Your point is well taken, but not applicable in this instance. Per the paper, the oral “gavage group received 1.5 mg/kg rapamune”. That’s the nanoparticle-based pharmaceutical formulation you reference at the end of your post.
The daily intraperitoneal injections used in the study @hunterama1 mentioned (Liu et al. 2017) would result in significantly higher levels of everolimus than the 3 times a week every other week intraperitoneal injections of rapamycin used in the study I had just mentioned for comparison (Leontieva et al. 2014). It’s the difference between 14 injections and 3 in a two week period.
I referenced that Blagosklonny paper because it directly compares the same dose of rapamycin given intraperitoneally and orally. But, the different pharmacokinetics of intraperitoneal injections and oral intake are widely known within fields that work with rodents. Most drugs injected i.p. absorb rapidly because the peritoneal membrane has a large surface area and a rich blood supply. So, i.p. injections typically result in higher bioavailability and a faster onset of action compared to the oral route. Drugs injected i.p. typically clear faster, too.
Here’s Matt Kaeberlein on the topic:
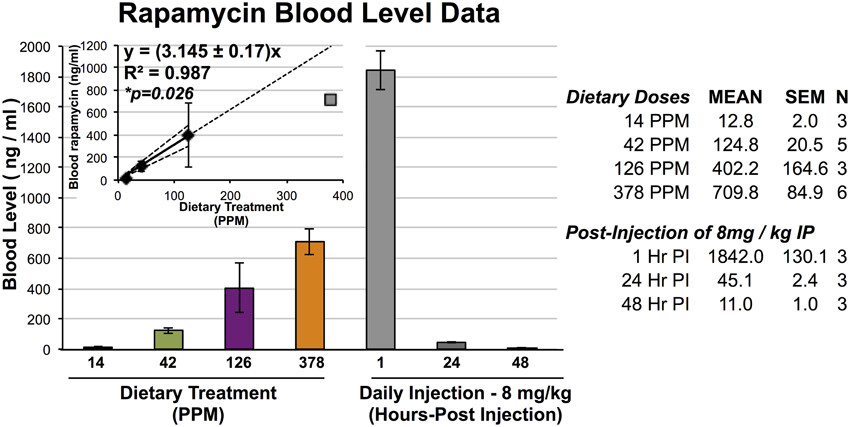
Analysis of rapamycin levels in blood suggests that daily i.p. injection of 8 mg/kg yields blood levels of around 1800 ng/mL one hour after injection and 45 ng/mL 24 h after injection (Johnson et al., 2013c). For comparison, blood levels of 3–4 ng/mL rapamycin were measured following dietary delivery at 14 ppm in the same mouse strain (Zhang et al., 2014) and studies from the ITP have reported between 9–16 ng/mL at this dose and 23–80 ng/mL in animals receiving the 42 ppm rapamycin diet (Miller et al., 2011). Thus, daily i.p. injection of 8 mg/kg rapamycin, which appears to be well tolerated in wild type mice (Johnson et al., 2013c), yields circulating levels of the drug that are at least 20-fold higher than the highest concentration that has been carefully tested for effects on normative ageing. (Kaeberlein 2014)
Here’s a helpful figure from (Johnson et al. 2015):
And, to get a better sense of the comparative doses, here’s the math for the highest oral dose:
378 PPM = 378 mg/kg of food = 0.378 mg/g × 4 g average mouse food consumption = 1.512 mg / 0.025 kg average mouse body weight = 60.48 mg/kg body weight.
Approximately 60 mg/kg body weight of encapsulated rapamycin (the same formulation used by the ITP) yielded 709.8 ng/mL, while 8 mg/kg body weight of i.p. injected rapamycin yielded 1842.0 ng/mL.
I hope that clears things up.