Thanks, do you have a brand you prefer?
Not really. I just make sure it is not Chinese. Recently I ordered this, because I saw it on BJ blueprint…
Btw I prefer chlorella because it is a sweet water algae / spirulina is sea water algae and sea water is more easily contaminated…
1 Like
I use spirulina by Microingredients, but not sure if it’s a good choice. It’s organic.
I have been happy with their products and they claim to be third-party tested and passed for heavy metals.
1 Like
When were these blood sirolimus levels in the mice in those longevity studies measured? Do you know if they measured them in the early day time (before the mice go to sleep) or in the evening when they have eaten food all night?
You asked about the time of day of blood sirolimus level testing in the mouse studies… I don’t have that information, I don’t think they even mention that in the research papers… you’d have to talk to the people who did the studies.
In most of these studies though - the mice are feed ad-libitum and the rapamycin is mixed in with their food at a prespecified level (e.g. 14ppm). I believe I’ve heard that mice tend to eat randomly throughout the day, so I would suspect that the sampling timing over the months of the study would equal out to provide an approximate typical range… and that is what they are reporting.
5 Likes
Yes, I think the levels are probably some sort of steady state levels with the timing of the blood tests not having much of an influence on the measured levels because mice tend to eat randomly not just during the day like humans, so their intake is more constant over 24 hours than that of humans.
2 Likes
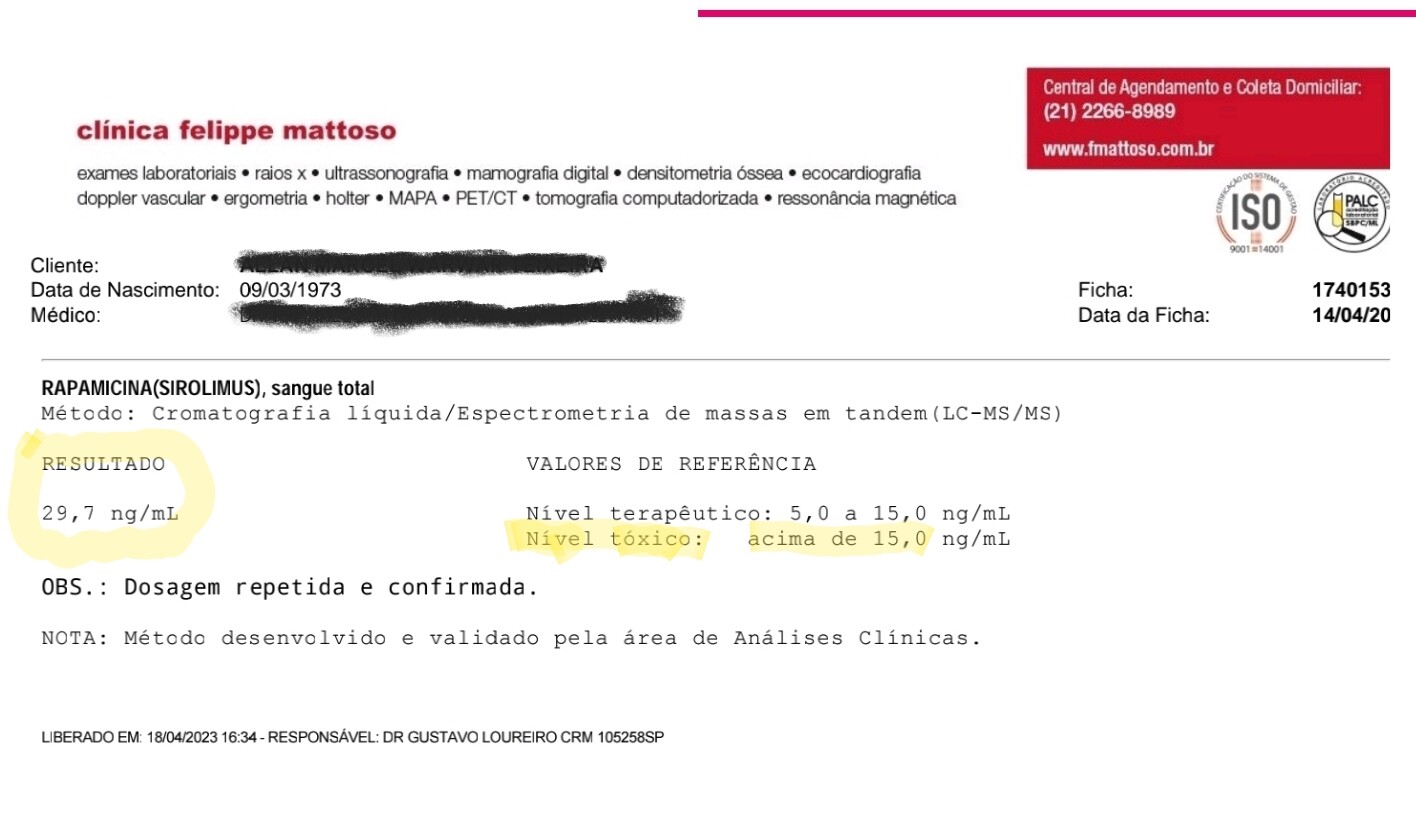
Hello, I started my rapamycin journey a few months ago. I have been on 6mg of Rapacan for 4 weeks now. I have had mild headaches. I got tested my rapamycin levels 2:10 after taking the medication with a fatty meal (3 eggs and 50g of cheese). My labs showed an almost 30 ng/dL level! It’s scary, since by laboratory standards this level is twice as toxic! What do you guys think about this? My blood tests are fine, apart from the hyperlipidemia, induced by the ketogenic diet. In that regard, rapamycin had zero influence on my lipid profile. My insulin dropped from 3 to 2. It seems that low insulin levels are associated with less LDL receptors in the liver, which causes cholesterol to rise. This does not scare me, as I follow another group of people who have a lipid profile very similar to mine and, until now, they have not experienced progression in atherosclerosis, as I have not. With rapa, my CRP dropped from 0.06 to 0.03, which is the lowest measurement I’ve had since I started tracking this marker. But I would really like to hear what you guys think about 30ng/mL after 2:10 hours of taking the medication: is this too much? Looking at the charts here, I have the impression that it doesn’t, but I need to hear more people about it.
3 Likes
Hi - and welcome to the forums. Thanks for posting the detailed information.
Just so you understand better - the usual blood sirolimus tests and range is really designed for the organ transplant patients who take 1mg to 5mg per day, and so the test is designed to measure the typical daily level of sirolimus in their blood. So the therapeutic rage of 5ng/ML to 15ng/ML is only with regard to organ transplant patients and this is thought to be best for them.
When you go above that level - it isn’t toxic, its just high. You can see the blood / sirolimus levels that are typically seen in all the animal studies where they are seeing longevity increases of up to 30% and you’ll see the range is much, much higher than the therapeutic values used in organ transplant patients - see here: What is the Rapamycin Dose / Dosage for Anti-Aging or Longevity? - #218 by RapAdmin
Peak levels of sirolimus in blood isn’t really that meaningful. Really its the AUC (area under the curve) over the long term that matters. And here - it seems to be a balancing act, the higher the better (from the longevity studies we’ve seen so far), but the higher you go the greater the risk of side effects and immune system supression (all the mouse studies have the mice in pathogen-free lab environments that are very different from the environments we live in).
Rapamycin was approved in 2006, and has been used safely for almost 20 yrs. There is even a study paper on “acute Sirolimus overdose” cases of over 100mg dosing, all without any serious permanent effects. See below:
If you haven’t already, you should read the full thread here to better understand blood sirolimus level testing: How to get a Rapamycin (sirolimus) Blood Level Test
9 Likes
Does “2:10” mean two hours and ten minutes after your meal? The reference range is for your trough level, 24 hours after your last dose. And the high end of that range isn’t the “toxic” dose — just outside the reference range.
I agree entirely with RapAdmin’s additional comments.
You have that last bit backward. Low insulin levels lead to low circulating LDL-C, all else being equal, because insulin upregulates PCSK9 expression in the liver, leading to increased LDL receptor degradation.
Normally, when people have elevated LDL-C on ketogenic diets, it’s because they’re eating more saturated fat.
When you say “they have not experienced progression in atherosclerosis, as I have not,” what are you basing that on? If (like a lot of people in the keto community) you’re basing it on a coronary calcium score, you’re making a grave mistake, for reasons explained here:

“About one-fourth to one-third of the total incident cardiovascular disease (CVD) events (Table) occur in those with a CAC of zero, despite some use of lipid-lowering therapy at baseline or during follow-up (in MESA [Multi-Ethnic Study of Atherosclerosis] ≈15% at baseline and 44% during follow-up).”
https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.119.045026
Interesting, but not a reason to ignore a high LDL-C. LDL-C is causal for atherosclerosis; CRP is just a downstream marker of atherosclerosis-associated inflammation.
4 Likes
Just to clarify, you are taking 6mg / week, not 6mg / day correct?
29.7 ng/ml does seem a bit high for a 6mg dose. Not dangerous but I’m a bit surprised it is that high.
4 Likes
Yes a level of 30 ng/mL sounds very high. But it doesn’t give you any details other than showing that you got a high level. It makes a lot more sense to measure rapamycin levels at 24 or 48 hours after dosing. That will give you an estimate of how much you are absorbing. Trying to catch peak levels a few hours after dosing is kind of pointless IMO because you have no idea how close to the peak you were at the time of measurement. Testing when levels will have stabilized a bit will give you a much better idea of where you stand. Levels taken 24 or 48 hours after dosing can be much better compared to those reached at the same time at different doses or for different people.
3 Likes
I follow the progression of atherosclerosis with CMIT. After 2 years of LDL close to 200, my carotids are the same. I have a mild atherosclerosis in one of the coronary arteries, detected by CT angioscan, and also in one of the carotids, by ultrasound. According to my cardiologist, it hasn’t appeared in recent years, when my LDL has skyrocketed on the keto diet. It took many years. My CAC score is zero and my plaques are mild and stable. That’s more or less according to my age bracket, I think.
1 Like
I don’t necessarily agree. I think that pharmacology of rapamycin is really well researched as it is on the market for almost 25 years and all studies show that is relatively poorly absorbed (∼14%) and has fast absorption and reaches maximal blood level concentration in 1-2 hours. Since it has a slow half life (∼63h) measuring at 2 or 2.30h would not make a big statistical difference. I personally would not measure before 2h after dosing after doing some research (studies I found generally measure at 0.30, 1h, 2h, 4h, 8h and 24h and 48h). Measuring at 24 and 48 hours would only give you the idea of how rapamycin is being metabolized and give you more information on half life… since tMax for longevity is not established is more of a personal interest to know it and more important insight is trough value just before the next dose, which should be almost zero to keep you immune system running and not suppressed all the time.
4 Likes
Except it does make a big difference. Look at the figure from PMID: 11034258. The initial drop from the peak is way faster than a half-life of 63 would indicate, and the timing of the peak varies significantly, so the values in the first hour or two are all over the place and hard to compare. It’s only after about 48 hours when the drop is gradual in line with a half-life of 63 hours. The values in the figure at 24 and 48 hours differ in a pretty linear way with the dose given so those are good time points to measure for bioavailability comparison. Besides at that time it hasn’t even been one half-life since the peak so the rate of metabolism shouldn’t have a large effect on the values there. The values at that time are more a function of the rate of absorption. The metabolism rate would be more apparent at a much longer time after dosing, which is why measuring at something like 96 hours would be good to see how fast one is metabolizing it.
1 Like
That much is true. I agree it’s very important to know that to determine how long of a space between doses is optimal for each individual. However I think it’s also very important to figure out where each individual stands in terms of bioavailability. As an example, all those longevity leaders that are taking 6 mg weekly, some of them are getting 2-3 times more than others due to increased absorption. You can’t compare yourself to other people if you don’t know your absorption. The only way to do that is with blood tests, and for that you need to measure rapamycin in the blood at a time point where it is relatively stable where the level reflects the absorption of rapamycin rather than the timing (if you measure too close to the peak) or the metabolism (if you measure a few half-lives after the dose). If anyone has a better suggestion to compare bioavailability with blood tests please share.
1 Like
I don’t think that Dr. Green, Dr. Attia or other experts taking or prescribing Rapamycin frequently measure or rely on the blood levels. As far as I understand, many of them watch for an appearance of side effects indicating that the dose is too high- not too scientific.
2 Likes
Yes i suspect you are right. Most of them prescribe based on some simple protocol like 3mg for light people, 6mg for average weight people, and 8mg if you are older or heavier than average.
6 Likes
Yes I doubt they rely on blood levels. But that’s because they don’t have much to compare them too, in addition to the fact that it’s not so easy to get such tests and get people to take them. If they actually would ask all their clients that can to take blood tests and would collect the data from them, then such test results would become much more useful as a means to compare bioavailability between individuals relative to the average person.
The reason they usually watch for an appearance of side effects is probably that the mouse studies have found the greatest benefits at the highest doses and so far we haven’t found the ceiling and given how high the doses given in the mouse studies are it makes sense to aim for something that is as high as people tolerate without any side effects.
4 Likes
If you haven’t read it already, checked out the thread at
2 Likes