[Note: Avi got some of the details wrong here, Rapamycin has improved lifespan by up to 26% and over 29 labs have confirmed lifespan improvements, TAME trial has not been funded, etc. but the generalities and the cost information is correct]
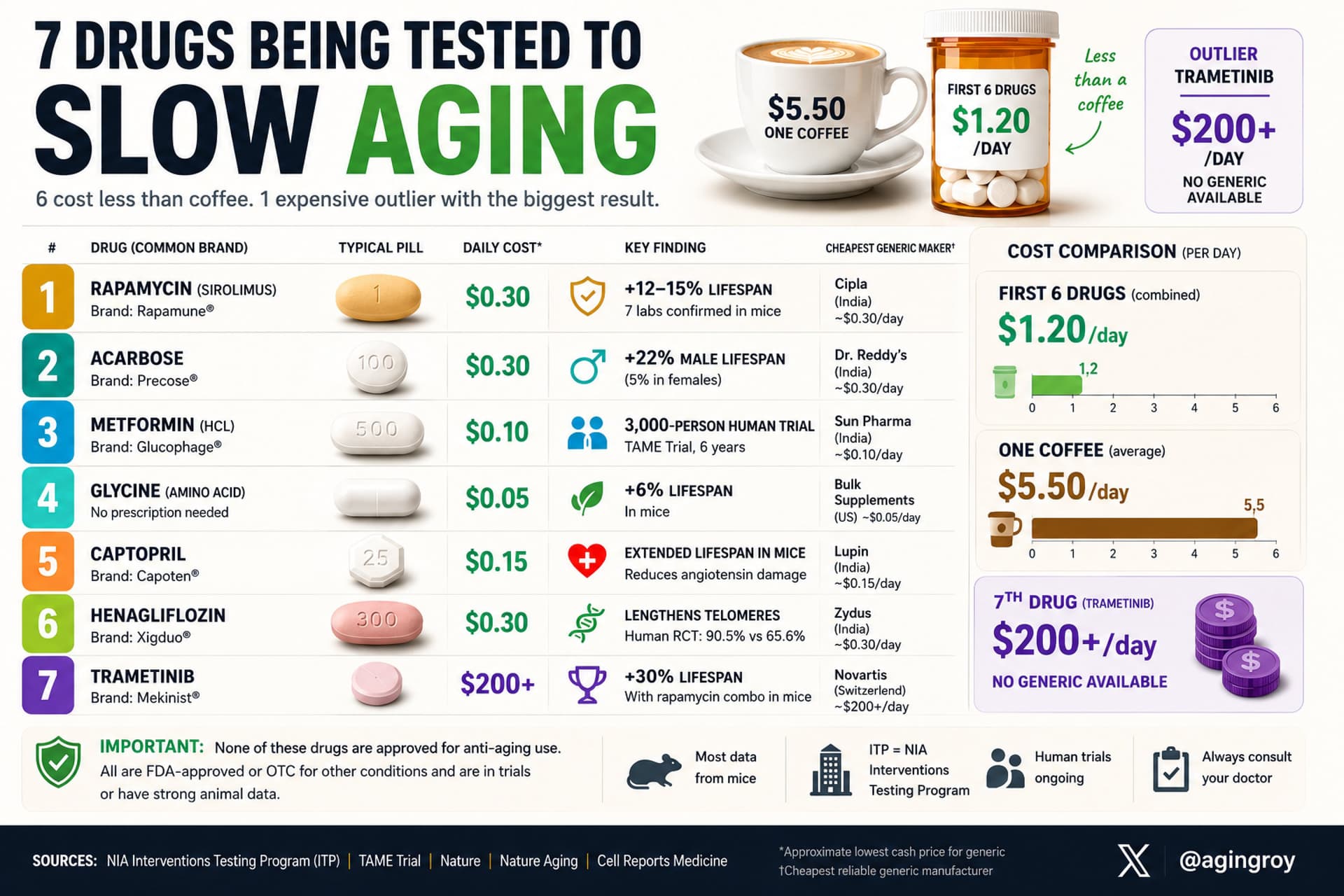
6 drugs under $1/day being tested to slow aging (plus 1 expensive outlier with the biggest result):
Rapamycin ($0.30/day) - Extended lifespan 12-15% in mice. 7 labs confirmed. Human trials ongoing for immune aging.
Acarbose ($0.30/day) - Extended male mouse lifespan 22%. Diabetes drug since 1995. Slows glucose spikes.
Metformin ($0.10/day) - TAME trial (3,000 people, 6 years) testing whether it delays age-related disease. Most prescribed diabetes drug in history.
Glycine ($0.05/day) - An amino acid. Extended mouse lifespan 6%. Costs less than coffee. Available without prescription.
Captopril ($0.15/day) - Blood pressure drug. Extended mouse lifespan in ITP. Mechanism: reduces angiotensin damage.
Henagliflozin ($0.30/day) - SGLT2 inhibitor. First drug to lengthen telomeres in a randomized trial (90.5% vs 65.6%).
Trametinib (expensive, ~$200+/day brand, no generic yet) - Combined with rapamycin: 30% lifespan extension. FDA-approved cancer drug. Included because it produced the biggest aging result ever seen in combination.
None are approved for aging. All are in trials or have strong animal data. Total daily cost of the first six: $1.20.
Note: The prices quoted here are the prices we see from Indian Pharmacy vendors (not necessarily from US vendors, though sometimes places like CostPlusDrugs have similar pricing on some of the medications). See: List of Reliable Online Pharmacies.
I posted information about a rat lifespan study along with a study reference and link. And rather than having the courtesy to click on it and take a look, you responded with a curt “Wrong” and a link to a third-party website listing lifespan data for worms and mice.
Sorry wrong is not correct but a 2011 study that isn’t in DrugAge might be irrelevant. Here it’s a non-peer reviewed abstract report. If the result was so good, surely they would have published it?
Actually “Wrong” was probably the correct assessment:
Prior to this rigorously designed study conducted by the Interventions Testing Program, a 2011 report documented that glycine supplementation could enhance longevity in male Fisher 344 rats (Brind et al., 2011). Although glycine at different doses was reported to extend median lifespan by up to 28.4% and maximum lifespan by up to 30.8%, an analysis using the Wang/Allison method (Wang et al., 2004) found that maximum lifespan was only significantly extended by an 8% dose (Miller et al., 2019).
The rat study was the basis for the ITP testing in mice. If the ITP team had seen no merit in the findings, they likely would not have prioritized glycine for formal testing. Although the subsequent ITP study was more rigorously designed and conducted across three independent testing sites, it was performed in mice, so it does not invalidate the earlier rat results. Moreover, rats are a valuable model for gerontological research because they are larger, have longer lifespans than mice, and often show stronger physiological parallels to humans. For example, cardiovascular and renal function. I did specify 8% glycine above.
On the glycine discussion: among those of European descent, I believe 10-11% are BHMT-08 (rs651852 (A,A), as I am. This genotype may want to consider modifying its glycine and several related supplement parameters. I found the topic to be a deep dive contingent on so many specific related issues that it is better undertaken by the individual rather than posting a generic analysis here.
Henagliflozin has shown some impressive benefits. I have been trying to obtain some for testing, but it only seems to be available in China. The drug shown in the chart is another “flozin”. Any ideas ?
The proven benefits for dapagliflozin and empagliflozin and waaaaaaaay better than one unreplicated Chinese paper showing benefits for henagliflozin. If correct, it is also likely to be a class effect.
Wait, shouldn’t we be analyzing the drug itself? As a novel SGLT2 inhibitor , henagliflozin innovatively incorporates a fluorine atom into its structure and utilizes an L-proline co-crystal formulation. Moreover, in terms of both glucose-lowering and blood pressure-lowering efficacy, henagliflozin consistently ranks in the top two. True, it currently lacks cardiovascular outcome trials , but that’s simply because it’s a new drug. Furthermore, henagliflozin can significantly extend telomere length, and its anti-aging mechanisms are already well-established, so I won’t belabor the point here. Price-wise, it is also the most expensive per milligram. Clearly, this is one of the top drugs that anyone focused on anti-aging should be taking.
Furthermore, claiming it ‘lacks replicate validation’ is simply inaccurate. Henagliflozin is already backed by multiple clinical studies, and a recent paper detailing its ability to extend telomere length was published in a Cell sister journal.
Glycine might be a minor improver of lifespan, but it’s honestly really great for sleep, which is the main reason I take it. I found it increases the amount of slow wave sleep I get by about 20 minutes, up to a total of 2 hours on average, and that’s pretty good overall.
To contextualize henagliflozin within the broader SGLT2i landscape, its selectivity profile places it among the highly selective “pure” SGLT2 inhibitors, sitting slightly below empagliflozin but above dapagliflozin.
Drug Molecule
SGLT2 IC50 (nM)
SGLT1 IC50 (nM)
Selectivity Ratio (SGLT2 vs SGLT1)
Primary Clinical / Structural Feature
Empagliflozin
3.1
~8,300
~2,700-fold
Highest selectivity among major FDA-approved agents; robust CV/renal data.
Ertugliflozin
0.88
~1,900
~2,200-fold
Highly potent absolute SGLT2 affinity at sub-nanomolar levels.
Henagliflozin
2.38
4,324
~1,816-fold
Comparable to top-tier selective agents; minimal intestinal SGLT1 cross-inhibition.
Dapagliflozin
1.2
~1,400
~1,200-fold
First approved highly selective C-glucoside archetype.
Canagliflozin
2.2
~550
~250-fold
Low selectivity; cross-inhibits intestinal SGLT1 to delay local glucose absorption.
Sotagliflozin
~1.8
~36
~20-fold
Intentionally designed dual SGLT1/2 inhibitor; alters proximal gut glucose dynamics.
As mentioned, the drug is too young to have rigorous CV data, but some interesting studies are underway.
1. Myocardial Infarction and Infarct Size Resolution
A randomized, controlled clinical trial (NCT06187727 ) has been tracking henagliflozin’s direct impact on acute cardiac injury. The study evaluates 240 patients presenting with ST-segment elevation myocardial infarction (STEMI) undergoing emergency percutaneous coronary intervention (PCI).
The Endpoint: Patients receive henagliflozin or placebo for 6 months post-PCI. Investigators are measuring dynamic changes in myocardial enzymes, NT-proBNP, and echocardiographic variables to determine if early SGLT2i intervention minimizes definitive infarct size and mitigates adverse post-ischemic left ventricular remodeling.
2. Tissue-Level Myocardial Remodeling via Cardiac MRI
Another highly targeted study (NCT06059287 ) directly compares henagliflozin against metformin in obese type 2 diabetic cohorts over 24 weeks.
The Endpoint: This trial bypasses broad clinical event tracking in favor of high-resolution Cardiac MRI protocols . It tracks structural changes at the tissue level, specifically mapping myocardial morphology, ejection fraction, and changes in myocardial fibrosis—a key driver of diabetic cardiomyopathy and heart failure with preserved ejection fraction (HFpEF).
3. Exploratory MACE Tracking in Prediabetes
The largest prospective trial evaluating henagliflozin’s broader vascular impact is a large-scale prediabetes trial (NCT06448130 ), which initiated enrollment across 50 Chinese medical institutions.
The Endpoint: While the primary goal of this 984-patient study is evaluating the rate of normoglycemic remission over a 24-month horizon, the investigators have integrated tracking of long-term macrovascular and microvascular complications, including exploratory MACE rates, as secondary outcomes.
Relaxing standards a bit, the drug’s vitro selectivity profile and its pharmacodynamic structure are almost identical to empagliflozin. This suggests its cardioprotective actions will fall in this general area.
The company has not applied for US FDA approval and indications are that there is no interest in doing so. Given market conditions and possibly near duplication/overlap, I can understand the position.