I agree, without symptoms, Rapamycin is a reach depending on your age. Unfortunately we also live in a world where you can have people that feel fine, but have genetic markers for heart disease - ApoE4, MTHFR with elevated CRP and CIMT studies that show plaque and thickened inflamed arteries and the cardiologist says that it is a waste of time to order any of that and to let them know when they have symptoms. I think for hormones, most probably should have a symptom issue to take on the risks.
3 Likes
Yeah, when they’re in ER. Western medicine is a SICK-CARE model…NOT prevention.
If you want to increase your chance of living a longer and healthier life…the responsibility falls on yourself.
8 Likes
I hate to say it, but I totally agree.
Scour the literature, weigh the evidence, share your ideas on this site so that they can be challenged, and follow your own symptoms and biomarkers.
Take your health into your own hands and then use specialists as a source for advanced testing.
10 Likes
The manufacturer of the enteric capsules responded to my query. They referred me to their dissolution report.
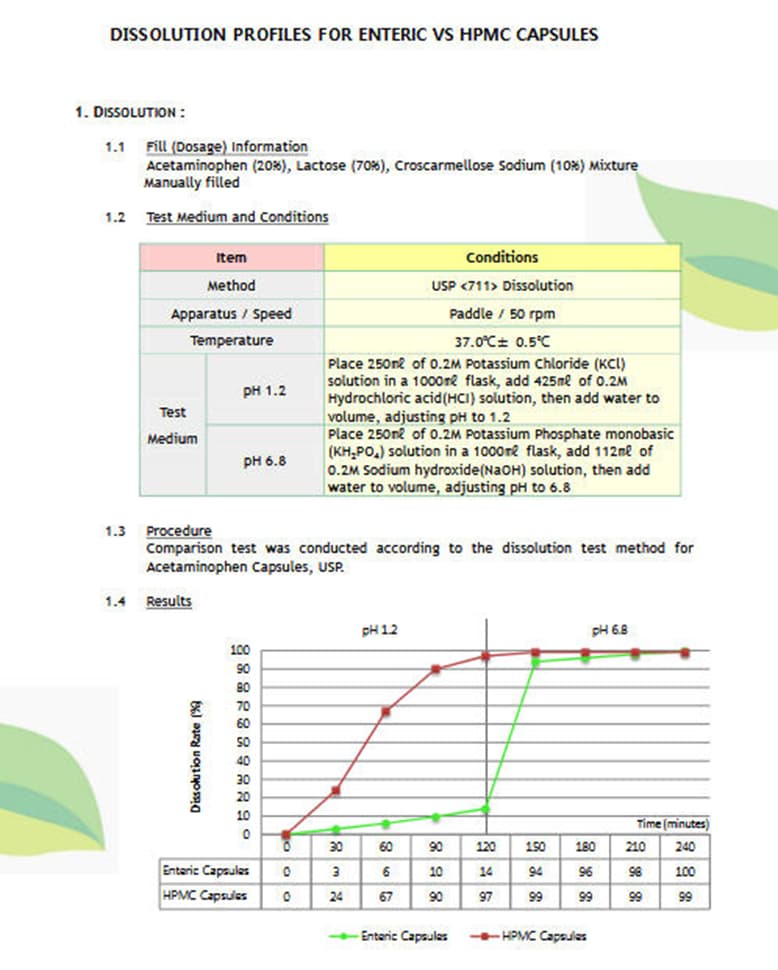
Here is the Definition of dissolution, from USP.org :
Dissolution is the process in which a substance forms a solution . Dissolution testing measures the extent and rate of solution formation from a dosage form, such as tablet, capsule, ointment, etc. The dissolution of a drug is important for its bioavailability and therapeutic effectiveness.
5 Likes
What Indian pharmacy do you use? And how do you make direct contact with them? I find India mart to be very confusing.
1 Like
You can skip Indiamart.com now, just go to our page with the list of reliable online pharmacies
4 Likes
I agree but for me, this has been a learning process with bumps in the road.
3 Likes
Since we can increase the pH of the stomach with food, maybe simply taking rapa powder capsule with a meal would avoid the low pH problem without even the need for enteric caps?
“In the fasted state, the median gastric pH was 1.7 and the median duodenal pH was 6.1. When the meal was administered the gastric pH climbed briefly to a median peak value of 6.7, then declined gradually back to the fasted state value over a period of less than 2 hr.”
Upper gastrointestinal (GI) pH in young, healthy men and women - PubMed.
1 Like
We have no idea what ph is associated with “lesser” (if any less) first pass metabolism of Rapamycin in stomach and intestinal tract. So this would be a total crap shoot.
How would you even be able to track this intervention, unless you have well controlled dietary/dosing and Sirolimus blood pharmacokinetic results?
If you really want to bypass this highly variable variable, just take grapefruit juice to give yourself a boost. Unless someone can find a truly proven efficacy enteric.
2 Likes
It’s all a crap shoot without the data. Just saying, if Matt K claims the bioavailability is low due to acidic pH in the stomach, then simply taking it after a meal might level the playing field (Rx tabs vs compounded caps). Yes, we need data for sure.
Getting ahold of the study MK mentioned showing 4-fold reduction in bioavailability of compounded rapa would be a good start, but I’ve never even seen an abstract for it.
1 Like
And a high fat meal, increases by approx 30% apparently. If cost isn’t an issue, you can of course increase dose.
1 Like
At this point I’d just like my 8 year old dog to be getting the most out of his compounded rapa Rx, but there’s just no way to know. I think it’s time to start importing the tablets for him myself
1 Like
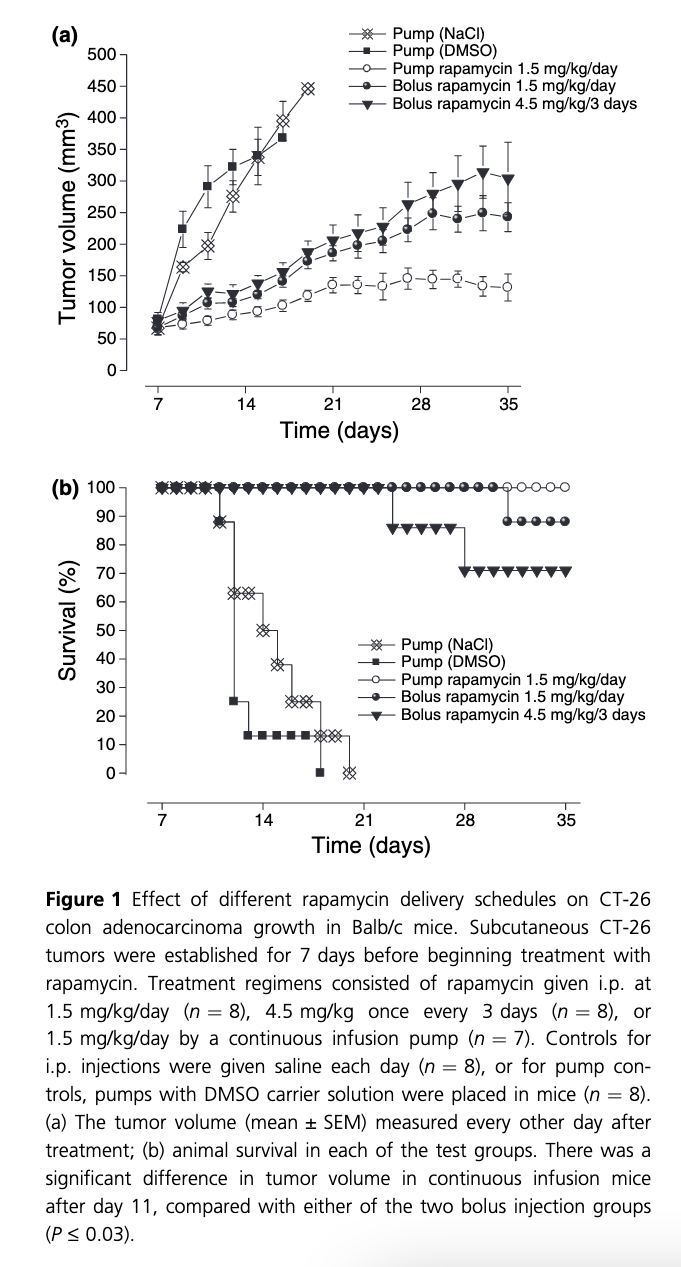
Here is an old (2004) and interesting study on dosing protocols on an angiogenic cancer mouse model.
Dosing of rapamycin is CRITICAL to achieve an optimal antiangiogenic effect against cancer
https://onlinelibrary.wiley.com/doi/epdf/10.1111/j.1432-2277.2004.00026.x
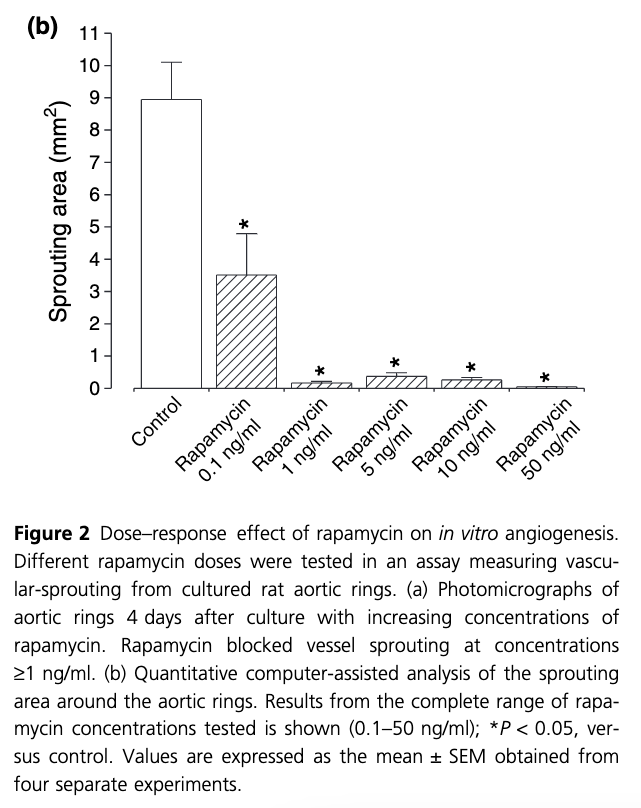
“Rapamycin has antiangiogenic activity against tumors. This has been discussed while addressing the problem of cancer in organ transplantation. Here we investigated effective dosing schedules against tumors and angiogenesis. Growth of established CT-26 colon adenocarcinoma tumors was measured in Balb/cmice treated with total equivalent rapamycin doses (1.5 mg/kg/day) given once a day, once every 3 days, or by continuous infusion. Tumors were MOST inhibited with continuous rapamycin infusion, and LESS BY BOLUS dosing. Interestingly, however, continuous dosing produced the lowest rapamycin blood levels(15 ng/ml). As rapamycin sensitive p70S6-kinase intracellular signaling is critical for angiogenesis, p70S6-kinase activation was measured in endothelialcells by Western blotting. Maximal p70S6-kinase inhibition occurred from1–5 ng/ml rapamycin. These same rapamycin concentrations optimally blocked vessel-sprouting from cultured aortic rings. Therefore, low-level rapamycin dosing most effectively controls tumors in mice. Importantly, antiangiogenic rapamycin levels are compatible with immunosuppressive doses, supporting its potential use in transplant patients with cancer”
Rapamycin treatment (ME: interesting, no dietary delivery) was initiated for the remainder of the experimental period under three different dosing schedules that delivered the same total amount of drug over the test period:
(i)1.5 mg/kg/day, intraperitoneally (i.p.)
(ii) 4.5 mg/kg once every 3 days i.p.,
(iii) 1.5 mg/kg/day by continuous infusion using an i.p. placed Alzet pump
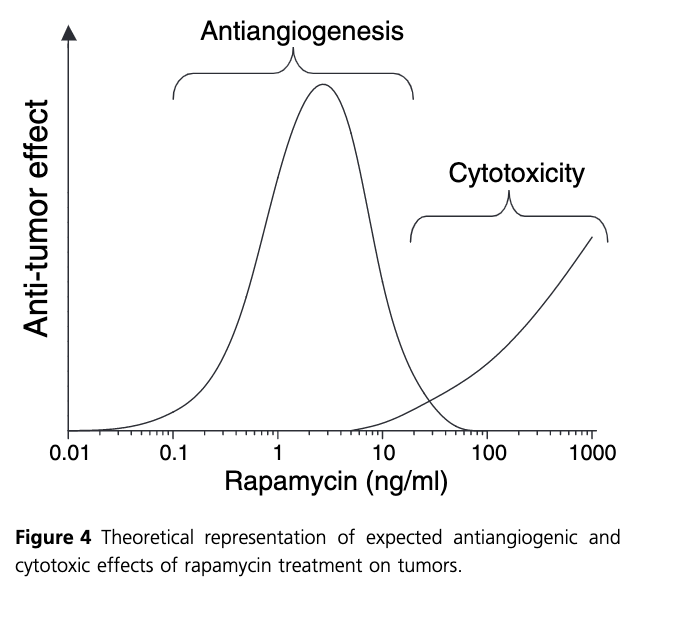
Taken together, we suggest that the effectiveness of rapamycin as an anticancer agent falls into two primary dose ranges, where low ng/ml concentrations of drug produce a potent antiangiogenic or potential anti-proliferative effect, and higher doses which can serve to have a direct cytotoxic effect on tumor cells (Fig. 4). Importantly, with regard to the use of the drug in trans-plant patients, the antiangiogenic dosing profile of rapamycin appears most compatible with normal immunosuppressive therapy.
Finally, it is interesting to consider the observation that continuous delivery of rapamycin provided the most effective in vivo treatment regimen.
This finding is similar to what has been observed with other known antiangiogenic agents, where low-level continuous-delivery methods induce the greatest anti-tumor effect [17–19]. The advantage of this type of therapy is that side effects tend to be low, making it possible to use this approach over along period of time to maintain constant ‘pressure’ against tumor expansion. It is notable that as antiangio-genic effects are directed against normal vessel cells, and not cancer cells, drug resistance to this form of therapy is less likely.
However, an antiangiogenic approach to tumor therapy is not without pitfalls. In particular, if the antiangiogenic agent is not also cytotoxic at the concentrations used, nests of cancer cells not large enough to require angiogenesis will continue to exist"
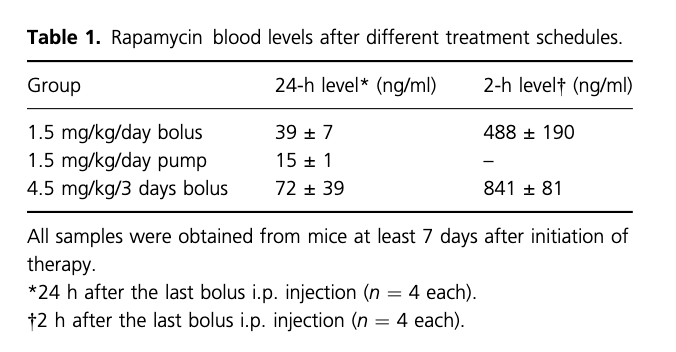
Surprised at the significant effects of the dosing protocols. The high dose every 3 days produced the poorest result compared to constant LOWER dosing? Namely, higher peak and higher likely trough. No measurements of TOR1 or TOR2 blunting, would have been very beneficial.
Meaning for translation in humans? Take rapamycin smaller doses higher frequency for lower peaks/trough, vs higher doses spaced father apart but more side effects? How about taking Everolimus, with shorter half life, smaller doses more frequently? Perhaps more potency, less side effects? Or just maintain a MIN trough level, however the rapalog/modality, but without side effects? And which side effects acceptable? Minor and/or lipid/CBC dysregulation?
I wish we had a readily available assay for mTOR inhibition: “70S6-kinase:rapamycin inhibits this signaling pathway because mTOR, which is blocked by rapamycin, is an upstream regulator of p70S6-kinase. Phosphorylation at the Thr389 site correlates with p70S6-kinase activity”
These findings could be a metabolism translation issue…mice have super high metabolism (ie cancer proliferation), and clear rapamycin very quickly, so any “gap” in rapamycin gives cancer cells a chance to proliferate (1). But even transient treatment of mice with rapamycin mid life (albeit continuous), can increase lifespan 60% (MK, 2016)
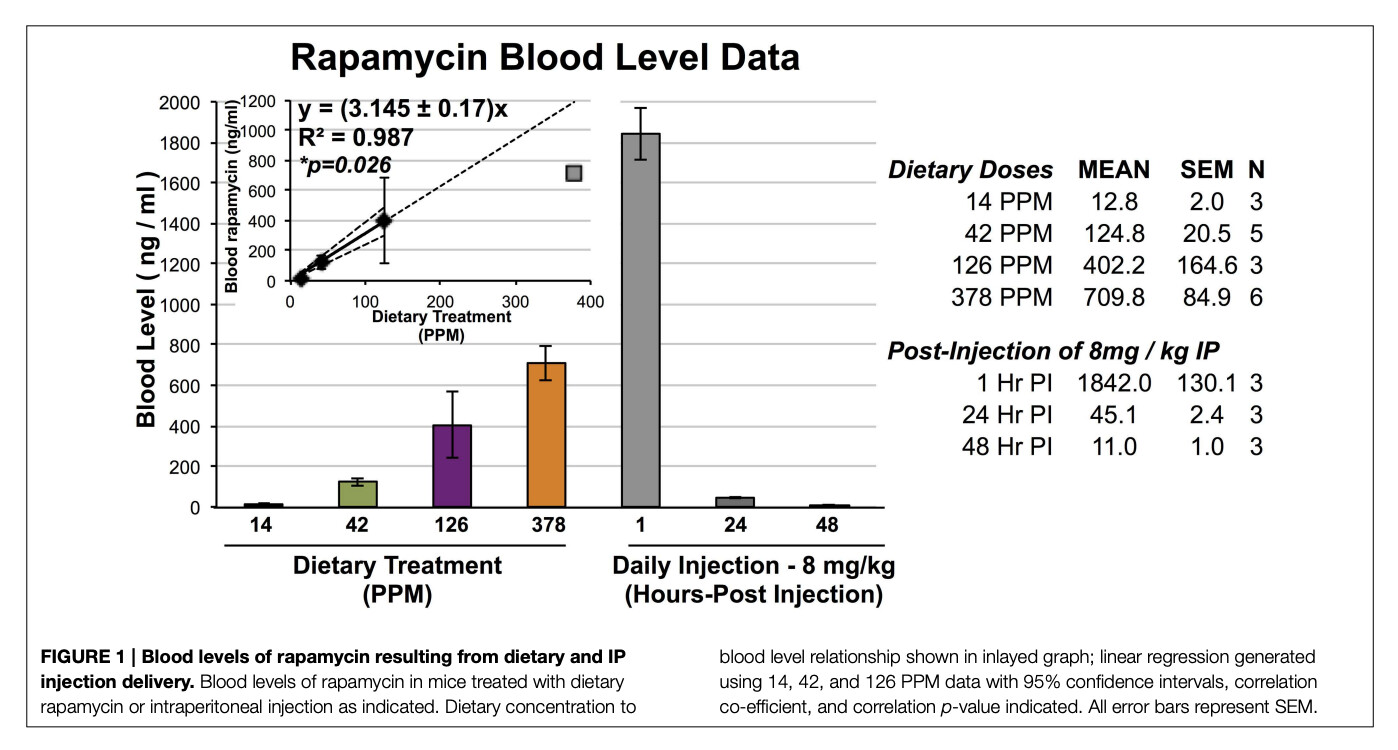
(1) Blood levels of rapamycin in IP injected mice goes from 1800 ng/L to 45 ng/L in 24 hrs.
An MK paper (2016)…6 YEARS AGO, he postulates about rapamycin regimen, dose, formulation
Rapamycin in aging and disease: maximizing efficacy while minimizing side effects
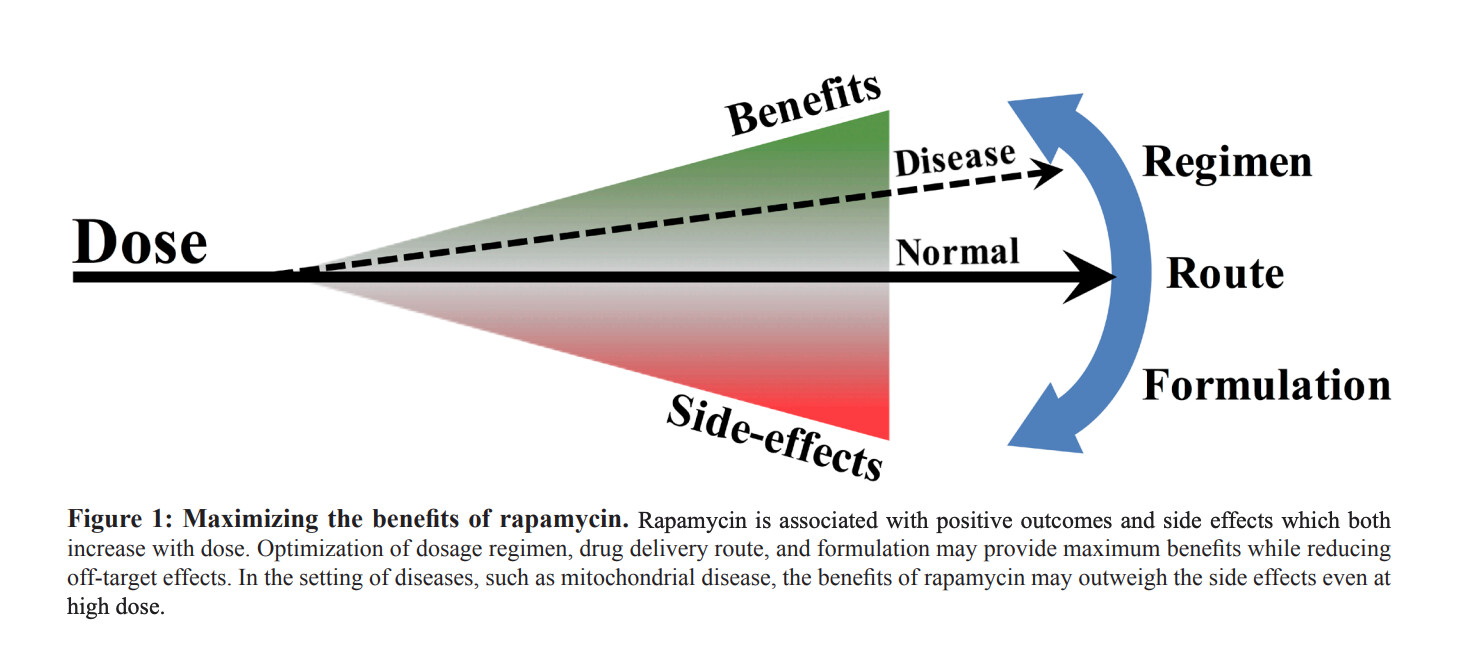
“Moving forward, we believe an emphasis should be placed on understanding how to achieve maximal efficacy from rapamycin treatment while minimizing side effects. While eRAPA and injected rapamycin are not directly comparable, as the delivery methods will have different pharmacokinetic parameters and may result in dramatically different tissue distributions, these results provide an initial foray into examination of dosing and delivery of rapamycin in a preclinical model of a medically relevant class of disease”
Yet what has changed, what have we learned in human translation since then? Pretty much nada…simple oral dosing to “max tolerable side effects”, and we don’t even know which side effects are acceptable long term?
“dramatically different tissue distributions”…indeed, but as yet unexplored.
We have no readily available tissue or blood or other assays for TOR or p70S6-kinase, or fully validated/translatable epigenetic aging, one of Peter Attia’s rapamycin concerns…“we have no good clinical biomarker”
Although they did measure an mTOR signal in the seminal cancer/rapamycin/GFJ study: “mTOR phosphorylates p70S6 kinase (p70S6K) at threonine 389 which most closely correlates with activity in vivo(23). p70S6K phosphorylation at Thr389 was measured in peripheral blood lymphocytes (PBL) as a potential biomarker of rapamycin activity. Only subjects in the sirolimus alone study underwent determination of phosphorylated p70S6K”
6 Likes
Good stuff MAC. Thanks.
I like the low dose prevent angiogenesis and reduce cell proliferation approach. Granted, it may not have the cytotoxicity, but no metastasis without angiogenesis.
I sort of like the everolimus short half life twice a week regimen. I’m still not clear on its affect on TOR 2.
2 Likes
Both of these rapalogs will definitively will trigger TOR2 disruption with sufficient high dose and chronic dosing, well documented. But Everolimus, mechanistically, does have a higher affinity for TOR2.
Everolimus “might” offer a superior different dose/AUC/side effect tradeoff. The Mannick study of Everolimus (2014), showed that 0.5mg/day was well tolerated.
From a “brief” scan, it appears everolimus might confer fewer side effects (CBC, lipids), but would have to be careful to compare equal AUC/potency. Everolimus requires approx 2X the dose of sirolimus to achieve similar trough.
I am taking a deeper comparison, will post something on the Everolimus vs Sirolimus topic thread.
Certainly coming off patent and being very low cost compared to Rapamycin makes a close look worthwhile.
3 Likes
Do I have this right?
Everolimus
Pros: short half life
may be able to dose it higher and even twice a week
fewer side effects ( lipids,glucose)
Cons: need a higher dose than rapa
hits TOR 2 even harder
a little more expensive
the longevity effects haven’t been studied as much as rapa
2 Likes
Would agree with what you’ve briefly summarized. Also some indication Everolimus better at crossing BBB. Is perhaps taking more frequently a con? The harder TOR2 perhaps at very high doses…cancer/transplant, not at lower doses? Dysregulating TOR2 would more amplify side effects, including TOR2 specific insulin signalling/hyperglycemia. Of the comparative studies, not many report higher hyperglycemia with Everolimus…but similar range of side effects as rapamycin.
Re cost, I was quoted by an Indian supplier $0.7/mg for Rapamycin ($7 for 10 x 1mg/tabs), and Everolimus $.95/mg ($95 for 10 x 10mg tabs). If you’ve got to take 2X the Everolimus dose for same potency, then effectively $1.80/mg vs $0.70/mg, 250% more. On a total cost basis over a year if it really increased lifespan…meaningless.
It’s slightly better side effects profile, that could be the lure/incentive.
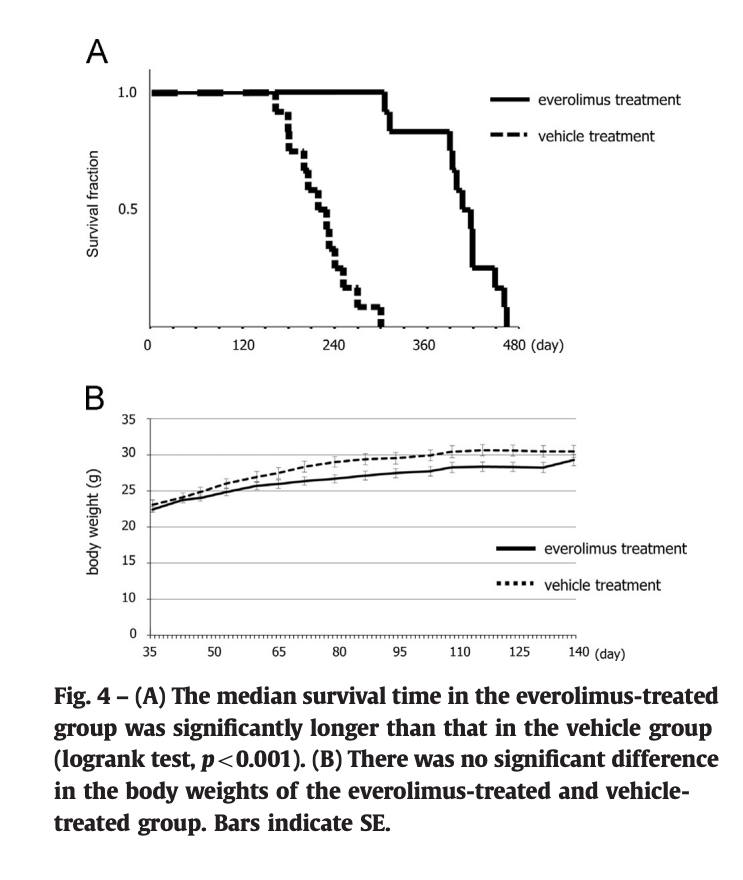
I’ve only found a few longevity studies on Everolimus. One showed an increased lifespan of 85% (1). Everolimus works so VERY similarly mechanistically to rapamycin, and according to Dr B, would deliver “equal lifespan enhancements” to Rapamycin, potency equivalent. More clinical trials seem to be using Everolimus and Tacromilus recently over rapamycin…better side effect profile as a chemo/immuno adjuvant. And in reality, rapamcyin has a poor record in existing cancer trials in terms of cancer mitigation or transplant rejection.
https://sci-hub.se/https://doi.org/10.1016/j.yexcr.2014.04.012
2 Likes
The article also says that c/w rapamycin, everolimus stimulates mitochondrial oxidation. What am I missing here? Do they mean increased mitochondrial stress from reactive oxygen species?
The increase in propensity for TOR 2 inhibition is also concerning.
1 Like
Perhaps they mean that everolimus increases mitochondrial oxidative capacity. That would be a positive.
1 Like
The reference:
“Shows that everolimus alone has the potential to stimulate mitochondrial energy metabolism, while sirolimus has negative effects”
1 Like