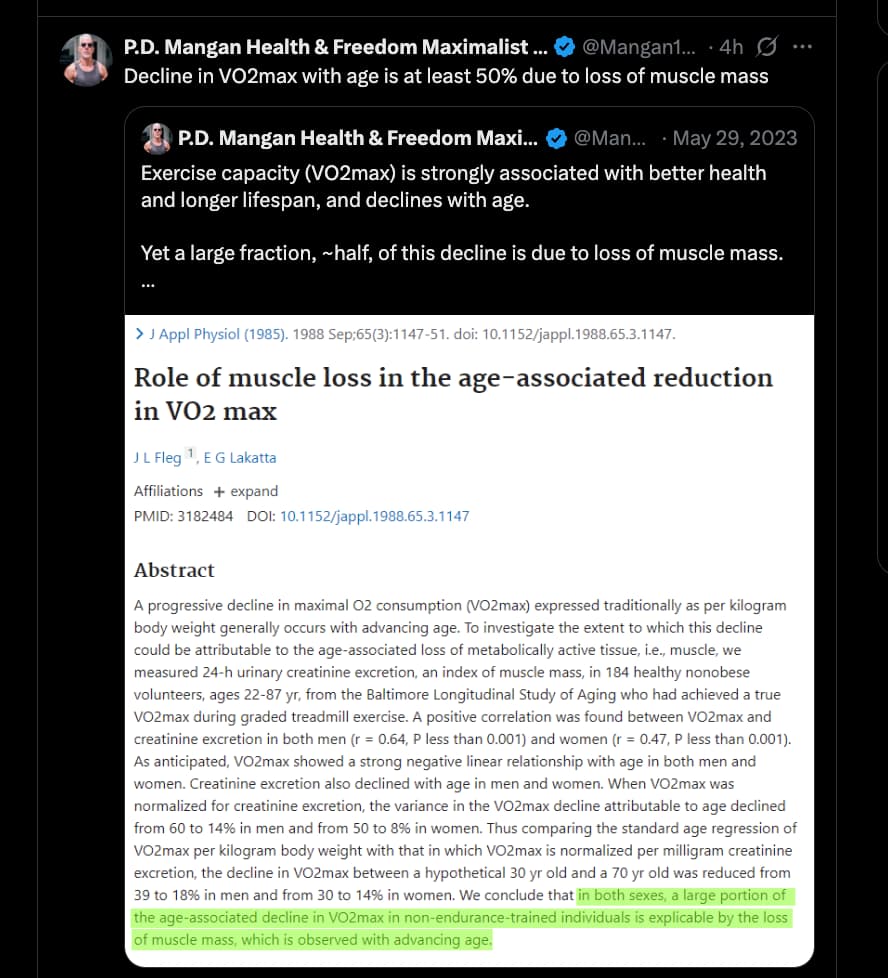
Exactly this happened to me. My VO2max used to be 48, but after I had surgery and had to stop running, it dropped to 38 in a year or so. I still walk about 10k steps a day and use my bike instead of the car whenever possible, but it clearly isn’t enough to maintain it.
I’m about to start training again and add some running back into my workouts, and I’m hoping to regain at least some of that VO2max.
I’m about to have surgery and will be unable to exercise for a few weeks at least. I also had to stop exercising because of spinal disc problems (hence surgery) for a couple of months, and I could tell my conditioning absolutely collapsed. Muscle decline was even more stark. Just a couple of months ago I was doing very strenuous squats including jumping squats with a 45lbs weight vest, and now I’m winded after 5 minutes of bodyweight squats.
I have noticed that with advancing age (I’m 67), you decondition extremely rapidly. When younger I could stop exercising and the decline in exercise capacity would be quite gradual. Now I stop exercising and my conditioning falls off a cliff.
Now that the diagnosis has been made, and a surgery date set for late December, I’ve resumed some exercise specially modified to spare the spine, because I will be immobilized for many weeks after the surgery and I don’t want to emerge from this with sarcopenia and frailty. I’m trying to build up some reserve.
As has been observed, older people decline in stages. There’s an event, you decline some and regain only part of your previous physical capacity. Then there’s another event and you decline further and so on. The trick is to try to regain your full exercise capacity after an event. That is what I am determined to do. I may have to adjust my exercise protocol, but I must do all I can to get back to 100% of my previous capacity.
For example, right now I cannot jog for longer than about 10 minutes due to spine issues. So instead, I’m doing a series of “high knees” intervals. It’s incredibly taxing on your cardio, I at present cannot do more than about 15 seconds in an interval (with proper form and max effort). So I do about 5 of those a day. I’m hoping to gradually increase the intervals, so in a few weeks before the surgery I’m at least in better shape and not like a human jellyfish. We’ll see.
Bottom line: you must fight to get your VO2Max back to a higher level and not allow an event (like surgery) to permanently set at a lower level. With age there will be a gradual decline anyway, but you try to avoid sharp drop offs after forced episodes of non-exercise.
After surgery and recovery, that will be my challenge. I must get back 100% of my conditioning and muscle strength and power. I am absolutely determined to meet that challenge.
I’m 50, absolutely fit, feel decades younger, and a “simple” surgery set me back hard. It took me over a year just to rebuild my strength, and now I probably need another 6 months to get my endurance and VO2 max back. I totally get now how having surgery at an advanced age can basically wipe you out physically.
An interesting piece from this year’s BSRA conference was that exercising the day before surgery helped reduce the harm to fitness from surgery. Not two days before, however.
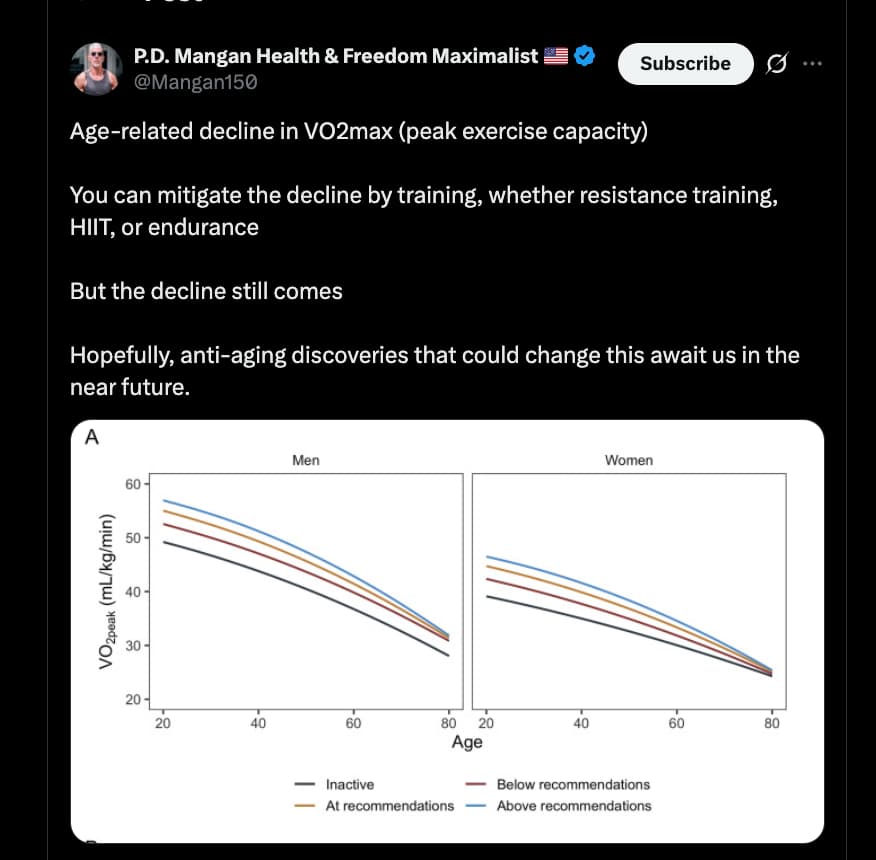
Looking at that graph, it seems the older you get, the less you benefit from exercising more than just enough not to be completely sedentary. I’ll save my time (as I don’t enjoy exercise and do so exclusively for health benefits), and do just enough to extract most of the benefits (roughly within recommendations) and bank the rest of the time to add to my actual “life enjoyment”. Ultimately, time is the only thing we can’t make more of, so each minute is precious. YMMV.
That guy seems to disprove the graph above. But working out for 3 hours per day is probably not on your plans.
Details here from CGPT5.1:
Here’s a summary and analysis of the paper titled “How to Be 80 Year Old and Have a VO₂max of a 35 Year Old”(How to Be 80 Year Old and Have a VO₂max of a 35 Year Old, Karlsen et al., 2015).
Executive Summary
The paper reports on a case study of an 80-year-old man whose measured maximal oxygen uptake (VO₂max) was 50 mL·kg⁻¹·min⁻¹ (3.31 L·min⁻¹) — very high for his age.
His cardiopulmonary, vascular and muscle metrics were all well-above expectation for someone his age: strong left ventricular systolic & diastolic function, excellent pulmonary diffusion capacity, above-average blood volume/hemoglobin mass, and a large skeletal muscle mass (49 % skeletal muscle mass) for his age.
The subject had a lifelong history of physical activity, both endurance and strength training, and a very high daily activity level in his 80s: ~10,900 steps per day and approximately 2:51 hours per day of physical activity (moderate + vigorous) logged via a wearable.
The authors suggest that his very high VO₂max is attributable to the combination of lifelong activity, maintaining a high fitness baseline, excellent organ/system function, and high ongoing activity volume. They note that while most decline in VO₂max with aging is inevitable, starting high and remaining active may mitigate the decrement.
The paper frames this as more than an extraordinary outlier — it offers “how” someone at 80 yrs can have physiological fitness of someone decades younger — though as a single case it cannot establish causality or generalize widely.
Farm work from youth, endurance and strength training across life
The background context.
Level of Exercise / Physical Activity to Achieve This VO₂max
From the data in the paper, we can infer what level of exercise this person performed. Important to note: the paper does not provide a detailed training log with weekly hours at specific intensities for the last decades, so some inference is needed — but the measured objective data (daily steps, active time, lifelong training) gives us a solid estimate.
Key points to infer exercise level:
The subject logged 2:51 (hours:minutes) of physical activity each day (measured by activity sensor) when in his 80s.
He logged ~10,900 steps/day.
The activity sensor data broken down indicated ~1050 min·week⁻¹ of moderate activity and ~147 min·week⁻¹ of vigorous activity (i.e., ~15.75 h/week moderate + ~2.45 h/week vigorous) — note this appears in discussion as “seven times” and “two times” the recommendations for moderate and vigorous physical activity respectively.
The authors write: “He is moderately and vigorously active, 1050 min·wk⁻¹ and 147 min·wk⁻¹, which is seven times and two times above the recommendations for moderate and high-intensity physical activity of ≥150 min·wk⁻¹ and ≥75 min·wk⁻¹, respectively.”
The subject also reported “~ 90 min/week of structured endurance and strength training” by self-report (though the authors note self‐report is low and actual activity was much higher in daily non‐structured movement). This suggests that the bulk of his high activity level was from unstructured daily movement + lifelong lifestyle rather than just structured training.
Therefore, a practical summary of the exercise level:
Daily movement: ~11,000 steps/day (which for many people is ~8–10 km walking equivalent, depending on stride length) plus additional dynamic movement (e.g., farm work style, strength training).
Active time: ~3 hours of moderate + vigorous activity each day.
Lifelong consistent training: The subject had been physically active from youth (farm work) and maintained both endurance (e.g., cross-country skiing races into older age) and strength training.
The authors note that volume (not just intensity) seems very high compared to typical older active individuals and likely contributed to maintaining such a high VO₂max at age 80.
In short : This man was well above typical activity guidelines — around 7× the recommended moderate-intensity volume and 2× the recommended vigorous-intensity volume (in his 80s), plus high muscle mass, strong organ reserve, and lifelong training history.
Actionable Insights (for your domain of longevity / health)
For someone aiming to push VO₂max (or maintain a high VO₂max into older age), merely meeting the guidelines (150 min moderate / 75 min vigorous per week) may not be sufficient; volume and consistency matter greatly. This case indicates ~1000 min/week moderate + 150 min/week vigorous (~18 h/week) in old age.
Lifelong maintenance of activity (endurance + strength) appears critical. Starting early and keeping up high levels of activity likely built a higher baseline which made later maintenance feasible.
In older age, significant movement volumes (steps/day, hours of active time) may help preserve VO₂max; structured training alone isn’t the full story — daily lived movement matters.
Strength training and muscle mass appear relevant: high skeletal muscle mass (49 % in this subject) likely supported mitochondrial capacity, peripheral oxygen utilization, and thus VO₂max.
Monitoring daily movement (steps, active time) in addition to structured training might be useful in longevity protocols aiming to maximize cardiorespiratory fitness.
Well, a graph like that is not pulled out of thin air. It represents human data, what a member of the human cohort can expect. That’s reality, even if we wish it were not so. Decline is the norm, even among athletes. Note, that athletes outlive the general population on average by only a small number of years, around 3 or so in most countries. But can you have exceptions like that 80 year old? Sure! But so what, it’s the vast majority that matter. Calmet lived to 122, is that someone to point to when speaking of even the most health obsessed among us? Is Calmet really relevant to us? Is that 80 year old? Or is that graph by far more relevant? You could make two lines in a graph, all those in numbers who play the lottery, and the second line all those who actually win the lottery. Which line do you think is more relevant to you when you contemplate buying a lottery ticket? Same here - I am not about to devote 3 hours a day, lol, hoping I’ll be lucky enough to get the same results after a lifetime of such exercise as that 80yo… and that’s before we even ask the really relevant question: is that 80yo going to live longer than the next 80yo who only exercises 5% as much as that guy… 3hrs=180minutes, 5%of180minutes=9minutes. I’m willing to bet that an 80yo guy who exercises 9 minutes every single day, will live just as long (and in reasonable shape) as that exercise fanatic 80yo genetic lottery winner. Yeah, thanks, but no thanks !
I enjoy exercising, especially brisk walking or jogging outside in nature - it makes me energized (especially jogging) and clears my mind. Swimming is another enjoyment, especially in combination with sauna. I also like to skate at least once a week. What I don’t like is lifting weights or doing resistance training. Time is precious - you are right!
Worst graph ever. Could be a winner of a contest for the most useless and inscrutable graph with random numbers and colors the meaning of which is not labeled. Life is too short. Pass.
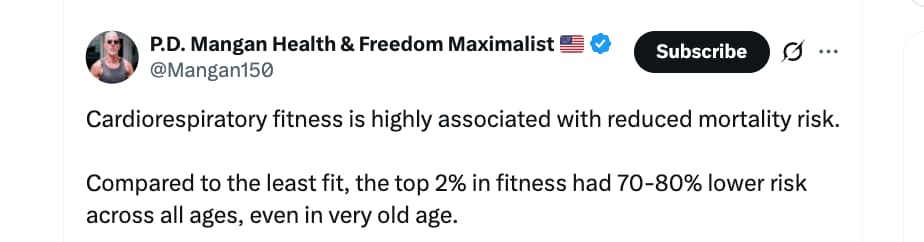
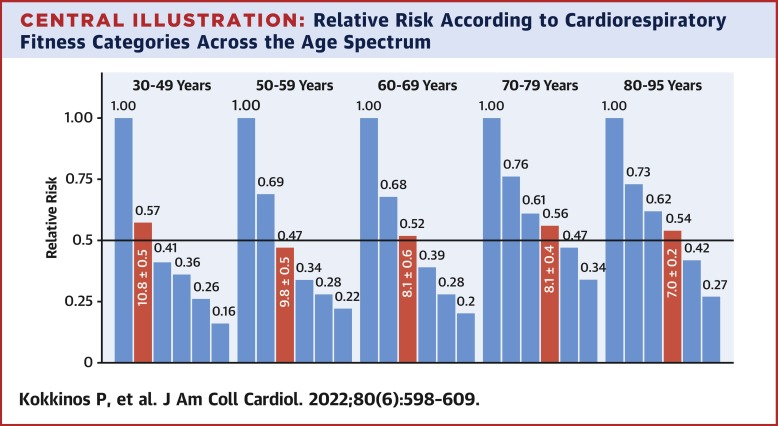
The association of CRF and mortality risk across the age spectrum (including septuagenarians and octogenarians), men, women, and all races was inverse, independent, and graded. No increased risk was observed with extreme fitness. Being unfit carried a greater risk than any of the cardiac risk factors examined.
In the paper Cardiorespiratory Fitness and Mortality Risk Across the Spectra of Age, Race, and Sex (Kokkinos et al., J Am Coll Cardiol 2022) the authors define levels of fitness (cardiorespiratory fitness, CRF) as follows:
Definition of fitness‐categories
CRF was measured via peak exercise capacity in metabolic equivalents (METs) achieved during a standardized treadmill exercise test. (PubMed)
Participants were categorised into age‐ and sex‐specific fitness groups using quintiles plus the 98th percentile (i.e., extremely fit) based on their peak METs. (PubMed)
In effect:
“Least fit” = ~20th percentile of peak METs (approximately mean ~4.7 ± 1.5 METs in this cohort) (ResearchGate)
“Extremely fit” = ≥98th percentile of peak METs (approximate mean ~14.5 ± 2.1 METs) (ResearchGate)
They report that the lowest mortality risk was around ~14 METs for both men and women. (PubMed)
They also provide age‐group thresholds for ~50 % reduction in mortality: ~11.0 METs (age 30-49), ~10.0 METs (50-59), ~8.0 METs (60-79), ~7.0 METs (≥80). (ResearchGate)
In summary: “fitness levels” are defined relative to the cohort’s age‐ and sex‐specific distribution of peak METs: the lowest quintile (“least fit”) vs the highest (~98th percentile, “extremely fit”), with specific MET cut-points reported in the paper.
Caveats
The authors do not provide universal absolute cut‐points (e.g., “low fitness = <X METs”) that apply across all ages/sexes; rather they use population‐based percentiles stratified by age and sex.
Because they stratified by age and sex, the exact MET cut‐points for quintiles will vary by age group and sex.
The study cohort was US veterans, so generalisability to other populations may be limited.
They emphasise that changes in fitness over time were not accounted for (they only used the single baseline exercise test). (Health Sciences Research Commons)
Mapping JACC Study Categories to Real Activities
The JACC paper’s fitness categories roughly translate to:
Least fit (~4–5 METs)
Speed: 3.0–3.5 mph walking
Everyday meaning: unable to sustain uphill vigorous walking
Clinical equivalent: frailty threshold for many age groups.
Moderately fit (~7–8 METs)
Speed: 5.5 mph jog (~11:00 min/mile)
Fit (~10–12 METs)
Speed: 6.5–7.5 mph run (~8:00–9:30 min/mile)
These people have markedly lower mortality risk.
Extremely fit (≥14 METs)
Speed: 8.5–9.0 mph run (~6:40–7:00 min/mile)
Equivalent to high recreational fitness or competitive amateur ability.
Elite (16–18 METs)
Speed: 10 mph+ (sub-6:20 pace)
This corresponds to strong competitive age-group runners or elite cyclists/triathletes.