare against.